实用医学杂志 ›› 2025, Vol. 41 ›› Issue (14): 2138-2142.doi: 10.3969/j.issn.1006-5725.2025.14.003
胡作怀,付建东,李小芳,姚欣悦,赵宾,晏涑,何思思( )
)
Zuohuai HU,Jiandong FU,Xiaofang LI,Xinyue YAO,Bin ZHAO,Shu YAN,Sisi. HE()
摘要:
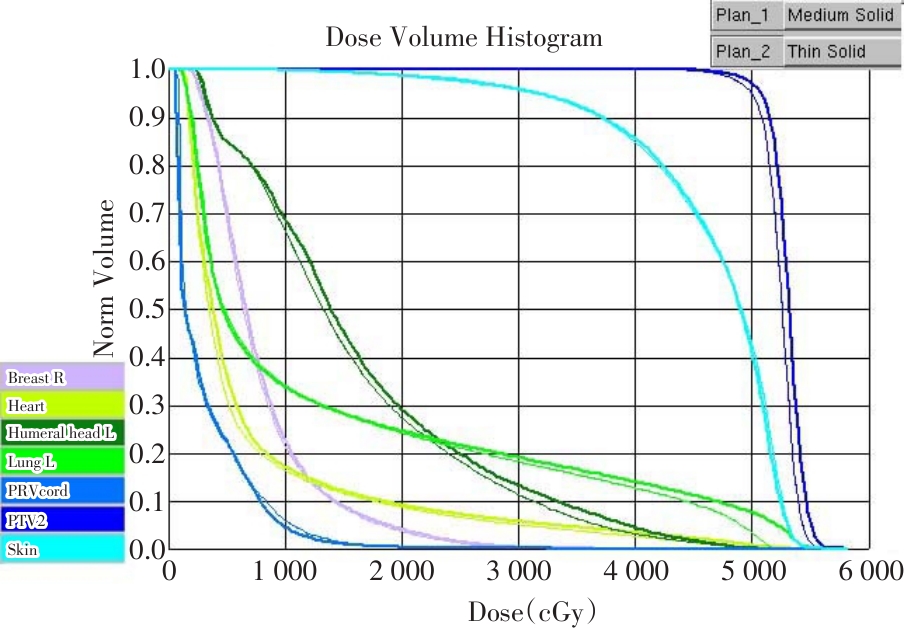
目的 探讨组织补偿膜(Bolus)不同使用方式对乳腺癌根治术后胸壁皮肤剂量的影响。 方法 回顾性分析2023年1月至2025年3月间,医院乳腺癌根治术后需胸壁放疗的女性患者60例,用Pinnacle3 9.10放疗计划系统(TPS)为每例患者设计2个VMAT双半弧放疗计划,靶区处方剂量为50 Gy/2 Gy/25 f。Plan1前半程添加Bolus优化放疗15次,后半程10次去掉Bolus,不做计划优化,保持前半程优化计划的子野形状和剂量权重,仅做剂量计算,将有无Bolus的计划组合放疗;Plan2前半程添加Bolus优化放疗15次,后半程10次去掉Bolus,重新做计划优化,将两次优化计划组合放疗。用SPSS 29.0软件对两组计划的数据做配对样本t检验。 结果 皮肤Dmean、V52.5、V55,心脏Dmean、V5、V30、V40,患侧肺Dmean、V5、V20,脊髓外扩Dmean、Dmax,健侧乳房Dmean、V5、V10,患侧肱骨头Dmean、V30,PTV的Dmean、V50、V55、D2%、D98%、CI、MU,差异均有统计学意义(P < 0.05),且靶区层面剂量分布,DVH图明显不同;而PTV的HI(P = 0.125),差异无统计学意义。 结论 15次Bolus与10次不加Bolus的两个优化计划组合,真实反映了计划靶区与危及器官的剂量分布,能更好地保护患者胸壁皮肤。
中图分类号: