实用医学杂志 ›› 2025, Vol. 41 ›› Issue (24): 3883-3890.doi: 10.3969/j.issn.1006-5725.2025.24.012
• 临床研究 • 上一篇
张路1,何芬1,梁晓一1,刘小霞1,蓝茂英1,许文伟1,莫威1,孙建聪1,邹俊涛2( )
)
Lu ZHANG1,Fen HE1,Xiaoyi LIANG1,Xiaoxia LIU1,Maoying LAN1,Wenwei XU1,Wei MO1,Jiancong SUN1,Juntao. ZOU2()
摘要:
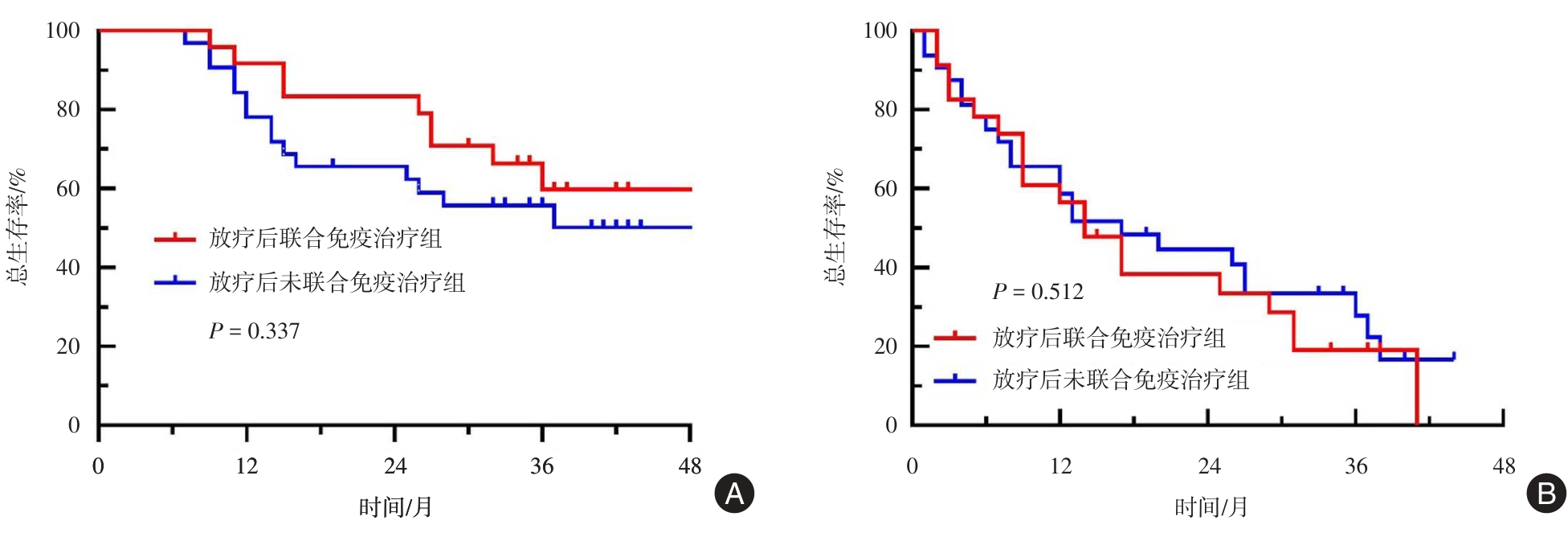
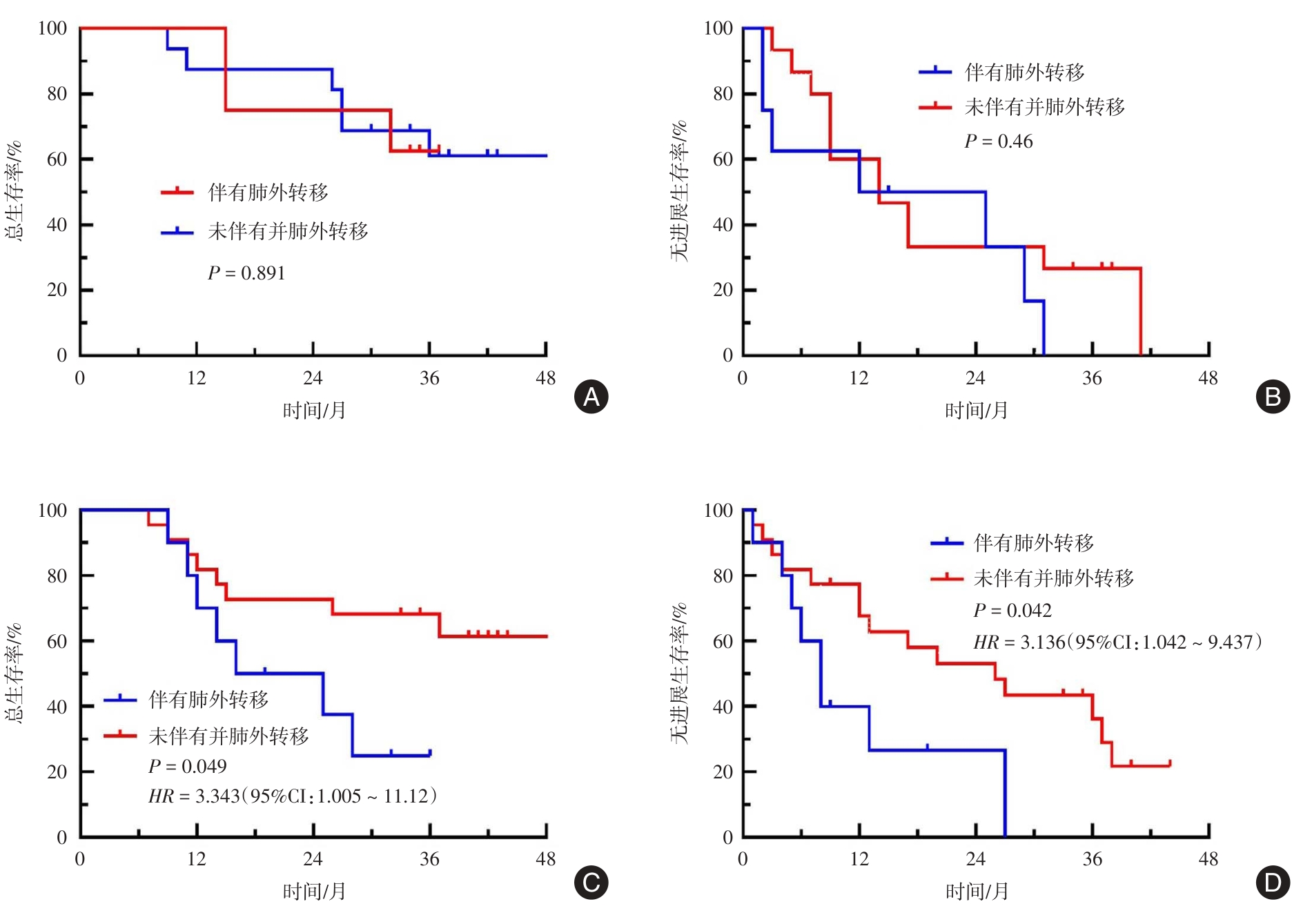
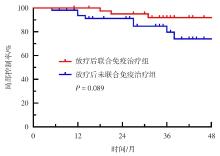
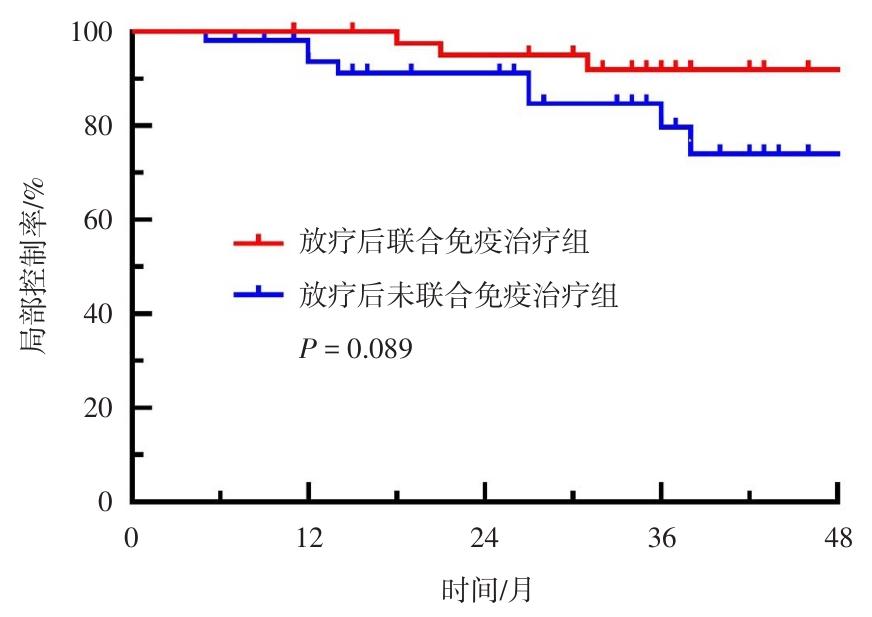
目的 评估大分割放疗或立体定向放射治疗(stereotactic body radiotherapy,SBRT)后联合免疫治疗对肺转移瘤患者生存的影响,并分析该联合治疗方案的疗效和安全性。 方法 回顾性纳入2021年1月至2023年1月在广州医科大学附属第一医院接受大分割放疗或SBRT治疗的56例不同病理类型肺转移瘤患者(共104个病灶)的临床资料。根据治疗策略,将患者分为大分割放疗或SBRT后联合免疫治疗组(n = 24)和大分割放疗或SBRT后未联合免疫治疗组(n = 32)。主要研究目的为总生存时间(overall survival,OS),次要研究目的包括无进展生存时间(progression-free survival,PFS),局部控制率(local control rate,LCR)和安全性。通过Kaplan-Meier和Cox回归模型进行生存分析,并探索伴有肺外转移在不同治疗策略下的预后价值。 结果 纳入患者原发肿瘤以肺癌(35/56,62.5%),消化系统(8/56,14.3%)和头颈肿瘤(6/56,10.7%)为主。至数据分析截止日(2025年7月31日),放疗后联合免疫治疗组的2年和3年OS高于未联合免疫治疗组,呈现生存获益趋势,但差异无统计学意义(2年OS:83.3% vs. 65.6%;3年OS:59.8% vs. 55.8%,P = 0.337)。探索性分析发现,在未联合免疫治疗组中,伴有肺外转移患者较仅肺转移瘤患者的生存期明显缩短,中位OS为16个月vs.未达到(HR = 3.343,95% CI:1.005~11.120,P = 0.049),中位PFS为8个月vs. 26个月(HR = 3.136,95% CI:1.042~9.437,P = 0.042)。而在联合免疫治疗组中,是否伴有肺外转移对OS(HR = 1.099,95% CI:0.268~4.496,P = 0.891)与PFS(HR = 1.525,95% CI:0.558~4.167,P = 0.46)均无显著影响。联合治疗组2年和3年LCR在数值上高于未联合免疫治疗组(2年:95% vs. 91.2%;3年:91.9% vs. 79.7%,P = 0.089)。治疗安全性良好,≥ 2级急性放射性肺炎(acute radiation pneumonitis, ARP)发生率为15.4%,无4级及以上ARP事件。 结论 大分割放疗或SBRT后联合免疫治疗显示出改善肺转移瘤患者生存的趋势,虽未达到统计学显著性,但是对伴有肺外转移的患者,采用该治疗模式能够获得与仅肺转移患者相当的生存预后。这一发现具有一定的临床启发意义,为晚期肺转移瘤的治疗策略优化提供了新思路。
中图分类号: