

The Journal of Practical Medicine ›› 2026, Vol. 42 ›› Issue (1): 21-28.doi: 10.3969/j.issn.1006-5725.2026.01.003
• Oncology: Diagnosis, Treatment and Prevention • Previous Articles Next Articles
Zhen ZHANG,Donghao WANG,Yang LV( )
)
Received:2025-09-26
Online:2026-01-10
Published:2026-01-14
Contact:
Yang LV
E-mail:lyuyang@tjmuch.com
CLC Number:
Zhen ZHANG,Donghao WANG,Yang LV. Diagnostic value of skeletal muscle ultrasonography combined with bioelectrical impedance analysis in acquired weakness in the intensive care unit of patients with tumor sepsis[J]. The Journal of Practical Medicine, 2026, 42(1): 21-28.
Fig.1
Ultrasonic measurements of muscle cross-sectional area and thickness"
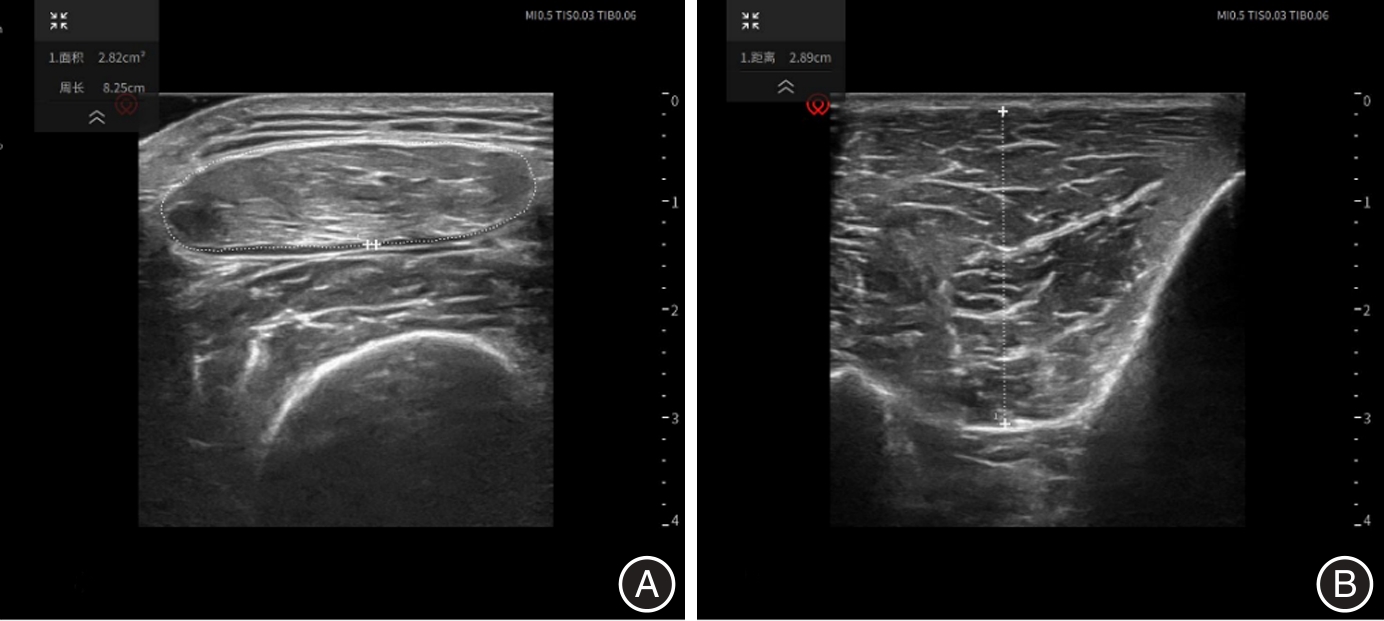

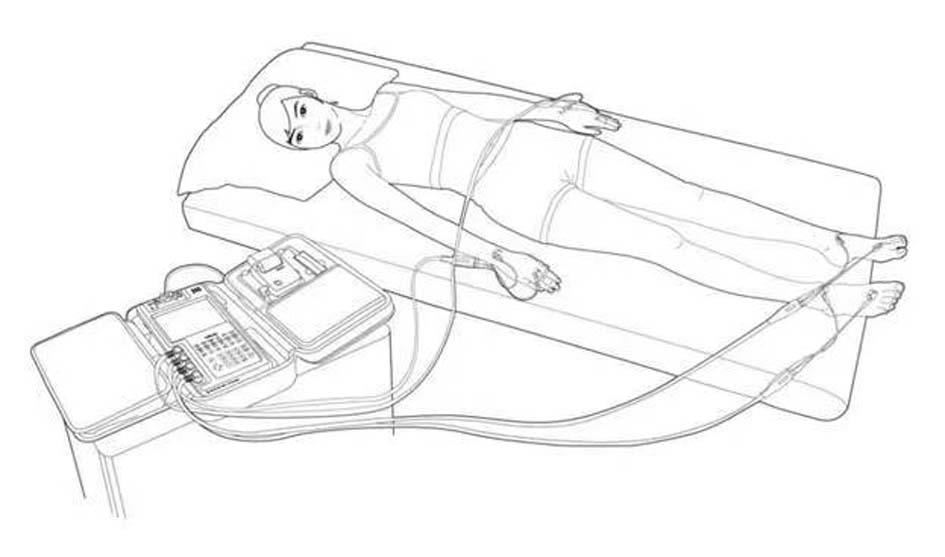
Fig.2
Bioelectrical impedance analysis"
Tab.1
Comparison of clinical data between patients in the No ICU-AW group and the ICU-AW group"
| 变量 | No ICU-AW组(n = 75) | ICU-AW组(n = 41) | t/χ2值 | P值 |
|---|---|---|---|---|
| 性别 | 0.511 | 0.475 | ||
| 男 | 70(81.4) | 38(86.4) | ||
| 女 | 16(18.6) | 6(13.6) | ||
| 年龄(x ± s)/岁 | 66.43 ± 8.45 | 66.31 ± 10.03 | -0.047 | 0.962 |
| BMI(x ± s)/(kg/cm2) | 23.54 ± 4.39 | 23.97 ± 2.91 | 0.362 | 0.719 |
| 肿瘤类型 | 2.457 | 0.483 | ||
| 食管癌 | 28(32.6) | 19(43.2) | ||
| 胃癌 | 25(29.1) | 13(29.5) | ||
| 结肠癌 | 15(17.4) | 7(15.9) | ||
| 其他 | 18(20.9) | 5(11.4) | ||
| 感染部位 | 3.295 | 0.348 | ||
| 腹腔感染 | 32(37.2) | 15(34.1) | ||
| 肺炎 | 28(32.6) | 19(43.2) | ||
| 胸腔感染 | 17(19.8) | 4(9.1) | ||
| 其他 | 9(10.4) | 6(13.6) | ||
| 使用血管活性药物 | 29(33.7) | 32(72.7) | 17.782 | < 0.001 |
| 使用机械通气 | 35(40.7) | 30(68.2) | 8.795 | 0.003 |
| 使用镇痛镇静 | 62(72.1) | 37(84.1) | 2.307 | 0.129 |
| 乳酸(x ± s)/(mmol/L) | 1.90 ± 0.79 | 2.13 ± 1.32 | 0.813 | 0.419 |
| NRS2002评分(x ± s)/分 | 4.13 ± 1.02 | 4.42 ± 1.44 | 0.328 | 0.637 |
Tab.2
Comparison of various indicators between patients in the No ICU-AW group and the ICU-AW groupat different treatment time points"
| 指标 | No ICU-AW组(n = 75) | ICU-AW 组(n = 41) | t值 | P值 | 指标 | No ICU-AW组(n = 75) | ICU-AW 组(n = 41) | t值 | P值 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 股直肌横截面积/cm2 | SOFA 评分 | |||||||||
| D0h | 4.37 ± 0.74 | 4.36 ± 0.87 | 0.081 | 0.936 | D0h | 5.44 ± 2.64 | 8.27 ± 3.41 | -4.965 | < 0.001 | |
| D72h | 4.19 ± 0.78 | 3.87 ± 0.81 | 2.122 | 0.036 | D72h | 3.05 ± 2.23 | 4.02 ± 3.62 | -1.789 | 0.076 | |
| t值 | 6.872 | 13.250 | t值 | 8.848 | 9.768 | |||||
| P′值 | < 0.001 | < 0.001 | P′值 | < 0.001 | < 0.001 | |||||
| 胫骨前肌厚度/cm | 全身水/L | |||||||||
| D0h | 2.19 ± 0.30 | 2.27 ± 0.34 | -1.274 | 0.205 | D0h | 37.68 ± 5.94 | 40.91 ± 6.37 | -2.732 | 0.007 | |
| D72h | 2.08 ± 0.29 | 2.04 ± 0.30 | 0.688 | 0.493 | D72h | 36.00 ± 5.70 | 36.59 ± 6.06 | -0.525 | 0.601 | |
| t值 | 6.876 | 10.117 | t值 | 8.442 | 10.552 | |||||
| P′值 | < 0.001 | < 0.001 | P′值 | < 0.001 | < 0.001 | |||||
| 骨骼肌指数/(kg/m2) | 蛋白质质量/kg | |||||||||
| D0h | 7.52 ± 1.11 | 8.21 ± 1.31 | -2.982 | 0.003 | D0h | 9.64 ± 1.52 | 10.40 ± 1.60 | -2.530 | 0.013 | |
| D72h | 7.13 ± 1.08 | 6.99 ± 1.14 | 0.663 | 0.509 | D72h | 9.27 ± 1.47 | 9.42 ± 1.52 | -0.537 | 0.592 | |
| t值 | 11.675 | 13.350 | t值 | 8.290 | 12.036 | |||||
| P′值 | < 0.001 | < 0.001 | P′值 | < 0.001 | < 0.001 | |||||
| 上臂围/cm | (细胞外水/全身水)/% | |||||||||
| D0h | 29.98 ± 2.55 | 30.70 ± 3.56 | -1.254 | 0.212 | D0h | 40.85 ± 1.12 | 41.21 ± 1.66 | -1.376 | 0.172 | |
| D72h | 29.74 ± 2.61 | 30.73 ± 5.51 | -1.316 | 0.191 | D72h | 40.36 ± 1.54 | 40.40 ± 1.23 | -0.139 | 0.890 | |
| t值 | 1.552 | -0.040 | t值 | 5.019 | 2.875 | |||||
| P′值 | 0.125 | 0.968 | P′值 | < 0.001 | 0.006 | |||||
| APACHEⅡ评分 | 相位角/° | |||||||||
| D0h | 14.11 ± 3.51 | 22.07 ± 6.93 | -8.235 | < 0.001 | D0h | 3.80 ± 0.86 | 3.42 ± 0.71 | 2.406 | 0.018 | |
| D72h | 10.15 ± 3.58 | 11.59 ± 5.21 | -1.754 | 0.082 | D72h | 4.22 ± 1.06 | 4.10 ± 0.98 | 0.567 | 0.572 | |
| t值 | 8.750 | 10.331 | t值 | -7.561 | -5.601 | |||||
| P′值 | < 0.001 | < 0.001 | P′值 | < 0.001 | < 0.001 |
Tab.3
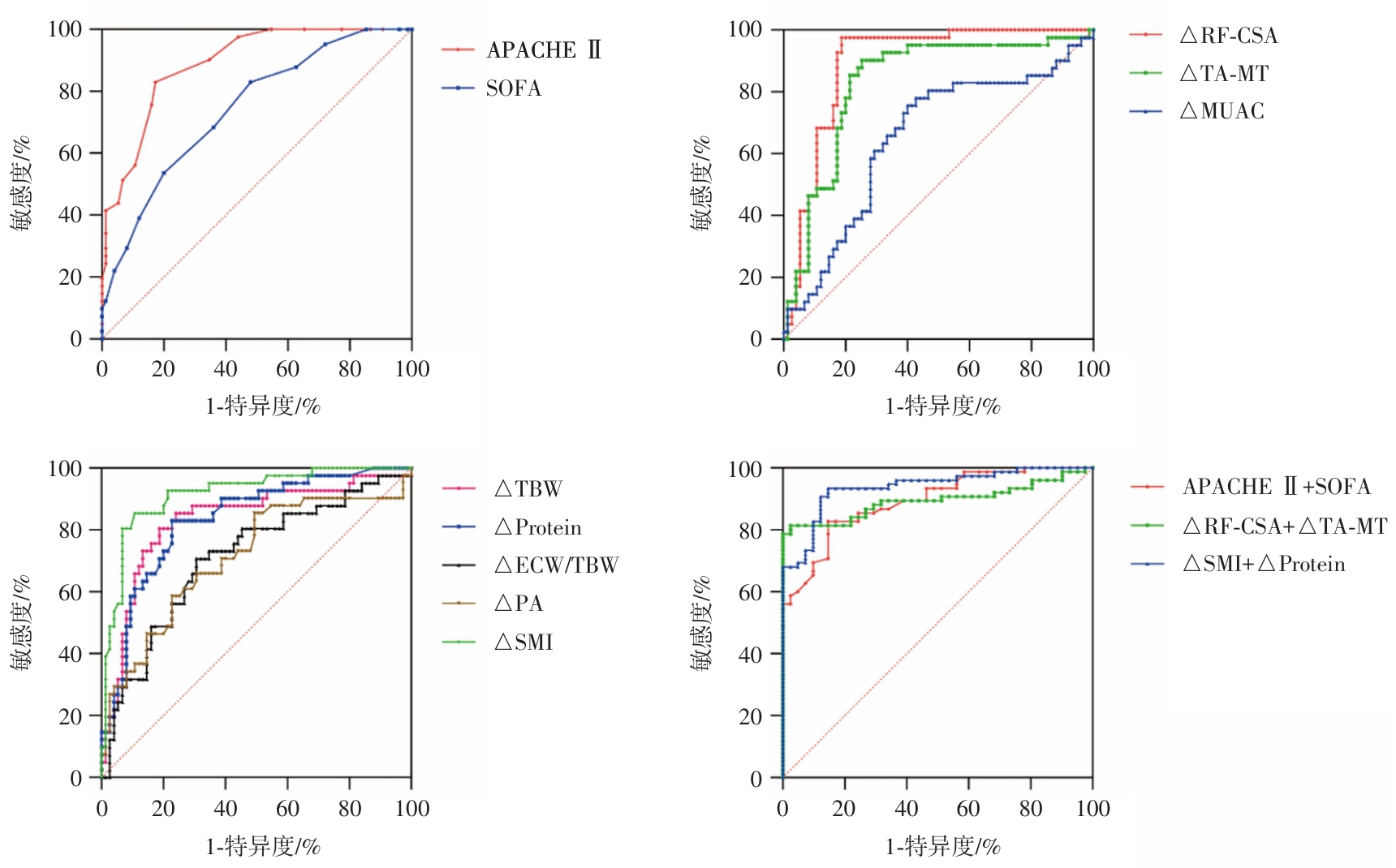
ROC curve analysis of ICU-AW in tumor patients with sepsis"
| 变量 | SE | P值 | ROC-AUC(95%CI) |
|---|---|---|---|
| △MUAC | 0.055 | 0.007 | 0.652(0.545 ~ 0.760) |
| △RF-CSA | 0.031 | < 0.001 | 0.891(0.831 ~ 0.952) |
| △TA-MT | 0.041 | < 0.001 | 0.830(0.749 ~ 0.911) |
| △SMI | 0.028 | < 0.001 | 0.916(0.862 ~ 0.971) |
| △TBW | 0.043 | < 0.001 | 0.833(0.749 ~ 0.917) |
| △ECW/TBW | 0.051 | < 0.001 | 0.711(0.610 ~ 0.811) |
| △PA | 0.053 | < 0.001 | 0.712(0.609 ~ 0.815) |
| △Protein | 0.039 | < 0.001 | 0.834(0.758 ~ 0.911) |
| APACHE II-D0h | 0.029 | < 0.001 | 0.829(0.803 ~ 0.917) |
| SOFA-D0h | 0.047 | < 0.001 | 0.743(0.651 ~ 0.834) |
| △SMI+△Protein | 0.022 | < 0.001 | 0.938(0.895 ~ 0.980) |
| △RF-CSA+△TA-MT | 0.030 | < 0.001 | 0.894(0.834 ~ 0.954) |
| APACHE Ⅱ+SOFA-D0h | 0.029 | < 0.001 | 0.842(0.806 ~ 0.918) |
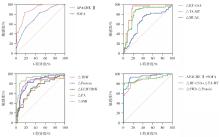
Fig.3
The predictive value of ROC curve analysis on various indicators for ICU-AW in tumor patients with sepsis"
Tab.4
Diagnostic value of various indicators for ICU-AW in tumor patients with sepsis"
| 变量 | 截断值 | 敏感度 | 特异度 | 阳性预测值 | 阴性预测值 | 约登指数 |
|---|---|---|---|---|---|---|
| △MUAC | 0.013 | 0.756 | 0.600 | 0.508 | 0.818 | 0.356 |
| △RF-CSA | 0.054 | 0.951 | 0.813 | 0.736 | 0.968 | 0.789 |
| △TA-MT | 0.053 | 0.902 | 0.760 | 0.672 | 0.934 | 0.649 |
| △SMI | 0.095 | 0.829 | 0.893 | 0.810 | 0.905 | 0.747 |
| △TBW | 0.071 | 0.805 | 0.813 | 0.702 | 0.884 | 0.618 |
| △ECW/TBW | 0.017 | 0.707 | 0.693 | 0.558 | 0.813 | 0.401 |
| △PA | 0.091 | 0.854 | 0.520 | 0.493 | 0.867 | 0.360 |
| △Protein | 0.063 | 0.805 | 0.773 | 0.660 | 0.879 | 0.603 |
| APACHE II-D0h | 16.50 | 0.829 | 0.587 | 0.523 | 0.863 | 0.656 |
| SOFA-D0h | 5.50 | 0.829 | 0.520 | 0.486 | 0.848 | 0.349 |
| △RF-CSA +△TA-MT | 0.286 | 0.976 | 0.813 | 0.741 | 0.984 | 0.789 |
| △SMI+△Protein | 0.467 | 0.854 | 0.933 | 0.875 | 0.921 | 0.787 |
| APACHE II+SOFA-D0h | 0.281 | 0.854 | 0.827 | 0.729 | 0.912 | 0.680 |
| [1] |
SOUSSI S, SHARMA D, JÜNI P, et al. Identifying clinical subtypes in sepsis-survivors with different one-year outcomes: A secondary latent class analysis of the FROG-ICU cohort[J]. Crit Care, 2022,26(1):114. doi: 10.1186/s13054-022-03972-8 .
doi: 10.1186/s13054-022-03972-8 |
| [2] |
TANAKA K, YAMADA T. Ultrasound Measurement of Septic Shock-induced Acute Skeletal Muscle Atrophy in Intensive Care Unit[J]. PM R, 2021,13(4):347-352. doi: 10.1002/pmrj.12406 .
doi: 10.1002/pmrj.12406 |
| [3] |
BORGES R C, BARBEIRO H V, BARBEIRO D F, et al. Muscle degradation, vitamin D and systemic inflammation in hospitalized septic patients[J]. J Crit Care, 2020,56:125-131. doi: 10.1016/j.jcrc.2019.12.017 .
doi: 10.1016/j.jcrc.2019.12.017 |
| [4] |
BATT J, HERRIDGE M, SANTOS C D. Mechanism of ICU-acquired weakness: Skeletal muscle loss in critical illness[J]. Intensive Care Med, 2017,43(12):1844-1846. doi: 10.1007/s00134-017-4758-4 .
doi: 10.1007/s00134-017-4758-4 |
| [5] |
MAYER K P, BASTIN M L T, MONTGOMERY-YATES A A, et al. Acute skeletal muscle wasting and dysfunction predict physical disability at hospital discharge in patients with critical illness[J]. Crit Care, 2020,24(1):637. doi: 10.1186/s13054-020-03355-x .
doi: 10.1186/s13054-020-03355-x |
| [6] |
李云婷, 李芬, 邢柏. 机械通气老年脓毒症患者并发重症监护病房获得性衰弱的风险因素分析及mNUTRIC评分的早期预测价值[J]. 实用医学杂志,2022,38 (20):2568-2573. doi: 10.3969/j.issn.1006-5725.2022.20.011 .
doi: 10.3969/j.issn.1006-5725.2022.20.011 |
| [7] |
CONNOLLY B A, JONES G D, CURTIS A A, et al. Clinical predictive value of manual muscle strength testing during critical illness: An observational cohort study[J]. Crit Care, 2013,17(5):R229. doi: 10.1186/cc13052 .
doi: 10.1186/cc13052 |
| [8] |
KASOTAKIS G, SCHMIDT U, PERRY D, et al. The surgical intensive care unit optimal mobility score predicts mortality and length of stay[J]. Crit Care Med, 2012,40(4):1122-1128. doi: 10.1097/CCM.0b013e3182376e6d .
doi: 10.1097/CCM.0b013e3182376e6d |
| [9] |
STEVENS R D, MARSHALL S A, CORNBLATH D R, et al. A framework for diagnosing and classifying intensive care unit-acquired weakness[J]. Crit Care Med, 2009,37(10 ):S299-S308. doi: 10.1097/CCM.0b013e3181b6ef67 .
doi: 10.1097/CCM.0b013e3181b6ef67 |
| [10] |
郑卉,史源,张钊龙,等. ICU获得性衰弱的研究进展[J]. 中华危重病急救医学,2024,36(3): 308-312. doi: 10.3760/cma.j.cn121430-20231113-00975 .
doi: 10.3760/cma.j.cn121430-20231113-00975 |
| [11] |
RIVERS E, NGUYEN B, HAVSTAD S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock[J]. N Engl J Med, 2001,345(19):1368-1377. doi: 10.1056/NEJMoa010307 .
doi: 10.1056/NEJMoa010307 |
| [12] |
DE JONGHE B, BASTUJI-GARIN S, DURAND M, et al. Respiratory weakness is associated with limb weakness and delayed weaning in critical illness[J]. Crit Care Med, 2007,35(9):2007-2015. doi: 10.1097/01.ccm.0000281450.01881.d8 .
doi: 10.1097/01.ccm.0000281450.01881.d8 |
| [13] |
PUTHUCHEARY Z A, RAWAL J, MCPHAIL M, et al. Acute skeletal muscle wasting in critical illness[J]. JAMA, 2013,310(15):1591-1600. doi: 10.1001/jama.2013.278481 .
doi: 10.1001/jama.2013.278481 |
| [14] |
KLAWITTER F, WALTER U, PATEJDL R, et al. Sonographic Evaluation of Muscle Echogenicity for the Detection of Intensive Care Unit-Acquired Weakness: A Pilot Single-Center Prospective Cohort Study[J]. Diagnostics (Basel), 2022,12(6):1378. doi: 10.3390/diagnostics12061378 .
doi: 10.3390/diagnostics12061378 |
| [15] |
WITTEVEEN E, SOMMERS J, WIESKE L, et al. Diagnostic accuracy of quantitative neuromuscular ultrasound for the diagnosis of intensive care unit-acquired weakness: A cross-sectional observational study[J]. Ann Intensive Care, 2017,7(1):40. doi: 10.1186/s13613-017-0263-8 .
doi: 10.1186/s13613-017-0263-8 |
| [16] |
周潇清, 鲁海燕, 鲁雅儿,等. 床旁超声评估四肢骨骼肌和膈肌对老年ICU获得性衰弱的诊断价值[J]. 实用医学杂志,2024(18):2629-2634. doi: 10.3969/j.issn.1006-5725.2024.18.021 .
doi: 10.3969/j.issn.1006-5725.2024.18.021 |
| [17] |
PUTHUCHEARY Z A, MCNELLY A S, RAWAL J, et al. Rectus Femoris Cross-Sectional Area and Muscle Layer Thickness: Comparative Markers of Muscle Wasting and Weakness[J]. Am J Respir Crit Care Med, 2017,195(1):136-138. doi: 10.1164/rccm.201604-0875LE .
doi: 10.1164/rccm.201604-0875LE |
| [18] |
MARRA M, SAMMARCO R, De LORENZO A, et al. Assessment of Body Composition in Health and Disease Using Bioelectrical Impedance Analysis (BIA) and Dual Energy X-Ray Absorptiometry (DXA): A Critical Overview[J]. Contrast Media Mol Imaging, 2019,2019:3548284. doi: 10.1155/2019/3548284 .
doi: 10.1155/2019/3548284 |
| [19] |
MOONEN H P F X, Van ZANTEN A R H. Bioelectric impedance analysis for body composition measurement and other potential clinical applications in critical illness[J]. Curr Opin Crit Care, 2021,27(4):344-353. doi: 10.1097/MCC.0000000000000840 .
doi: 10.1097/MCC.0000000000000840 |
| [20] |
MITOBE Y, MORISHITA S, OHASHI K, et al. Skeletal Muscle Index at Intensive Care Unit Admission Is a Predictor of Intensive Care Unit-Acquired Weakness in Patients With Sepsis[J]. J Clin Med Res, 2019,11(12):834-841. doi: 10.14740/jocmr4027 .
doi: 10.14740/jocmr4027 |
| [21] |
KUBIAK C A, RANGANATHAN K, MATUSKO N, et al. Computed Tomography Evidence of Psoas Muscle Atrophy Without Concomitant Tendon Wasting in Early Sepsis[J]. J Surg Res, 2019,234:210-216. doi: 10.1016/j.jss.2018.09.010 .
doi: 10.1016/j.jss.2018.09.010 |
| [22] |
DELLAGRAMMATICAS D, LEWIS S C, GOUGH M J, et al. Is heparin reversal with protamine after carotid endarterectomy dangerous?[J]. Eur J Vasc Endovasc Surg, 2008,36(1):41-44. doi: 10.1016/j.ejvs.2008.01.021 .
doi: 10.1016/j.ejvs.2008.01.021 |
| [23] |
HERMANS G, Van den BERGHE G. Clinical review: Intensive care unit acquired weakness[J]. Crit Care, 2015,19:274. doi: 10.1186/s13054-015-0993-7 .
doi: 10.1186/s13054-015-0993-7 |
| [24] |
de JONGHE B, LACHERADE J, SHARSHAR T, et al. Intensive care unit-acquired weakness: Risk factors and prevention[J]. Crit Care Med, 2009,37(10 ):S309-315. doi: 10.1097/CCM.0b013e3181b6e64c .
doi: 10.1097/CCM.0b013e3181b6e64c |
| [25] |
WITTEVEEN E, WIESKE L, SOMMERS J, et al. Early Prediction of Intensive Care Unit-Acquired Weakness: A Multicenter External Validation Study[J]. J Intensive Care Med, 2020,35(6):595-605. doi: 10.1177/0885066618771001 .
doi: 10.1177/0885066618771001 |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||