实用医学杂志 ›› 2025, Vol. 41 ›› Issue (14): 2143-2151.doi: 10.3969/j.issn.1006-5725.2025.14.004
丘海,归奕飞( ),刘媛
),刘媛
Hai QIU,Yifei GUI(),Yuan. LIU
摘要:
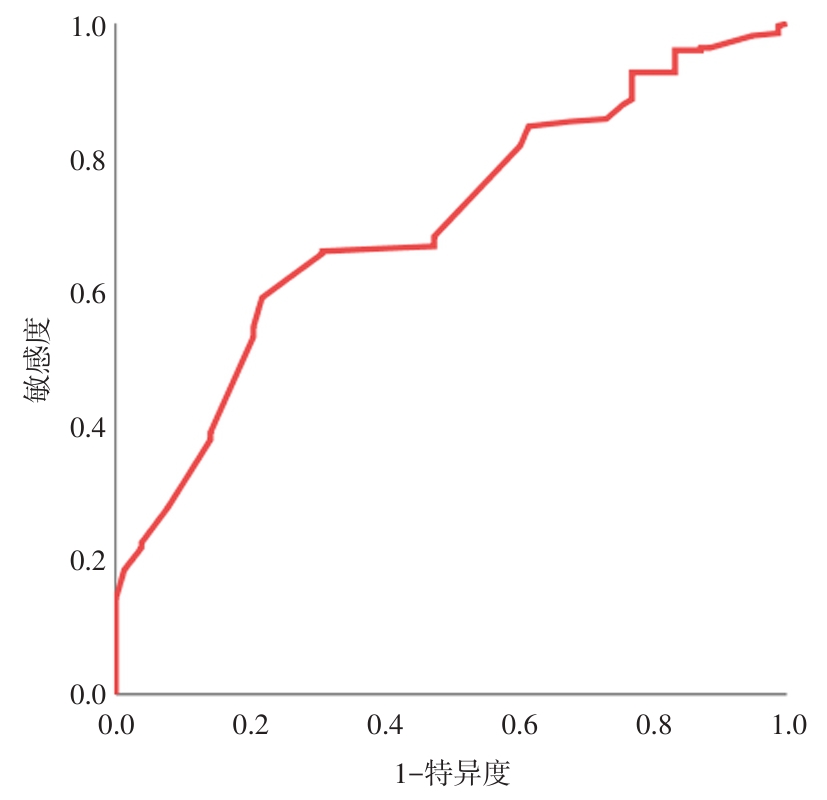
目的 建立多因素预测模型,筛选术前腋窝超声(axillary ultrasound, AUS)正常的临床T1—2N0患者发生前哨淋巴结(sentinel lymph node, SLN)转移的高危人群,为腋窝分期的个体化管理策略提供参考。 方法 回顾性分析柳州市工人医院普通外科四病区(乳腺)2018年1月至2023年12月收治的427例浸润性乳腺癌患者的临床病理资料及超声检查数据,进行单因素相关性分析和多因素logistic回归分析,从而确定影响SLN转移的独立危险因素,然后采用ROC曲线评估模型的准确性和预测价值。 结果 本研究共纳入427例术前AUS评估正常的临床T1—2 N0女性乳腺癌患者,其中47例(11.0%)患者探及正常腋窝淋巴结,余380例(89.0%)患者腋窝超声均未见报告肿大淋巴结。78例(18.3%)患者经术后病理证实SLN转移,单因素分析显示SLN转移与雌激素受体(estrogen receptor, ER)、肿瘤最大径、肿瘤位置、脉管癌栓和神经侵犯相关(P < 0.05),而多因素分析显示肿瘤位于外上象限(OR = 4.118, 95%CI: 1.349 ~ 12.571)、肿瘤最大径> 2 cm(OR = 2.246, 95%CI: 1.252 ~ 4.029)、脉管癌栓(OR = 4.477, 95%CI: 2.207 ~ 9.081)和神经侵犯(OR = 3.013, 95%CI: 1.573 ~ 5.771)是影响SLN转移的独立危险因素(P < 0.05)。超声下腋窝淋巴结的阴性或阳性、最短径、数目与SLN转移数目无关(P ≥ 0.05),而与病理淋巴结(pathological node, pN)分期有关(P < 0.05)。1 ~ 2枚SLN转移患者的超声下腋窝淋巴结的阴性或阳性、最长径、最短径、数目与ALN转移数目、pN分期变化均无关(P ≥ 0.05)。根据预测模型绘制ROC曲线的AUC值为0.702(95%CI: 0.651 ~ 0.749, P < 0.000 1),该模型预测的敏感度为78.21%,特异度为59.12%。 结论 肿瘤位于外上象限、肿瘤最大径> 2 cm、脉管癌栓和神经侵犯是术前AUS正常的临床T1-T2N0女性乳腺癌患者发生SLN转移的显著危险因素。另外,单从对pN分期的影响来说,对于cT1—2 N0且1 ~ 2枚SLN转移的绝大部分患者,豁免腋窝淋巴结清扫术(ALND)是可行的,但尚不能从超声腋窝淋巴结的特征预测与腋窝淋巴结(ALN)转移、pN分期的相关性。
中图分类号: