

实用医学杂志 ›› 2026, Vol. 42 ›› Issue (1): 1-11.doi: 10.3969/j.issn.1006-5725.2026.01.001
• 肿瘤诊治与预后专栏 •
邓波1,彭曹霞1,熊启连2,辇伟奇1,刘影1( )
)
收稿日期:2025-08-03
出版日期:2026-01-10
发布日期:2026-01-14
通讯作者:
刘影
E-mail:liuying_19_82@163.com
基金资助:
Bo DENG1,Caoxia PENG1,Qilian XIONG2,Weiqi NIAN1,Ying LIU1()
Received:2025-08-03
Online:2026-01-10
Published:2026-01-14
Contact:
Ying LIU
E-mail:liuying_19_82@163.com
摘要:
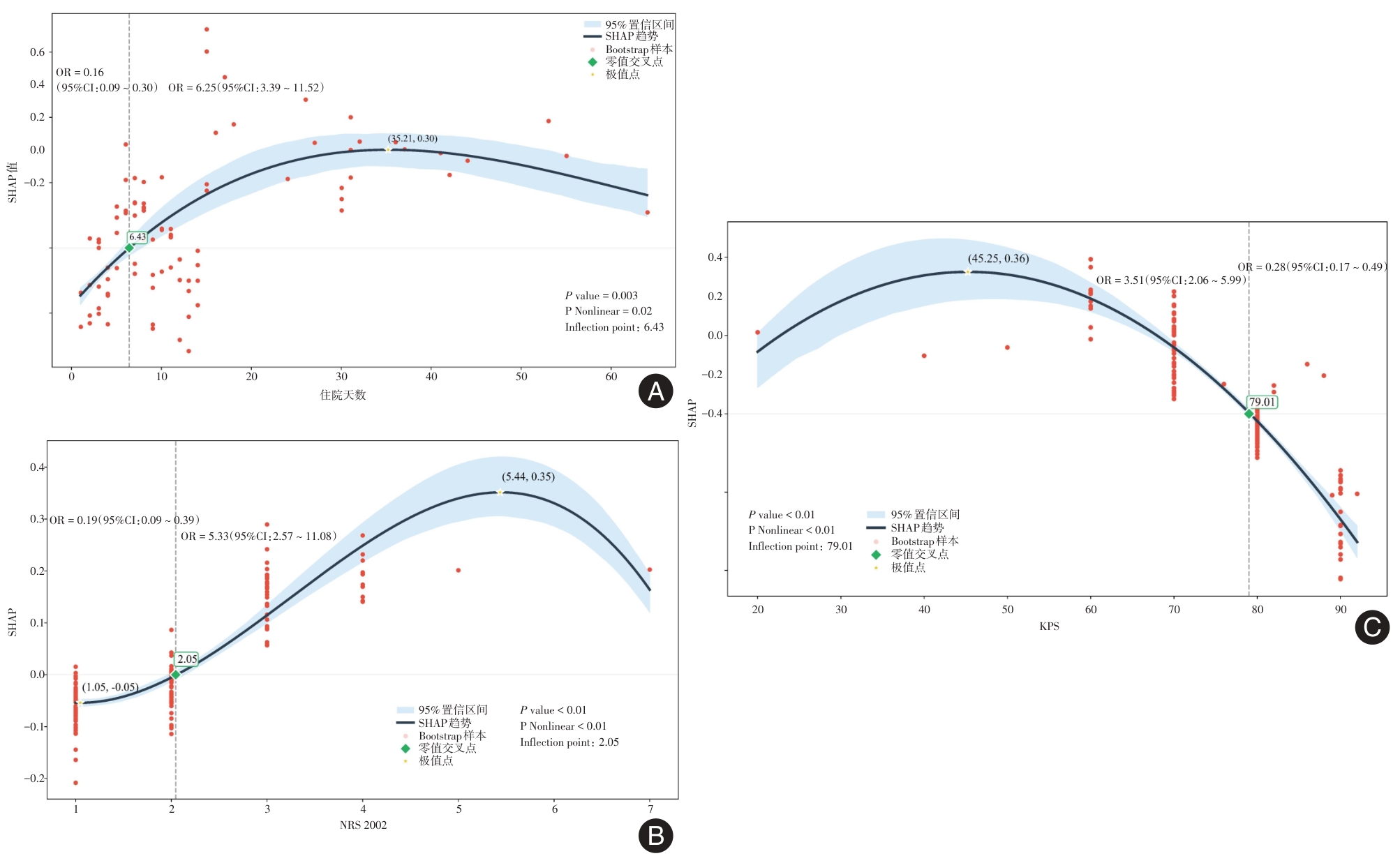
目的 探讨Ⅲ—Ⅳ期肺癌免疫检查点抑制剂(immune checkpoint inhibitors,ICIs)治疗后30 d内非计划再入院(unplanned patient readmission, UPR)的危险因素,构建并验证相应的风险预测模型。 方法 收集2023年1月至2024年5月在重庆市中医院接受ICIs治疗的Ⅲ—Ⅳ期肺癌患者的资料。应用Boruta算法初筛风险因素,采用logistic回归识别独立危险因素,构建列线图预测模型。通过受试者工作特征曲线(ROC)评估模型区分能力,以校准曲线验证模型一致性,利用决策曲线分析(DCA)评估其临床实用性。采用限制性立方样条回归(RCS)联合SHAP可解释分析明确危险因素与非计划再入院之间的剂量反应关系及阈值点。 结果 最终纳入284例患者,UPR发生率为30.63%。logistic回归分析显示住院天数、NRS 2002评分、介入治疗及KPS评分是非计划再入院的独立风险因素(P < 0.05)。模型训练集的ROC曲线AUC = 0.88,95%CI: 0.84 ~ 0.93,灵敏度84%,特异度80%,验证集的ROC曲线AUC = 0.87,95%CI: 0.79 ~ 0.95,灵敏度82%,特异度70%,模型的校准曲线接近于对角线,显示良好的准确性;DCA分析显示模型阈值在10% ~ 90%之间具有净获益,SHAP分析显示住院天数是UPR的关键因素,SHAP-RCS分析发现住院天数> 6.43 d、NRS 2002 > 2.05、KPS < 79.01且有介入手术史的患者再入院风险更高。 结论 基于4个风险因素构建的预测模型能有效预测Ⅲ—Ⅳ期肺癌ICIs患者30 d内非计划再入院的风险,具有良好的临床适用性,对于高风险患者应予以重点关注及提前干预。
中图分类号:
邓波,彭曹霞,熊启连,辇伟奇,刘影. Ⅲ—Ⅳ期肺癌免疫检查点抑制剂治疗30天内非计划再入院风险预测模型[J]. 实用医学杂志, 2026, 42(1): 1-11.
Bo DENG,Caoxia PENG,Qilian XIONG,Weiqi NIAN,Ying LIU. Predictive model for unplanned 30-day readmission in stage Ⅲ—Ⅳ lung cancer patients receiving immune checkpoint inhibitors[J]. The Journal of Practical Medicine, 2026, 42(1): 1-11.
表1
训练集与验证集患者基线对比 (例(%))"
| 变量 | 验证集(n = 84) | 训练集(n = 200) | t/Z/χ2值 | P值 |
|---|---|---|---|---|
| 年龄(x ± s)/岁 | 65.39 ± 9.78 | 64.75 ± 10.41 | 0.47 | 0.63 |
| 住院天数[M(P25,P75)]/d | 5.00(3.00, 9.00) | 5.00(3.00, 10.00) | 0.03 | 0.98 |
| 性别 | 0.37 | 0.54 | ||
| 女 | 27(32.1) | 57(28.5) | ||
| 男 | 57(67.9) | 143(71.5) | ||
| 吸烟 | 0.14 | 0.71 | ||
| 无 | 32(38.1) | 81(40.5) | ||
| 有 | 52(61.9) | 119(59.5) | ||
| 饮酒 | 3.21 | 0.07 | ||
| 无 | 42(50.0) | 123(61.5) | ||
| 有 | 42(50.0) | 77(38.5) | ||
| 介入治疗 | 0.005 | 0.95 | ||
| 无 | 70(83.3) | 166(83.0) | ||
| 有 | 14(16.7) | 34(17.0) | ||
| 远端转移 | 0.30 | 0.58 | ||
| 无 | 21(25.0) | 44(22.0) | ||
| 有 | 63(75.0) | 156(78.0) | ||
| TNM | 0.05 | 0.82 | ||
| Ⅲ期 | 22(26.2) | 55(27.5) | ||
| Ⅳ期 | 62(73.8) | 145(72.5) | ||
| KPS | 0.09 | 0.76 | ||
| < 70分 | 20(23.8) | 51(25.5) | ||
| ≥ 70分 | 64(76.2) | 149(74.5) | ||
| NRS 2002 | 0.80 | 0.37 | ||
| < 3分 | 65(77.4) | 164(82.0) | ||
| ≥ 3分 | 19(22.6) | 36(18.0) | ||
| TCMD | 1.79 | 0.18 | ||
| 虚证 | 71(84.5) | 155(77.5) | ||
| 实证 | 13(15.5) | 45(22.5) | ||
| RBC | 0.04 | 0.83 | ||
| 低 | 28(33.3) | 64(32.0) | ||
| 正常 | 56(66.7) | 136(68.0) | ||
| Hb | 0.09 | 0.76 | ||
| 低 | 28(33.3) | 63(31.5) | ||
| 正常 | 56(66.7) | 137(68.5) | ||
| WBC | 0.37 | 0.83 | ||
| < 3.5 × 109/L | 65(77.4) | 148(74.0) | ||
| 3.5 ~ 9.5 × 109/L | 12(14.3) | 32(16.0) | ||
| ≥ 9.5 × 109/L | 7(8.3) | 20(10.0) | ||
| NEUT | 2.88 | 0.24 | ||
| < 1.8 × 109/L | 60(71.4) | 149(74.5) | ||
| 1.8 ~ 6.3 × 109/L | 11(13.1) | 14(7.0) | ||
| ≥ 6.3 × 109/L | 13(15.5) | 37(18.5) | ||
| PLT | 0.48 | 0.79 | ||
| < 125 × 109/L | 54(64.3) | 136(68.0) | ||
| 125 ~ 350 × 109/L | 24(28.6) | 53(26.5) | ||
| ≥ 350 × 109/L | 6(7.1) | 11(5.5) | ||
| CRP | 2.57 | 0.11 | ||
| ≤ 10 mg/L | 44(52.4) | 84(42.0) | ||
| > 10 mg/L | 40(47.6) | 116(58.0) | ||
| ALB | 0.40 | 0.53 | ||
| < 40 g/L | 31(36.9) | 66(33.0) | ||
| 40 ~ 55 g/L | 53(63.1) | 134(67.0) | ||
| AFP | 2.11 | 0.15 | ||
| 0 ~ 7 mg/L | 71(84.5) | 181(90.5) | ||
| > 7 mg/L | 13(15.5) | 19(9.5) | ||
| CEA | 0.58 | 0.44 | ||
| 0 ~ 5 mg/L | 51(60.7) | 131(65.5) | ||
| > 5 mg/L | 33(39.3) | 69(34.5) | ||
| CA19-9 | 0.03 | 0.86 | ||
| 0 ~ 37 U/mL | 63(75.0) | 148(74.0) | ||
| > 37 U/mL | 21(25.0) | 52(26.0) | ||
| CA50 | 0.26 | 0.61 | ||
| 0 ~ 25 U/mL | 65(77.4) | 149(74.5) | ||
| > 25 U/mL | 19(22.6) | 51(25.5) |

图1
Boruta算法非计划再入院特征筛选结果注:绿色代表可接受因素,黄色代表待定因素,红色代表拒绝因素,蓝色分别表示平均、最小及最大的Z-score"
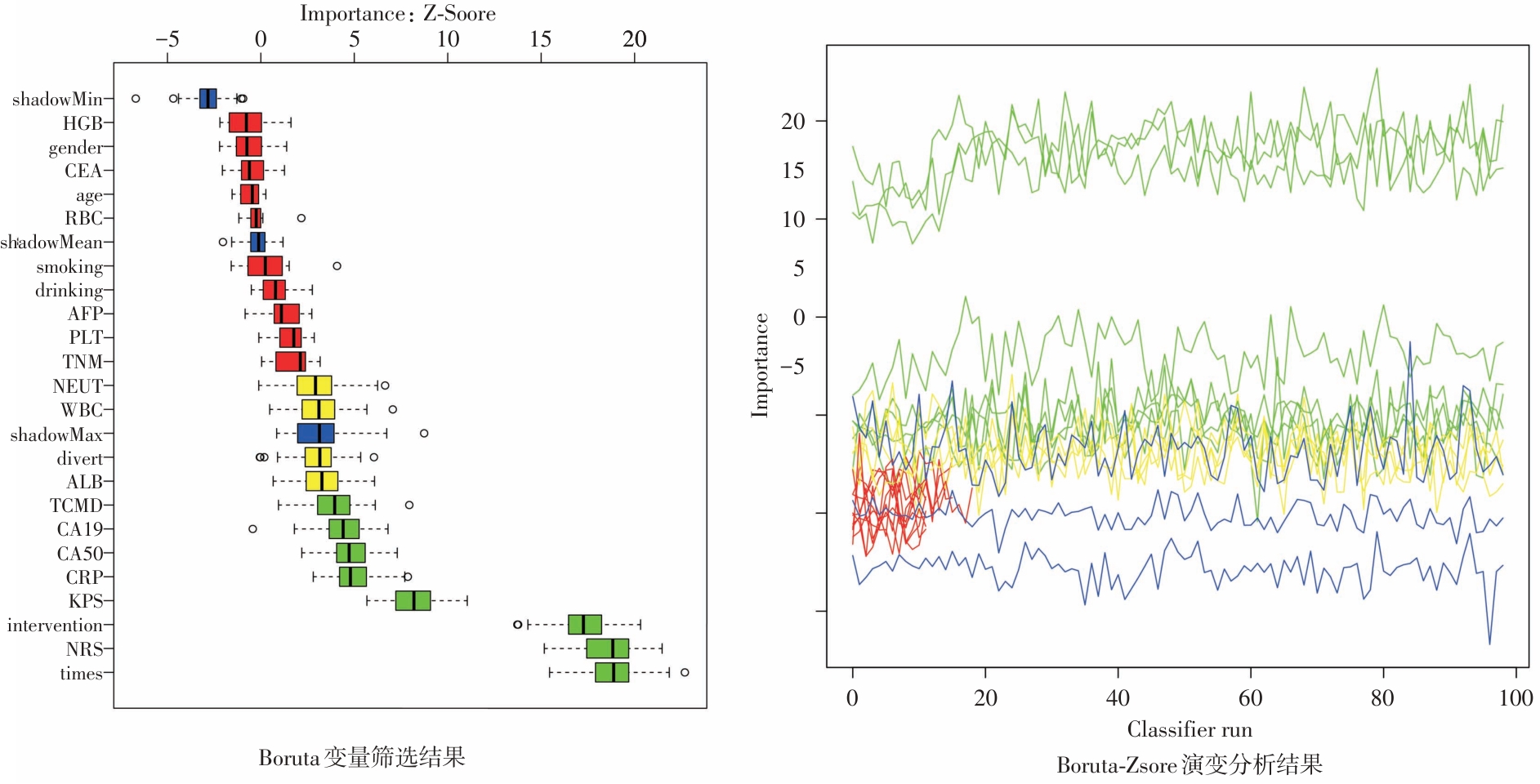
表2
Boruta筛选后单因素与多因素logistic回归分析结果"
| 变量 | 单因素分析 | 多因素分析 | |||
|---|---|---|---|---|---|
| OR(95%CI) | P值 | OR(95%CI) | P值 | ||
| 住院天数 | 1.115(1.06 ~ 1.169) | < 0.01 | 1.11(1.03 ~ 1.19) | < 0.01 | |
| 介入治疗 | |||||
| 否 | Ref | Ref | |||
| 是 | 5.26(2.41 ~ 11.47) | < 0.01 | 11.34(3.51 ~ 36.63) | < 0.01 | |
| CRP | |||||
| ≤ 10 mg/L | Ref | Ref | |||
| > 10 mg/L | 2.91(1.48 ~ 5.71) | < 0.01 | 1.46(0.60 ~ 3.56) | 0.4 | |
| CA19-9 | |||||
| 0 ~ 37 U/mL | Ref | Ref | |||
| > 37 U/mL | 2.379(1.23 ~ 4.61) | 0.01 | 0.65(0.17 ~ 2.49) | 0.53 | |
| CA50 | |||||
| 0 ~ 25 U/mL | Ref | Ref | |||
| > 25 U/mL | 2.79(1.43 ~ 5.43) | 0.003 | 1.61(0.43 ~ 5.96) | 0.47 | |
| KPS | |||||
| < 70分 | Ref | Ref | |||
| ≥ 70分 | 0.18(0.089 ~ 0.35) | < 0.01 | 0.22(0.08 ~ 0.58) | < 0.01 | |
| NRS 2002 | |||||
| < 3分 | Ref | Ref | |||
| ≥ 3分 | 11.90(5.11 ~ 27.74) | < 0.01 | 8.86(3.06 ~ 25.62) | < 0.01 | |
| TCMD | |||||
| 虚证 | Ref | Ref | |||
| 实证 | 0.81(0.39 ~ 1.71) | 0.58 | 0.92(0.43 ~ 1.81) | 0.62 | |

图2
非计划再入院logistic回归模型的综合评估注:A,受试者工作特征曲线及曲线下面积,specificity:特异度,sensitivity: 灵敏度;B,纳入模型各因素受试者工作特征曲线及曲线下面积;C、D,训练集与验证集校准曲线分析;E、F,训练集与验证集决策曲线分析"
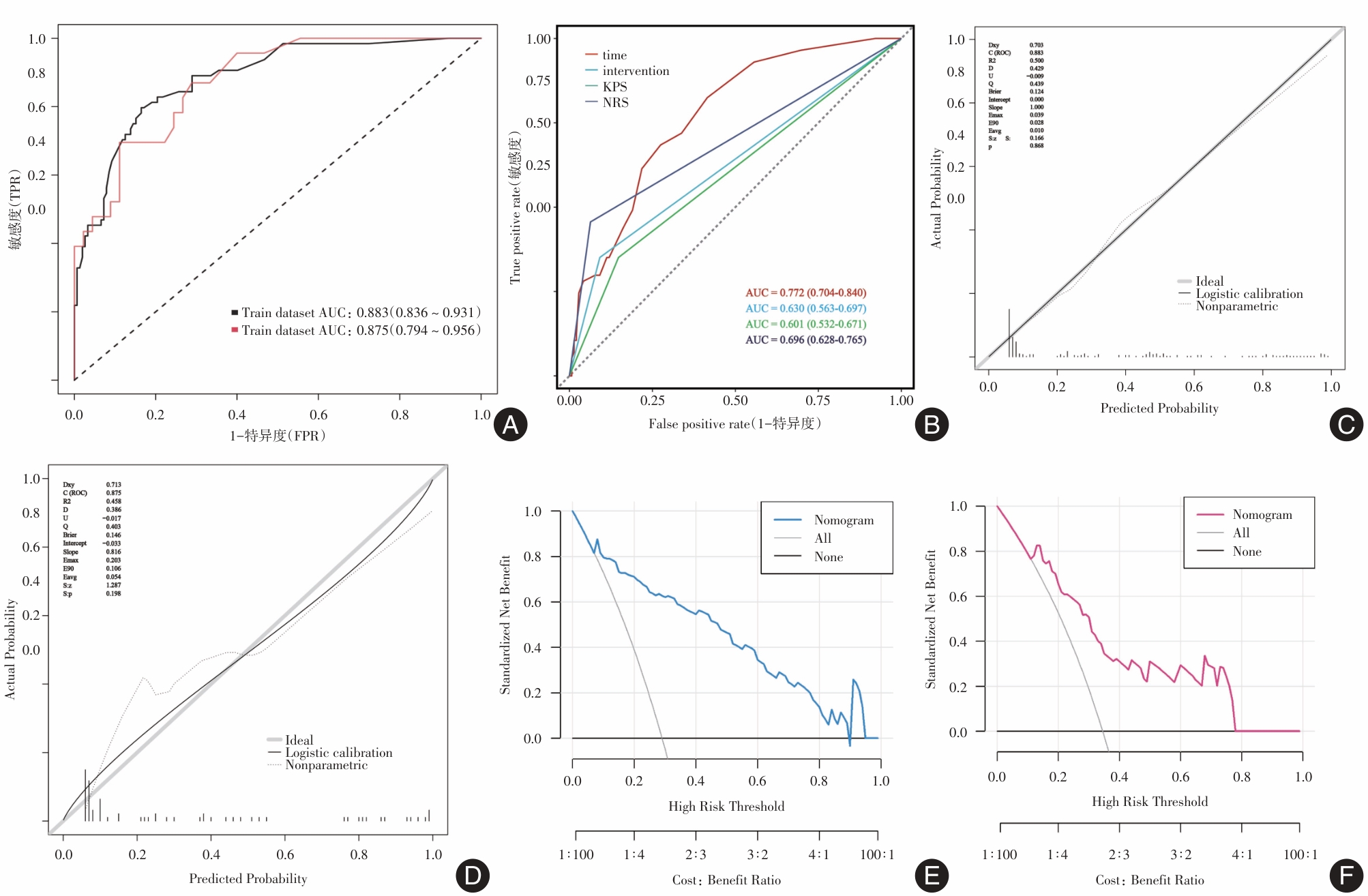

图3
Ⅲ—Ⅳ期肺癌ICIs治疗患者非计划再入院列线图注:A,基于logistic回归构建的列线图模型;B,第44号样本列线图得分及非计划发生风险概率"
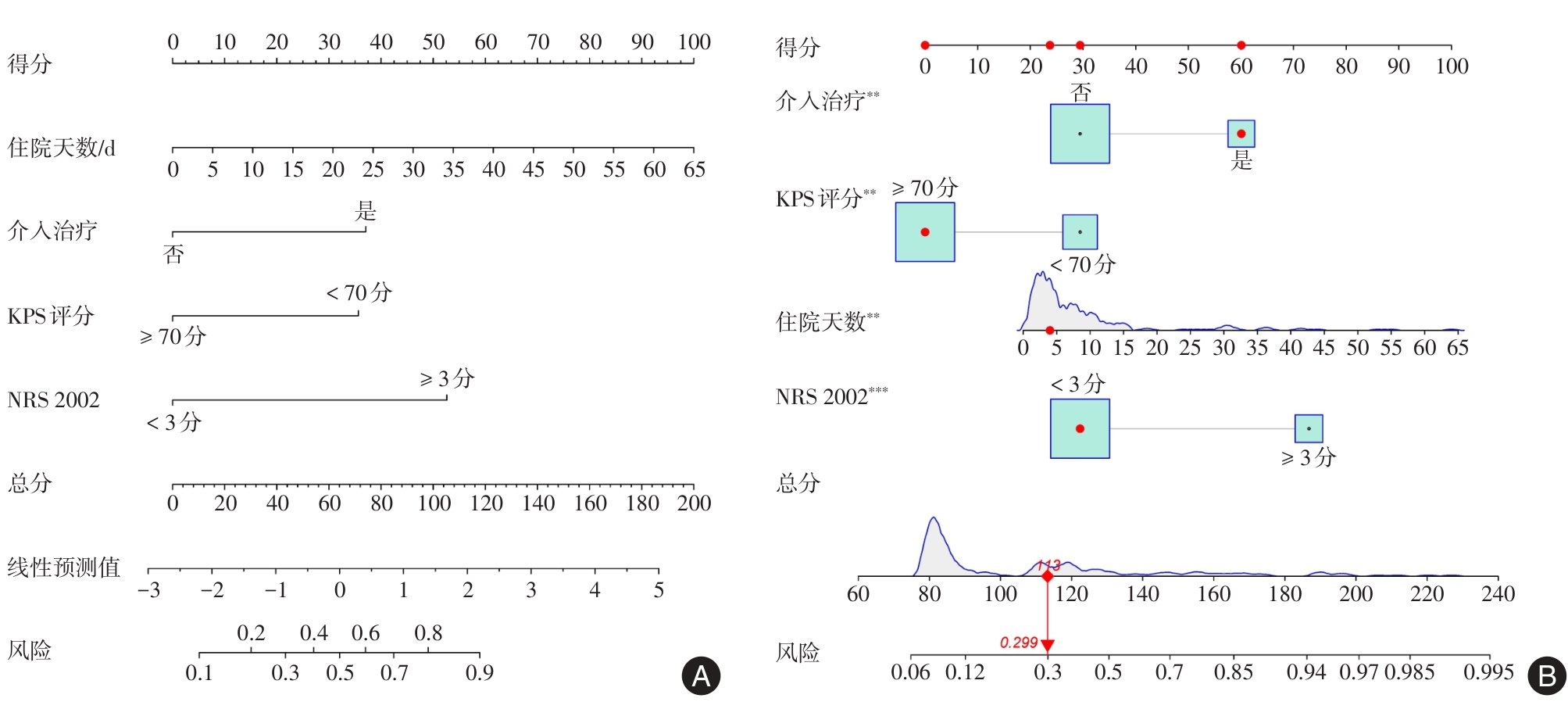

图4
logistic 回归列线图模型的SHAP 可解释性分析注:A,SHAP可解释图;B,SHAP全局条形图;C—D,第100、197号样本的SHAP力图。Times:住院天数,NRS 2002: 营养风险评分,Intervention:介入治疗,KPS:卡氏评分"
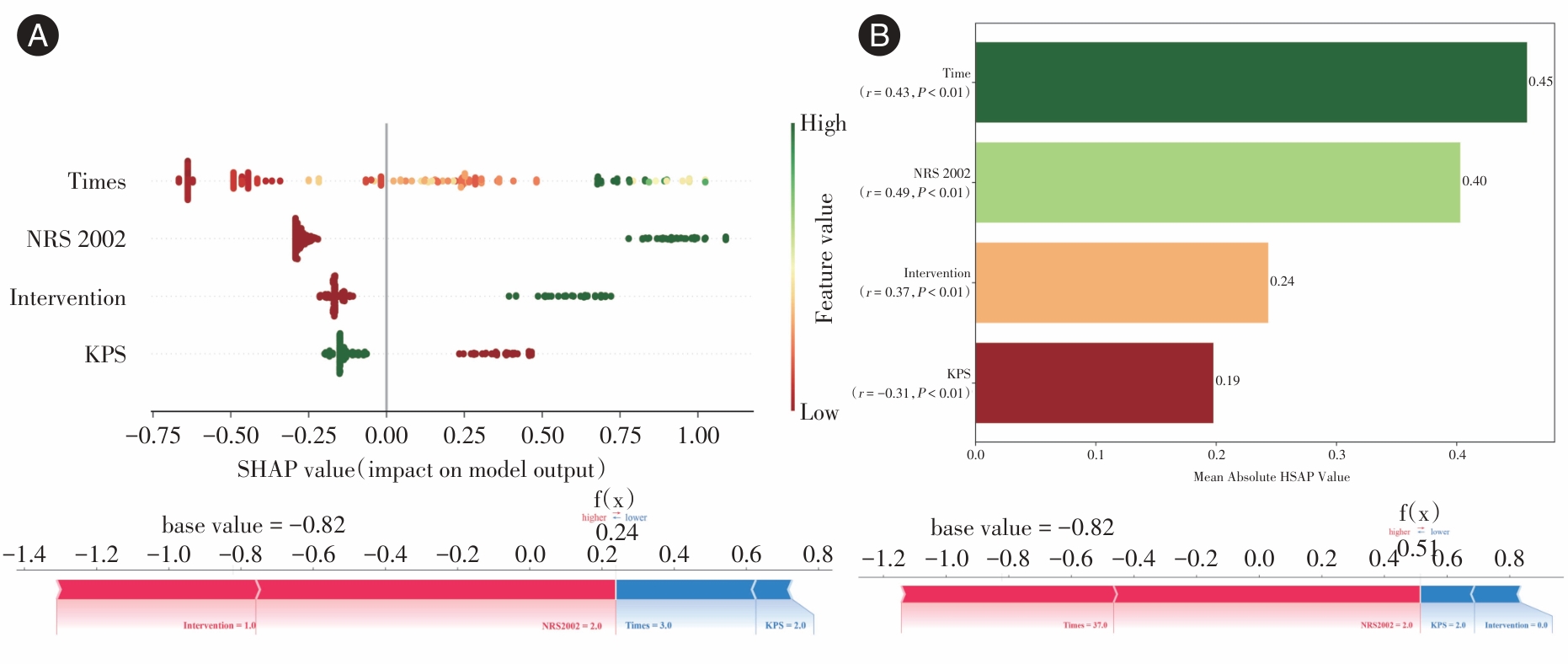
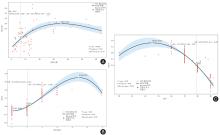
图5
KPS、NRS 2002、住院天数SHAP-RCS趋势分析注:A,住院天数特征SHAP趋势分析;B,NRS 2002特征SHAP趋势分析;C,KPS特征SHAP趋势分析;各模型中有2个节点,分别是零值交叉点与极值点。X轴表示特征值,Y轴为特征所对应的SHAP值,P值表示模型整体是否显著,P-Nonlinear表示是否存在非线性关系"
| [1] |
BRAY F, LAVERSANNE M, SUNG H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA-Cancer J Clin, 2024,74(3):229-263. doi: 10.3322/caac.21834 .
doi: 10.3322/caac.21834 |
| [2] |
SÁNCHEZ J C, NUÑEZ-GARCÍA B, RUANO-RAVINA A, et al. Patterns and outcome of unplanned care in lung cancer patients: An observational study in a medical oncology department[J]. Transl Lung Cancer Res, 2023, 12(8):1752-1765. doi: 10.21037/tlcr-23-48 .
doi: 10.21037/tlcr-23-48 |
| [3] |
MEDBERY R L, GILLESPIE T W, LIU Y, et al. Socioeconomic factors are associated with readmission after lobectomy for early stage lung cancer[J]. Ann Thorac Surg, 2016, 102(5): 1660-1667. doi: 10.1016/j.athoracsur.2016.05.060 .
doi: 10.1016/j.athoracsur.2016.05.060 |
| [4] |
PURI V, PATEL A P, CRABTREE T D, et al. Unexpected readmission after lung cancer surgery: A benign event? [J]. J Thorac Cardiovasc Surg, 2015, 150(6): 1496-504, 505.e1-5; discussion 504-505. doi: 10.1016/j.jtcvs.2015.08.067 .
doi: 10.1016/j.jtcvs.2015.08.067 |
| [5] |
CHUETZ P, SULO S, WALZER S, et al. Gomes F. Cost savings associated with nutritional support in medical inpatients: An economic model based on data from a systematic review of randomised trials[J]. BMJ Open, 2021, 11(7): e046402. doi: 10.1136/bmjopen-2020-046402 .
doi: 10.1136/bmjopen-2020-046402 |
| [6] |
NAIMI A, MOHAMMED R N, RAJI A, et al. Tumor immunotherapies by immune checkpoint inhibitors (ICIs); the pros and cons[J]. J Cell Commun Signal, 2022,20(1):44. doi: 10.1186/s12964-022-00854-y .
doi: 10.1186/s12964-022-00854-y |
| [7] |
WANG S J, DOUGAN S K, DOUGAN M. Immune mechanisms of toxicity from checkpoint inhibitors[J]. Trends in Cancer, 2023,9(7):543-553. doi: 10.1016/j.trecan.2023.04.002 .
doi: 10.1016/j.trecan.2023.04.002 |
| [8] |
CHHABRA N, KENNEDY J. A review of cancer immunotherapy toxicity: Immune checkpoint inhibitors[J]. J Med Toxicol, 2021, 17(4):411-424. doi: 10.1007/s13181-021-00833-8 .
doi: 10.1007/s13181-021-00833-8 |
| [9] |
THOMPSON J A, SCHNEIDER B J, BRAHMER J, et al. Management of immunotherapy-related toxicities, version 1.2022, nccn clinical practice guidelines in oncology[J]. J Natl Compr Canc Netw, 2022, 20(4):387-405. doi: 10.6004/jnccn. 2022. 0020 .
doi: 10.6004/jnccn. 2022. 0020 |
| [10] |
COUSSENS L M, WERB Z. Inflammation and cancer[J]. Nature, 2002, 420(6917): 860-867. doi: 10.1038/nature01322 .
doi: 10.1038/nature01322 |
| [11] |
GRETEN F R, GRIVENNIKOV S I. Inflammation and cancer: Triggers, mechanisms, and consequences[J]. Immunity, 2019, 51(1): 27-41. doi: 10.1016/j.immuni.2019.06.025 .
doi: 10.1016/j.immuni.2019.06.025 |
| [12] |
MANTOVANI A. The inflammation-cancer connection[J]. FEBS J, 2018, 285(4): 638-640. doi: 10.1111/febs.14395 .
doi: 10.1111/febs.14395 |
| [13] |
ECCLESTON D, DUONG M N, CHOWDHURY E, et al. Early vs. Late readmission following percutaneous coronary intervention: Predictors and impact on long-term outcomes[J]. J Clin Med, 2023, 12(4):1684. doi: 10.3390/jcm12041684 .
doi: 10.3390/jcm12041684 |
| [14] |
HUANG D, HARRISON R, CURTIS E, et al. Beyond post-operative readmissions: Analysis of the impact of unplanned readmissions during primary treatment of advanced-stage epithelial ovarian cancer on long-term oncology outcome[J]. Int J Gynecol Cancer, 2023, 33(5):741-748. doi: 10.1136/ijgc-2022-003765 .
doi: 10.1136/ijgc-2022-003765 |
| [15] |
KASPER J, WACH J, VYCHOPEN M, et al. Unplanned 30-day readmission in glioblastoma patients: Implications for the extent of resection and adjuvant therapy[J]. Cancers (Basel), 2023, 15(15):390. doi: 10.3390/cancers15153907 .
doi: 10.3390/cancers15153907 |
| [16] |
VAN SMEDEN M, MOONS K G, DE GROOT J A, et al. Sample size for binary logistic prediction models: Beyond events per variable criteria[J]. Stat Methods Med Res, 2019, 28(8): 2455-2474. doi: 10.1177/0962280218784726 .
doi: 10.1177/0962280218784726 |
| [17] |
VITTINGHOFF E, MCCULLOCH C E. Relaxing the rule of ten events per variable in logistic and Cox regression[J]. Am J Epidemiol, 2007, 165(6): 710-718. doi: 10.1093/aje/kwk052 .
doi: 10.1093/aje/kwk052 |
| [18] |
SOHIL F, SOHALI M U, SHABBIR J. An introduction to statistical learning with applications in R, eISBN: 978-1-4614-7137-7[J]. Statist Theor Relat Field, 2022, 6(1): 87. doi: 10.1080/24754269.2021.1980261 .
doi: 10.1080/24754269.2021.1980261 |
| [19] |
KURSA M B, RUDNICKI W R. Feature selection with the boruta package[J]. J Statist Soft, 2010, 36(11): 1-13. doi: 10.18637/jss.v036.i11 .
doi: 10.18637/jss.v036.i11 |
| [20] |
LUNDBERG S, LEE S I. A Unified Approach to Interpreting Model Predictions[J]. arXiv, 2017. doi:10.48550/arXiv. 1705. 07874 .
doi: 10.48550/arXiv. 1705. 07874 |
| [21] |
ZHU R, ZHANG Y, ZHANG J, et al. Development and validation of an explainable machine learning model for predicting occult lymph node metastasis in early-stage oral tongue squamous cell carcinoma a multi-center study[J]. Int J Surg, 2025,111(8):5022-5035. doi: 10.1097/JS9.0000000000002641 .
doi: 10.1097/JS9.0000000000002641 |
| [22] |
DONG W, JIANG H, LI Y, et al. Interpretable machine learning analysis of immunoinflammatory biomarkers for predicting CHD among NAFLD patients[J]. Cardiovasc Diabetol, 2025, 24(1):263. doi: 10.1186/s12933-025-02818-1 .
doi: 10.1186/s12933-025-02818-1 |
| [23] |
李文锋, 李建华, 王正昕. 肝癌肝移植术前应用免疫检查点抑制剂治疗的进展[J]. 器官移植, 2025, 16(3): 329-337. doi: 10.12464/j.issn.1674-7445.2025094 .
doi: 10.12464/j.issn.1674-7445.2025094 |
| [24] |
陈静文, 徐林霞, 吴秀丽, 等. 基于Logistic回归与决策树模型的结直肠癌术后患者非计划性再入院影响因素分析[J]. 护理学报, 2022,29(2):1-6. doi: 10.16460/j.issn1008-9969. 2022. 02.001 .
doi: 10.16460/j.issn1008-9969. 2022. 02.001 |
| [25] |
李静, 侯云霞, 强万敏. 癌症患者非计划性再入院风险预测模型的范围综述[J]. 中华护理杂志, 2022,57(9):1079-1087. doi: 10.3761/j.issn.0254-1769.2022.09.008 .
doi: 10.3761/j.issn.0254-1769.2022.09.008 |
| [26] |
SHAH M P, NEAL J W. Relative impact of anticancer therapy on unplanned hospital care in patients with non–small-cell lung cancer[J]. JCO Oncol Pract, 2021, 17(8): e1131-e1138. doi: 10.1200/OP.20.00612 .
doi: 10.1200/OP.20.00612 |
| [27] |
HARRON K, GILBERT R, CROMWELL D, et al. Newborn length of stay and risk of readmission[J]. Paediatr Perinat Epidemiol, 2017, 31(3):221-232. doi: 10.1111/ppe.12359 .
doi: 10.1111/ppe.12359 |
| [28] |
LENNES I T, EUSEBIO J, BOHLEN N, et al. Characterization of unplanned 30-day medical oncology readmissions after discharge at an academic medical center with a comprehensive cancer center[J]. J Clin Oncol, 2016, 34(7) suppl: 269. doi: 10.1200/jco.2016.34.7_suppl.269 .
doi: 10.1200/jco.2016.34.7_suppl.269 |
| [29] |
BISWAS S, DINH D, LUCAS M, et al. Incidence and predictors of unplanned hospital readmission after percutaneous coronary intervention[J]. J Clin Med, 2020, 9(10):3242. doi: 10.3390/jcm9103242 .
doi: 10.3390/jcm9103242 |
| [30] |
刘剑, 李敏菁. 全身免疫炎症指数对非小细胞肺癌免疫检查点抑制剂疗效的预测价值[J].实用医学杂志, 2022,38(7):904-908. doi: 10.3969/j.issn.1006-5725.2022.07.024 .
doi: 10.3969/j.issn.1006-5725.2022.07.024 |
| [31] |
TANG Q, CHEN Y, LI X, et al. The role of PD-1/PD-L1 and application of immune-checkpoint inhibitors in human cancers[J]. Front Immunol, 2022,13(1):964442. doi: 10.3389/fimmu. 2022.964442 .
doi: 10.3389/fimmu. 2022.964442 |
| [32] |
CATA J P, CORRALES G, SPEER B, et al. Postoperative acute pain challenges in patients with cancer[J]. Best Pract Res Clin Anaesthesiol, 2019,33(3):361-371. doi: 10.1016/j.bpa. 2019. 07.018 .
doi: 10.1016/j.bpa. 2019. 07.018 |
| [33] | WU D T Y, VITHALA T M, VU H, et al. Development of a clinical decision support system to predict unplanned cancer readmissions[J]. AMIA Annu Symp Proc, 2022,2022:1173-1180. |
| [34] |
THIAGARAJAN S, KANTAMANI T, SATHE P, et al. Impact of surgical site infection on unplanned hospital readmissions, initiation of adjuvant treatment following surgery, and disease-free survival on patients with upper aerodigestive tract squamous cell carcinoma[J]. J Surg Oncol, 2023,128(4):692-700. doi: 10.1002/jso.27356 .
doi: 10.1002/jso.27356 |
| [35] |
GUVEN D C, CEYLAN F, CAKIR I Y, et al. Evaluation of early unplanned readmissions and predisposing factors in an oncology clinic[J]. Support Care Cancer, 2021,29(7):4159-4164. doi: 10.1007/s00520-020-05927-7 .
doi: 10.1007/s00520-020-05927-7 |
| [36] |
YUAN Q, YAO H J, XI C H, et al. Perioperative risk factors associated with unplanned neurological intensive care unit readmission following elective supratentorial brain tumor resection[J]. J Neurosurg, 2022, 139(2):315-323. doi: 10.3171/2022.10.JNS221318 .
doi: 10.3171/2022.10.JNS221318 |
| [37] |
ZHOU J, YE D, ZHANG S, et al. The impact of karnofsky performance status on prognosis of patients with hepatocellular carcinoma in liver transplantation[J]. BMC Gastroenterol, 2024,24(1):85. doi: 10.1186/s12876-024-03161-7 .
doi: 10.1186/s12876-024-03161-7 |
| [38] |
郭科迪, 武岩, 汤夕慧, 等.术前衰弱对老年肺癌患者术后并发症的影响[J]. 实用医学杂志, 2023,39(15):1956-1960. doi: 10.3969/j.issn.1006-5725.2023.15.017 .
doi: 10.3969/j.issn.1006-5725.2023.15.017 |
| [39] |
MANZANO J M, LIN H, ZHAO H, et al. Derivation and validation of the cancer readmit score: a readmission risk scoring system for patients with solid tumor malignancies[J]. JCO Oncol Pract, 2022,18(1): e117-e128. doi: 10.1200/OP.20.01077 .
doi: 10.1200/OP.20.01077 |
| [40] |
PRADO C M, PURCELL S A, LAVIANO A. Nutrition interventions to treat low muscle mass in cancer[J]. J Cachexia Sarcopenia Muscle, 2020,11(2):366-380. doi: 10.1002/jcsm.12525 .
doi: 10.1002/jcsm.12525 |
| [41] |
匡荣康, 顾熙. 南京某三级医院2015至2019年间胃肠道恶性肿瘤病人营养风险和营养治疗现状调查分析[J]. 肠外与肠内营养, 2020,27(6):350-354. doi: 10.16151/j.1007-810x.2020.06.007 .
doi: 10.16151/j.1007-810x.2020.06.007 |
| [42] |
CHANG L, CHENG Q, MA Y, et al. Prognostic effect of the controlling nutritional status score in patients with esophageal cancer treated with immune checkpoint inhibitor[J]. J Immunother, 2022, 45(9):415-422. doi: 10.1097/CJI.0000000000000438 .
doi: 10.1097/CJI.0000000000000438 |
| [43] |
HERSBERGER L, BARGETZI L, TRIBOLET P, et al. Nutritional risk screening (NRS 2002) is a strong and modifiable predictor risk score for short-term and long-term clinical outcomes: Secondary analysis of a prospective randomised trial[J]. Clin Nutr, 2020,39(9):2720-2729. doi: 10.1016/j.clnu.2019.11.041 .
doi: 10.1016/j.clnu.2019.11.041 |
| [44] |
WANG F, DONG Q, YU K, et al. Nutrition risk screening and related factors analysis of non-hospitalized cancer survivors: A nationwide online survey in China[J]. Front Nutr, 2022,9:920714. doi: 10.3389/fnut.2022.920714 .
doi: 10.3389/fnut.2022.920714 |
| [45] |
王娜, 秦卓, 刘慧珍, 等. 营养风险评分对脓毒症相关性急性肾损伤患者预后的临床价值[J]. 中华危重病急救医学, 2022,34(3):245-249. doi: 10.3760/cma.j.cn121430-20211019-01525 .
doi: 10.3760/cma.j.cn121430-20211019-01525 |
| [46] |
GREENLEE H, SANTIAGO-TORRES M, MCMILLEN K K, et al. Helping patients eat better during and beyond cancer treatment: Continued nutrition management throughout care to address diet, malnutrition, and obesity in cancer[J]. Cancer J, 2019,25(5):320-328. doi: 10.1097/PPO.0000000000000405 .
doi: 10.1097/PPO.0000000000000405 |
| [47] |
PRADO C M, LANDI F, CHEW S T H, et al. Advances in muscle health and nutrition: A toolkit for healthcare professionals[J]. Clin Nutr, 2022, 41(10):2244-2263. doi: 10.1016/j.clnu. 2022.07.041 .
doi: 10.1016/j.clnu. 2022.07.041 |
| [48] |
LI Y F, NIE R C, WU T, et al. Prognostic value of the nutritional risk screening 2002 scale in metastatic gastric cancer: A large-scale cohort study[J]. J Cancer, 2019,10(1):112-119. doi: 10.7150/jca.27729 .
doi: 10.7150/jca.27729 |
| [1] | 赵应鼎,李邦胜,薛天天,资棋涵,杨欣,王曦. 微波消融术与亚肺叶切除术对ⅠA期非小细胞肺癌疗效的倾向评分匹配对比分析[J]. 实用医学杂志, 2025, 41(7): 976-984. |
| [2] | 董魁,吴洁,燕静,刘海涛,王军,乔冠恩. 大肠腺瘤性息肉危险因素及预测模型的构建与验证[J]. 实用医学杂志, 2025, 41(6): 838-845. |
| [3] | 何丽妃,朱琳,薛峰,闭祖悦,李赵鑫. LINC01772对A549细胞周期、凋亡及放疗敏感性的影响[J]. 实用医学杂志, 2025, 41(5): 657-663. |
| [4] | 刘冬丽,全梓林,钟灵秀,陈琦琦,蔡文巧,庄森培,魏莹,潘惠仪,林雅文. 儿童先天性心脏病术后抗生素相关性腹泻预测模型的构建与验证[J]. 实用医学杂志, 2025, 41(5): 683-690. |
| [5] | 黄洋,屈舸,王培宗,曾维安,闫芳. 术中使用地塞米松对非小细胞肺癌患者术后长期生存的影响[J]. 实用医学杂志, 2025, 41(5): 724-730. |
| [6] | 张宏威,王楠,石国西,翟俊英,钮红丽,王颖. 血清FGF-21、AMH及NRP-1联合预测体外受精-胚胎移植术后孕6周胎停育的模型构建与验证[J]. 实用医学杂志, 2025, 41(22): 3480-3489. |
| [7] | 杨秀冬,刘星,刘鑫,姜岩,王维,何宗斌,黄沙,文美红,刘亚珍. 腹腔镜下根治性前列腺切除术后淋巴漏风险预测模型的构建与验证[J]. 实用医学杂志, 2025, 41(21): 3378-3384. |
| [8] | 王照,左解鹏,车航,任凌云,徐哲,王磊. 血浆PPARγ作为女性间质性膀胱炎/膀胱疼痛综合征潜在诊断标志物的评估及其预测价值[J]. 实用医学杂志, 2025, 41(2): 258-263. |
| [9] | 高晓坤,谢子明,陶广昱,孙炎冰,任华,于佳卉,朱琳,于红,倪其鸣. 能谱和灌注CT多参数定量分析鉴别肺癌病理分型的应用[J]. 实用医学杂志, 2025, 41(19): 3096-3105. |
| [10] | 王翠翠,乔万通,姚俊英,李倩,高维鸽,范旻. 营养控制状态评分联合预后营养指数评估老年结直肠癌患者合并贫血风险的临床应用价值[J]. 实用医学杂志, 2025, 41(17): 2696-2704. |
| [11] | 曹玲春,孟凡亮,盛晓安. 非小细胞肺癌免疫治疗相关甲状腺功能障碍的危险因素分析及模型构建[J]. 实用医学杂志, 2025, 41(17): 2705-2714. |
| [12] | 王兆阳,张楠. 基于CT影像组学与中医舌象特征构建肝细胞癌根治术后早期复发的Nomogram预测模型[J]. 实用医学杂志, 2025, 41(16): 2590-2596. |
| [13] | 张红,章容,杨鹏程,罗丽艳,张文龙,成玉蓉,刘文琳,董文斌. 大理高海拔地区早产儿呼吸窘迫综合征发生风险的列线图预测模型构建[J]. 实用医学杂志, 2025, 41(15): 2342-2348. |
| [14] | 丘海,归奕飞,刘媛. 术前腋窝超声正常的临床T1—2 N0乳腺癌患者发生前哨淋巴结转移的预测模型[J]. 实用医学杂志, 2025, 41(14): 2143-2151. |
| [15] | 乔玉海,杜春花,赵新鸿,孟晓东,张剑飞. 慢性非细菌性前列腺炎患者临床特征及风险预测模型的构建和验证[J]. 实用医学杂志, 2025, 41(14): 2224-2230. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||