

The Journal of Practical Medicine ›› 2024, Vol. 40 ›› Issue (12): 1651-1658.doi: 10.3969/j.issn.1006-5725.2024.12.007
• Clinical Research • Previous Articles Next Articles
Yancun ZHENG1,2,Zhu DONG2,3,Jinli LIN2,3,Xiaowu WANG2,3
Received:2023-10-09
Online:2024-06-25
Published:2024-06-14
CLC Number:
Yancun ZHENG,Zhu DONG,Jinli LIN,Xiaowu WANG. The role of 3D printing technology in the preoperative interventional endovascular exclusion of Stanford B aortic dissection[J]. The Journal of Practical Medicine, 2024, 40(12): 1651-1658.
Tab.1
Comparison of basic information between two groups of patients"
| 组别 | 例数 | 年龄(x ± s,岁) | 性别 | 高血压 | 糖尿病 | 高血脂 | 冠心病 | |
|---|---|---|---|---|---|---|---|---|
| 男 | 女 | |||||||
| 模拟组 | 40 | 62.9 ± 7.1 | 30(75.00) | 10(25.00) | 21(52.50) | 12(30.00) | 29(72.50) | 9(22.50) |
| 对照组 | 36 | 64.5 ± 8.2 | 30(83.33) | 6(16.67) | 25(69.44) | 16(44.44) | 22(61.11) | 4(11.11) |
| t/χ 2 值 | -0.912 | 0.792 | 2.277 | 1.97 | 0.798 | 1.597 | ||
| P值 | 0.365 | 0.314 | 0.131 | 0.16 | 0.372 | 0.206 | ||
| 组别 | 例数 | BMI(x ± s,kg/m2) | NYHA分级 | 胸痛 | 胸闷 | 吸烟 | 饮酒 | |
| ≤Ⅱ级 | > 级 | |||||||
| 模拟组 | 40 | 23.38 ± 1.80 | 29(72.50) | 11(27.50) | 38(95.00) | 35(87.50) | 21(52.50) | 17(42.05) |
| 对照组 | 36 | 23.72 ± 1.92 | 31(86.11) | 5(13.89) | 35(97.22) | 30(83.33) | 17(47.22) | 12(33.33) |
| t/χ 2 值 | -0.797 | 2.112 | 0.247 | 0.052 | 0.115 | 0.675 | ||
| P值 | 0.428 | 0.146 | 0.619 | 0.82 | 0.734 | 0.411 | ||

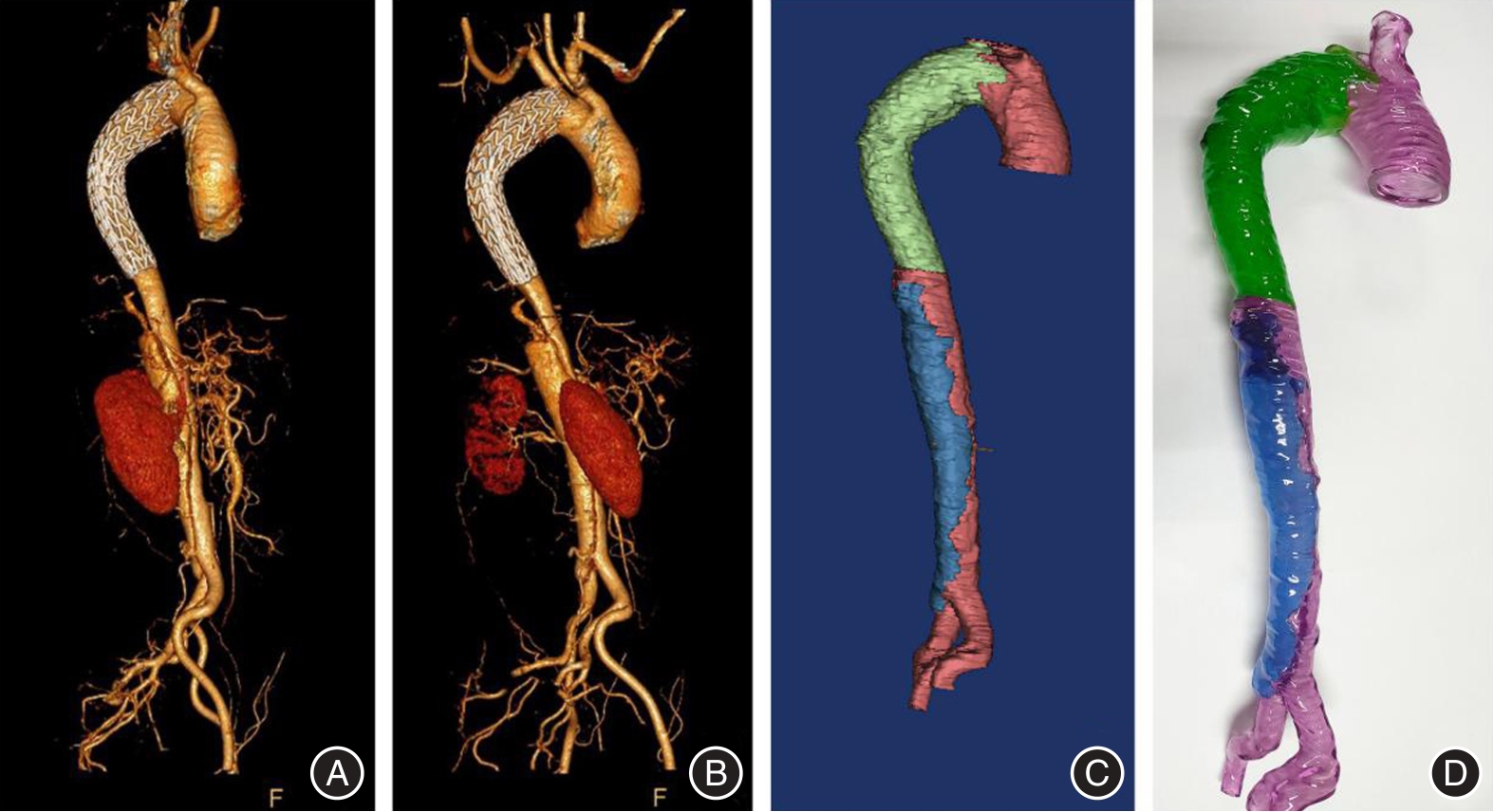
Fig.1
Preoperative CTA with 3D model"
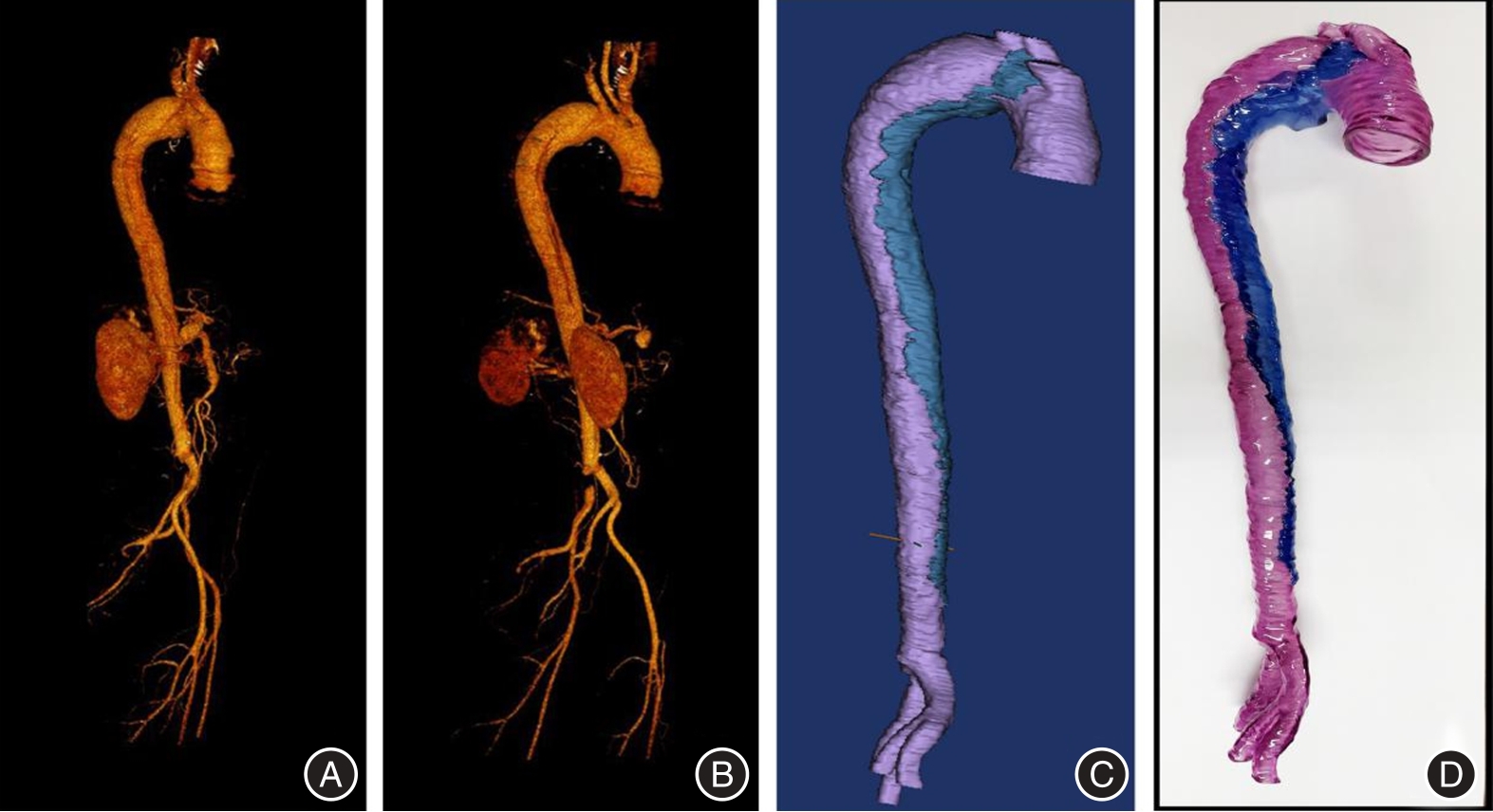
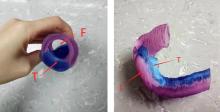
Fig.2
3D printed model of aortic dissection"
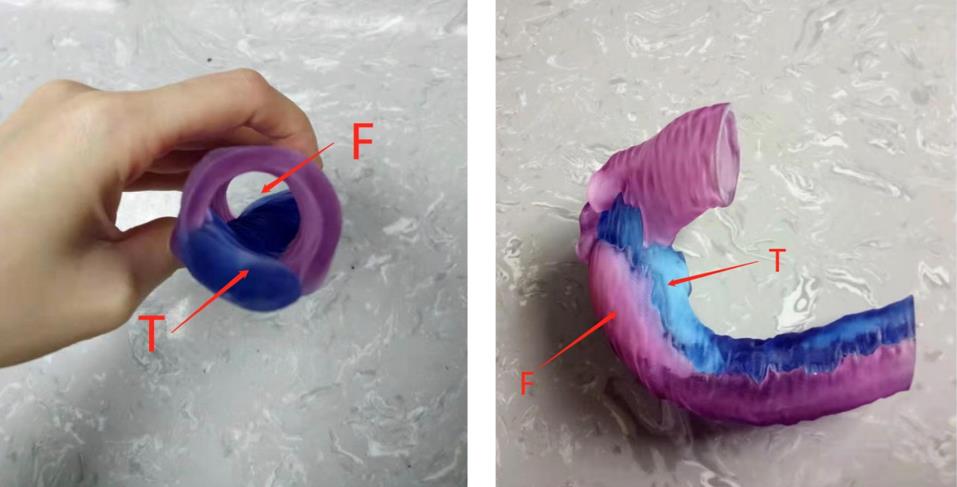

Fig.3
Intraoperative TEVAR stent release before and after"
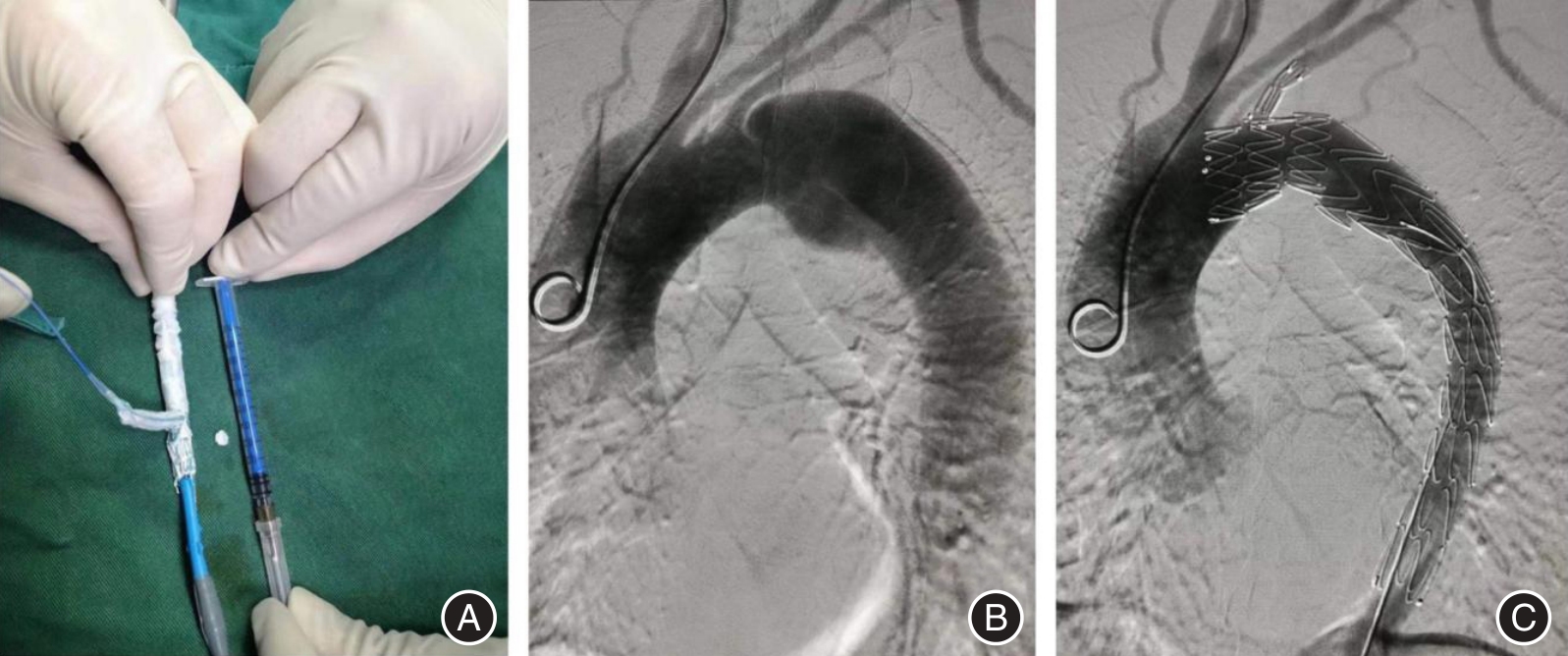

Fig.4
CTA and 3D model after TEVAR"
Tab.2
Comparison of surgical indicators between two groups of patients"
| 组别 | 例数 | 手术时间 (min) | 体外循环时间 (min) | 主动脉阻断时间 (min) | 手术出血量 (mL) | 术后气管插管时间 (h) | ICU停留时间 (h) |
|---|---|---|---|---|---|---|---|
| 模拟组 | 40 | 418.9 ± 67.8 | 224.6 ± 38.1 | 158.3 ± 22.0 | 784.8 ± 201.9 | 45.9 ± 9.4 | 92.8 ± 17.5 |
| 对照组 | 36 | 453.0 ± 72.4 | 247.3 ± 41.0 | 172.0 ± 24.3 | 811.3 ± 224.7 | 48.0 ± 11.2 | 103.6 ± 19.8 |
| t值 | -2.120 | -2.502 | -2.580 | -0.542 | -0.888 | -2.524 | |
| P值 | 0.037 | 0.015 | 0.012 | 0.590 | 0.377 | 0.014 |
Tab.3
Changes in true lumen diameter of the proximal aortic rupture plane, stent end plane, and abdominal trunk artery plane x ± s,mm"
| 指标 | 组别 | 术前 | 术后1个月 | 术后3个月 | 术后6个月 |
|---|---|---|---|---|---|
| 主动脉近端破口平面真腔内径 | 模拟组(n = 40) | 19.8 ± 3.6 | 32.7 ± 5.6* | 38.5 ± 5.9* | 41.0 ± 5.5* |
| 对照组(n = 36) | 20.5 ± 3.3 | 31.5 ± 5.5* | 36.4 ± 5.2* | 40.2 ± 4.8* | |
| F组间 = 0.910、F时间 = 74.201、F组间×时间 = 15.582 | |||||
| P组间 = 0.401、P时间 = 0.000、P组间×时间 = 0.000 | |||||
| 主动脉支架末端平面真腔内径 | 模拟组(n = 40) | 18.5 ± 4.0 | 24.5 ± 4.7* | 28.3 ± 3.8* | 30.5 ± 3.5* |
| 对照组(n = 36) | 17.8 ± 3.3 | 22.6 ± 3.5* | 26.9 ± 4.2* | 29.6 ± 4.1* | |
| F组间 = 1.104、F时间 = 48.662、F组间×时间 = 12.039 | |||||
| P组间 = 0.386、P时间 = 0.000、P组间×时间 = 0.000 | |||||
| 腹腔干动脉平面真腔内径 | 模拟组(n = 40) | 11.3 ± 2.5 | 13.2 ± 2.0* | 15.4 ± 2.2* | 15.5 ± 2.0* |
| 对照组(n = 36) | 10.8 ± 2.2 | 12.8 ± 2.1* | 14.9 ± 2.3* | 15.1 ± 2.2* | |
| F组间 = 1.361、F时间 = 14.209、F组间×时间 = 3.206 | |||||
| P组间 = 0.322、P时间 = 0.000、P组间×时间 = 0.720 | |||||

Fig.5
Histograms of true lumen diameter changes at the plane of proximal aortic rupture, stent end, and abdominal trunk arteryin two groups of patients"
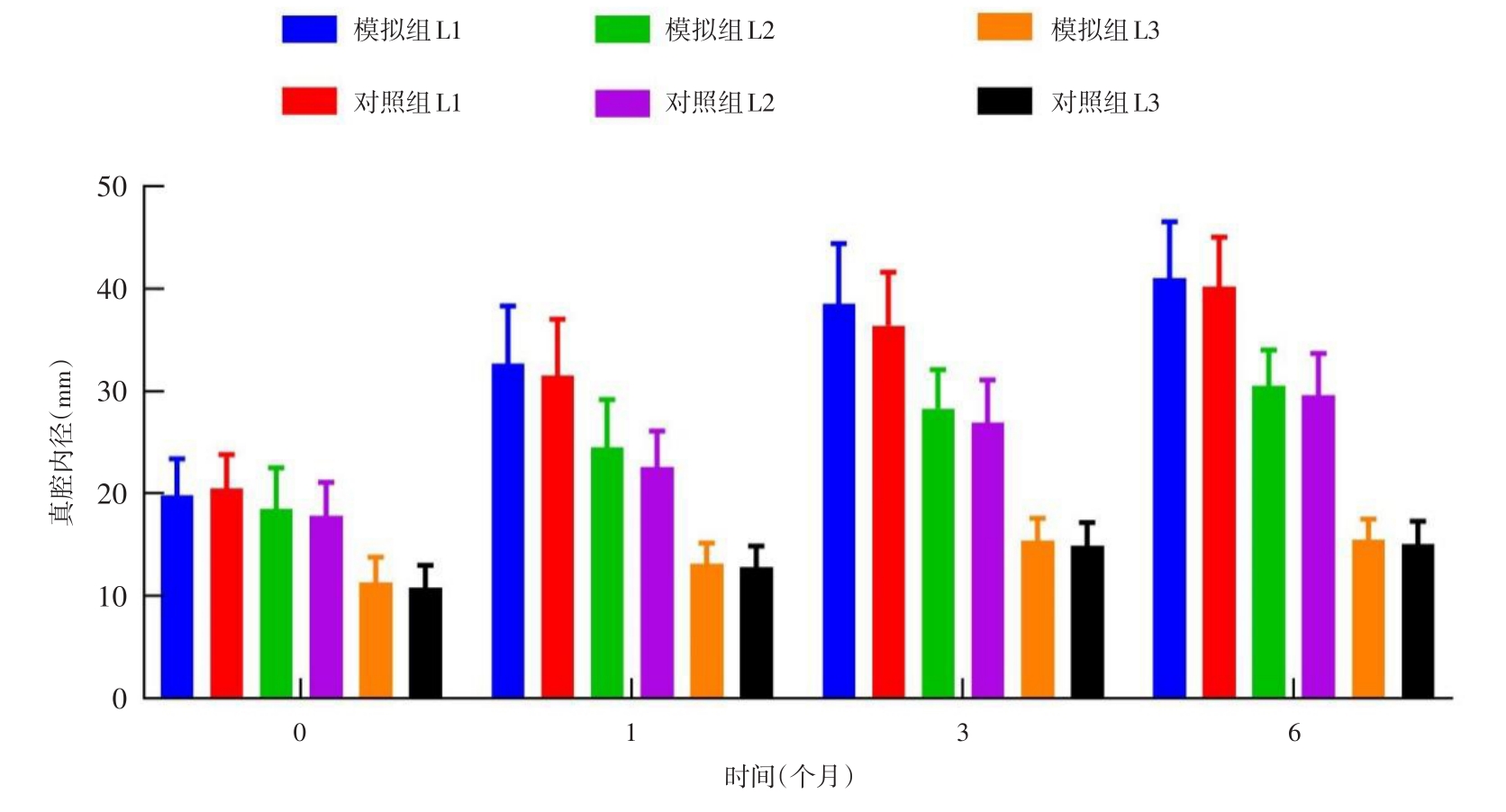

Fig.6
Histograms of the changes in false lumen inner diameter at the plane of proximal aortic rupture, stent end, and abdominal trunk artery in two groups of patients"
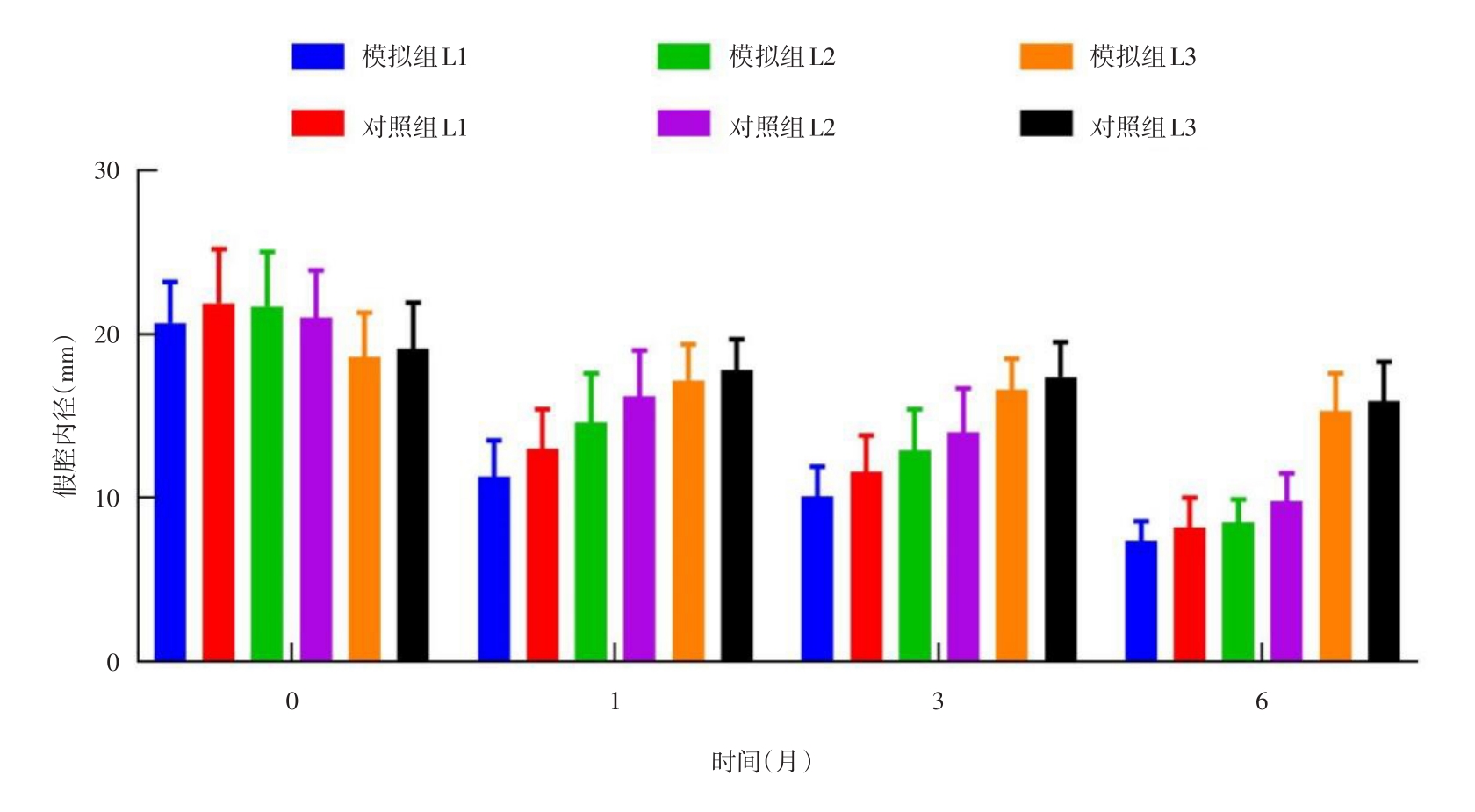
Tab.4
Changes in false lumen inner diameter at the plane of proximal aortic rupture, stent end plane, and abdominal trunk artery plane"
| 指标 | 组别 | 术前 | 术后1个月 | 术后3个月 | 术后6个月 |
|---|---|---|---|---|---|
| 主动脉近端破口平面假腔内径 | 模拟组(n = 40) | 20.7 ± 2.5 | 11.3 ± 2.2* | 10.1 ± 1.8* | 7.4 ± 1.2* |
| 对照组(n = 36) | 21.9 ± 3.3 | 13.0 ± 2.4* | 11.6 ± 2.2* | 8.2 ± 1.8* | |
| F组间 = 2.019、F时间 = 55.400、F组间×时间 = 14.293 | |||||
| P组间 = 0.183、P时间 = 0.000、P组间×时间 = 0.000 | |||||
| 主动脉支架末端平面假腔内径 | 模拟组(n = 40) | 21.7 ± 3.3 | 14.6 ± 3.0* | 12.9 ± 2.5* | 8.5 ± 1.4* |
| 对照组(n = 36) | 21.0 ± 2.9 | 16.2 ± 2.8* | 14.0 ± 2.7* | 9.8 ± 1.7* | |
| F组间 = 2.271、F时间 = 51.920、F组间×时间 = 15.514 | |||||
| P组间 = 0.166、P时间 = 0.000、P组间×时间 = 0.000 | |||||
| 腹腔干动脉平面假腔内径 | 模拟组(n = 40) | 18.6 ± 2.7 | 17.2 ± 2.2* | 16.6 ± 1.9* | 15.3 ± 2.3* |
| 对照组(n = 36) | 19.1 ± 2.8 | 17.8 ± 1.9* | 17.4 ± 2.1* | 15.9 ± 2.4* | |
| F组间 = 1.535、F时间 = 13.352、F组间×时间 = 2.961 | |||||
| P组间 = 0.310、P时间 = 0.000、P组间×时间 = 0.104 | |||||
Tab.5
Comparison of cardiac function indicators between two groups of patients"
| 组别 | 例数 | LVEF(%) | t值 | P值 | LVEDd(mm) | t值 | P值 | FS(%) | t值 | P值 | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 术前 | 术后6个月 | 术前 | 术后6个月 | 术前 | 术后6个月 | ||||||||
| 模拟组 | 40 | 53.9 ± 5.4 | 60.3 ± 4.8 | -5.436 | 0.000 | 50.8 ± 4.1 | 48.9 ± 4.5 | 1.926 | 0.058 | 26.5 ± 2.9 | 30.5 ± 3.4 | -5.534 | 0.000 |
| 对照组 | 36 | 52.5 ± 4.8 | 58.8 ± 5.1 | -5.547 | 0.000 | 52.1 ± 3.8 | 50.0 ± 4.8 | 1.518 | 0.133 | 27.4 ± 3.2 | 31.2 ± 3.8 | -4.731 | 0.000 |
| t值 | 1.189 | 1.321 | -1.429 | -1.593 | -1.286 | -0.848 | |||||||
| P值 | 0.238 | 0.191 | 0.157 | 0.115 | 0.202 | 0.399 | |||||||
Tab.6
Comparison of complication between two groups of patients"
| 组别 | 例数 | Ⅰ型内漏 | 脑梗死 | 肾功能损伤 | 胸腔积液 | 合计 |
|---|---|---|---|---|---|---|
| 模拟组 | 40 | 1 | 1 | 3 | 2 | 7(17.5) |
| 对照组 | 36 | 2 | 1 | 3 | 3 | 9(25.0) |
| χ2值 | 3.287 | |||||
| P值 | 0.07 |
| 1 |
唐前辉,陈靖,杨晗,等. Stanford B型主动脉夹层腔内治疗的血流动力学研究进展[J]. 实用医学杂志, 2022,38(14):1747-1752. doi:10.3969/j.issn.1006⁃5725.2022.14.007
doi: 10.3969/j.issn.1006?5725.2022.14.007 |
| 2 |
张雪花,董柱,毕生辉,等. 急性Stanford A型主动脉夹层术后行连续肾脏替代疗法的危险因素分析[J]. 实用医学杂志,2022,38(10):1226-1230. doi:10.3969/j.issn.1006-5725.2022.10.010
doi: 10.3969/j.issn.1006-5725.2022.10.010 |
| 3 |
张勇,梁家立,郑德志,等. 无冠窦补片在Standford A型主动脉夹层根部成形中的应用[J]. 实用医学杂志, 2021,37(6):778-781. doi:10.3969/j.issn.1006-5725.2021.06.018
doi: 10.3969/j.issn.1006-5725.2021.06.018 |
| 4 |
GEORGE M J, DIAS-NETO M, RAMOS TENORIO E, et al. 3D printing in aortic endovascular therapies[J]. J Cardiovasc Surg (Torino), 2022,63(5):597-605. doi:10.23736/s0021-9509.22.12407-9
doi: 10.23736/s0021-9509.22.12407-9 |
| 5 |
SUN W, XU H, XIONG J, et al. 3D Morphologic Findings Before and After Thoracic Endovascular Aortic Repair for Type B Aortic Dissection[J]. Ann Vasc Surg, 2021,74:220-228. doi:10.1016/j.avsg.2020.12.026
doi: 10.1016/j.avsg.2020.12.026 |
| 6 |
ERBEL R, ABOYANS V, BOILEAU C, et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC)[J]. Eur Heart J, 2014,35(41):2873-926. doi:10.1093/eurheartj/ehu281
doi: 10.1093/eurheartj/ehu281 |
| 7 |
JURASZEK A, CZERNY M, RYLSKI B. Update in aortic dissection[J]. Trends Cardiovasc Med, 2022,32(7):456-461. doi:10.1016/j.tcm.2021.08.008
doi: 10.1016/j.tcm.2021.08.008 |
| 8 |
MUNSHI B, RITTER J C, DOYLE B J,et al Management of acute type B aortic dissection[J]. ANZ J Surg, 2020,90(12):2425-2433. doi:10.1111/ans.16270
doi: 10.1111/ans.16270 |
| 9 |
TAN S Z C P, SANTAWY H EL, ABDELHALIEM A. Is TEVAR really needed for uncomplicated type B aortic dissection?[J] J Card Surg, 2021,36(10):3831-3833. doi:10.1111/jocs.15828
doi: 10.1111/jocs.15828 |
| 10 |
LOMBARDI J V, HUGHES G C, APPOO J J, et al. Society for Vascular Surgery (SVS) and Society of Thoracic Surgeons (STS) reporting standards for type B aortic dissections[J]. J Vasc Surg,2020,71(3):723-747. doi:10.1016/j.jvs.2019.11.013
doi: 10.1016/j.jvs.2019.11.013 |
| 11 |
XU H, XIONG J, HAN X, et al. Computed tomography-based hemodynamic index for aortic dissection[J]. J Thorac Cardiovasc Surg, 2021,162(2):e165-e176. doi:10.1016/j.jtcvs.2020.02.034
doi: 10.1016/j.jtcvs.2020.02.034 |
| 12 |
WANG J, LI M, LI J, et al. Safety and efficacy of thoracic endovascular aortic repair for acute Stanford type B aortic dissection with retrograde type A intramural hematoma[J]. J Vasc Surg,2023,78(1):61-69.e4. doi:10.1016/j.jvs.2023.02.021
doi: 10.1016/j.jvs.2023.02.021 |
| 13 |
TONG Y H, YU T, ZHOU M J, et al. Use of 3D Printing to Guide Creation of Fenestrations in Physician-Modified Stent-Grafts for Treatment of Thoracoabdominal Aortic Disease[J]. J Endovasc Ther, 2020,27(3):385-393. doi:10.1177/1526602820917960
doi: 10.1177/1526602820917960 |
| 14 |
SHAD R, KONG S, FONG R,et al. Computational Fluid Dynamics Simulations to Predict False Lumen Enlargement After Surgical Repair of Type-A Aortic Dissection[J]. Semin Thorac Cardiovasc Surg, 2022,34(2):443-448. doi:10.1053/j.semtcvs.2021.05.012
doi: 10.1053/j.semtcvs.2021.05.012 |
| 15 | MARROCCO-TRISCHITTA M M, STURLA F. Blood flow helical pattern in type Ⅲ arch configuration as a potential risk factor for type B aortic dissection[J]. Eur J Cardiothorac Surg, 2021,61(1):132-139. |
| 16 |
LI X R, TONG Y H, LI X Q, et al. Total endovascular repair of an intraoperative stent-graft deployed in the false lumen of Stanford type A aortic dissection: A case report[J]. World J Clin Cases, 2020,8(5):954-962. doi:10.12998/wjcc.v8.i5.954
doi: 10.12998/wjcc.v8.i5.954 |
| 17 | 张昊,张雷,魏小龙,等. Castor分支型主动脉覆膜支架治疗Stanford B型主动脉夹层的单中心中期疗效评估[J]. 上海医学, 2022, 45(10):699-703. |
| 18 |
黄飞来,杨广林,毕乐昌,等. 非复杂性Stanford B型主动脉夹层腔内修复术的时机选择研究[J]. 浙江创伤外科, 2022,27(6):1097-1098. doi:10.3969/j.issn.1009-7147.2022.06.037
doi: 10.3969/j.issn.1009-7147.2022.06.037 |
| 19 |
RIGHINI P, SECCHI F, MAZZACCARO D, et al. Four-Dimensional Flow MRI for the Evaluation of Aortic Endovascular Graft: A Pilot Study[J]. Diagnostics (Basel), 2023,13(12):2113. doi:10.3390/diagnostics13122113
doi: 10.3390/diagnostics13122113 |
| 20 |
SAADE W, VINCIGUERRA M, ROMITI S,et al. 3D morphometric analysis of ascending aorta as an adjunctive tool to predict type A acute aortic dissection[J]. J Thorac Dis, 2021,13(6):3443-3457. doi:10.21037/jtd-21-119
doi: 10.21037/jtd-21-119 |
| 21 |
代承忠,肖鹏,王浩东. 主动脉几何构型对Stanford B型主动脉夹层腔内修复术后围手术期支架周围假腔残留的预测价值[J]. 中国中西医结合影像学杂志, 2021,19(5):413-417. doi:10.3969/j.issn.1672-0512.2021.05.002
doi: 10.3969/j.issn.1672-0512.2021.05.002 |
| 22 |
ZHOU J, XU J, WANG X, et al. Personalized 3D-print-covered stent for endovascular treatment of complicated abdominal aortic dissection with Marfan syndrome[J]. Asian J Surg, 2023,46(3):1387-1389. doi:10.1016/j.asjsur.2022.08.128
doi: 10.1016/j.asjsur.2022.08.128 |
| 23 |
唐前辉,陈靖,杨晗,等. Stanford B型主动脉夹层腔内治疗的血流动力学研究进展[J]. 实用医学杂志, 2022,38(14):1747-1752. doi:10.3969/j.issn.1006⁃5725.2022.14.007
doi: 10.3969/j.issn.1006?5725.2022.14.007 |
| 24 | 吴励,韦亚宁,曾岸轲,等. CTA多模式3D打印制作Stanford B型主动脉夹层模型[J]. 中国医学影像技术, 2023,39(1):134-136. |
| 25 |
ISMAGUILOVA A, MARTUFI G, GREGORY A J,et al. Multidimensional Analysis of Descending Aortic Growth After Acute Type A Aortic Dissection[J]. Ann Thorac Surg, 2021,111(2):615-621. doi:10.1016/j.athoracsur.2020.04.064
doi: 10.1016/j.athoracsur.2020.04.064 |
| [1] | Bing LIU,Hanxi CHEN,Wenji LIU,Yingwen HUANG,Yan WANG,Chan HUANG,Tianhui. YOU. Impacts of illness perception and coping style on social participation in patients receiving surgery for Stanford type A aortic dissection [J]. The Journal of Practical Medicine, 2024, 40(8): 1160-1166. |
| [2] | Cui JI,Qinying WANG,Lei WANG,Yuan. WANG. Effect of cognitive⁃behavioral intervention under the family⁃based care model on continuing care of patients after aortic dissection surgery [J]. The Journal of Practical Medicine, 2024, 40(4): 566-570. |
| [3] | Runwei MA,Chunjie MU,Wenting GUI,Yao DENG,Minzhang ZHAO,Min LIU,Yi SONG. LncRNA SENCR targeted miR⁃206 regulates proliferation and apoptosis of human vascular smooth muscle cells of aortic dissection tissues [J]. The Journal of Practical Medicine, 2024, 40(3): 302-308. |
| [4] |
ZHANG Hao, ZHANG Yu, XIAO Shining, LIU Jiaming..
Experimental research progress of 3D printing bionic scaffold in repairing of spinal cord injury [J]. The Journal of Practical Medicine, 2022, 38(22): 2868-2873. |
| [5] |
HONG Miaoxuan, ZHANG Rong, ZHU Jin, LAI Jing, TAN Wenxuan..
Mediating effect of self ⁃efficacy between social support and resilience in type A aortic dissection patients [J]. The Journal of Practical Medicine, 2022, 38(16): 2056-2060. |
| [6] |
TANG Qianhui, CHEN Jing, YANG Han, QIN Xiao..
Research progress of hemodynamic in endovascular treatment for type B aortic dissection [J]. The Journal of Practical Medicine, 2022, 38(14): 1747-1752. |
| [7] |
ZHANG Xuehua, DONG Zhu, BI Shenghui, YU Xuefei, LI Yaling, YANG Bo, WANG Xiaowu..
Analysis of risk factors and prevention strategies for CRRT after acute Stanford Type A aortic dissection surgery [J]. The Journal of Practical Medicine, 2022, 38(10): 1226-1230. |
| [8] |
ZHANG Yong, LIANG Jiali, ZHENG Dezhi, WANG Hui, HOU Jun.
Application of non coronary sinus patch in the root plasty of Stanford type A aortic dissection [J]. The Journal of Practical Medicine, 2021, 37(6): 778-781. |
| [9] |
JIANG Yixiao, HUANG Bo, WANG Yuchuan, CHEN Xiahuan, LIU Meilin..
Clinical application of quantitative Allen′s test and simplified Allen′s test before the interventional therapy via radial artery [J]. The Journal of Practical Medicine, 2021, 37(15): 1944-1947. |
| [10] | QIN Qi, FENG Mengzhao, WANG Pengfei, DONG Hui. . Clinical application of 3D printing technology in infantile craniostenosis surgery [J]. The Journal of Practical Medicine, 2021, 37(14): 1883-1886. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||