实用医学杂志 ›› 2025, Vol. 41 ›› Issue (23): 3723-3729.doi: 10.3969/j.issn.1006-5725.2025.23.014
• 临床研究 • 上一篇
魏义1,饶春晖1,刘慧泽1,陈文2
Yi WEI1,Chunhui RAO1,Huize LIU1,Wen. CHEN2
摘要:
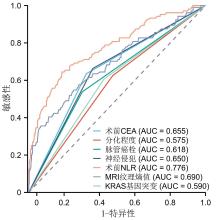
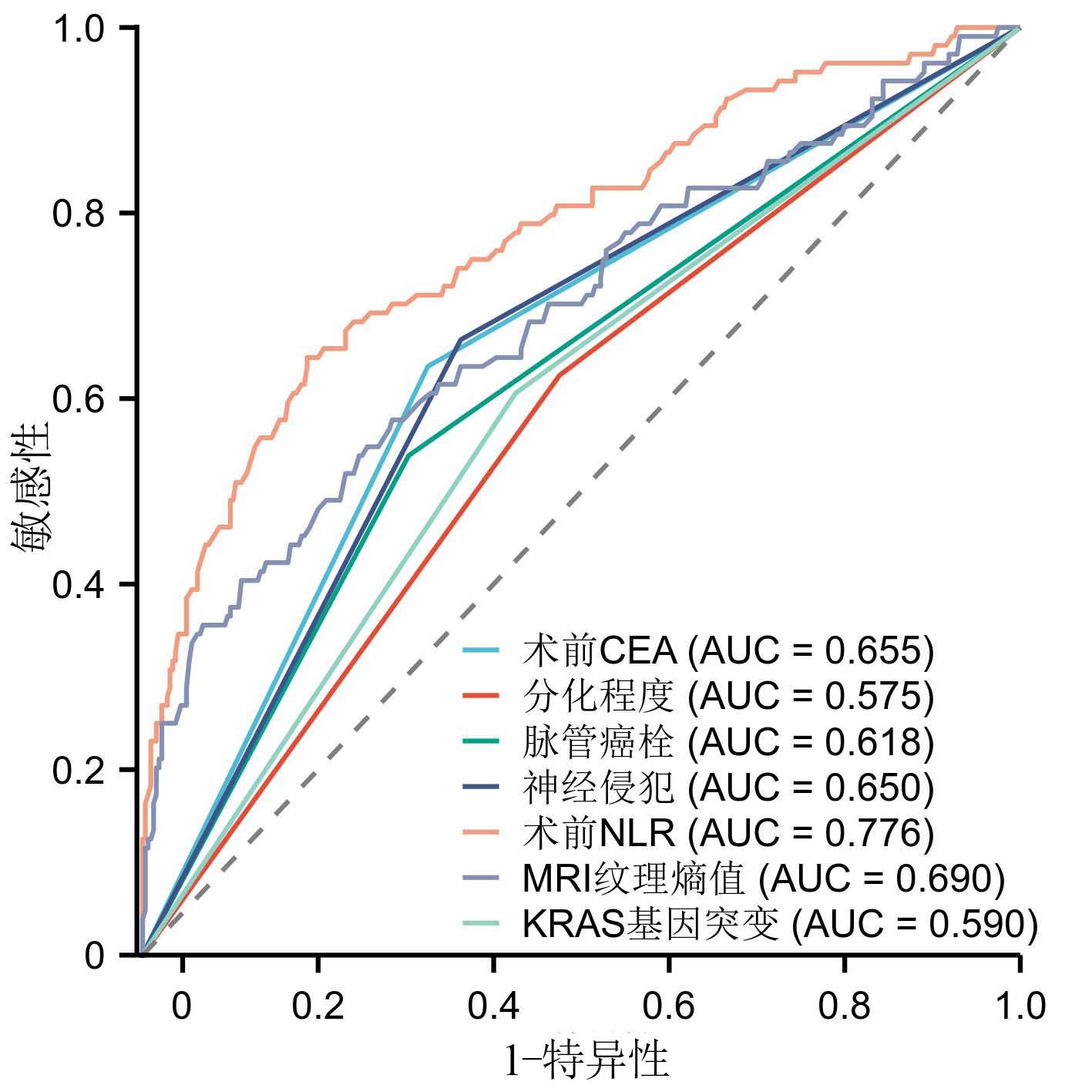
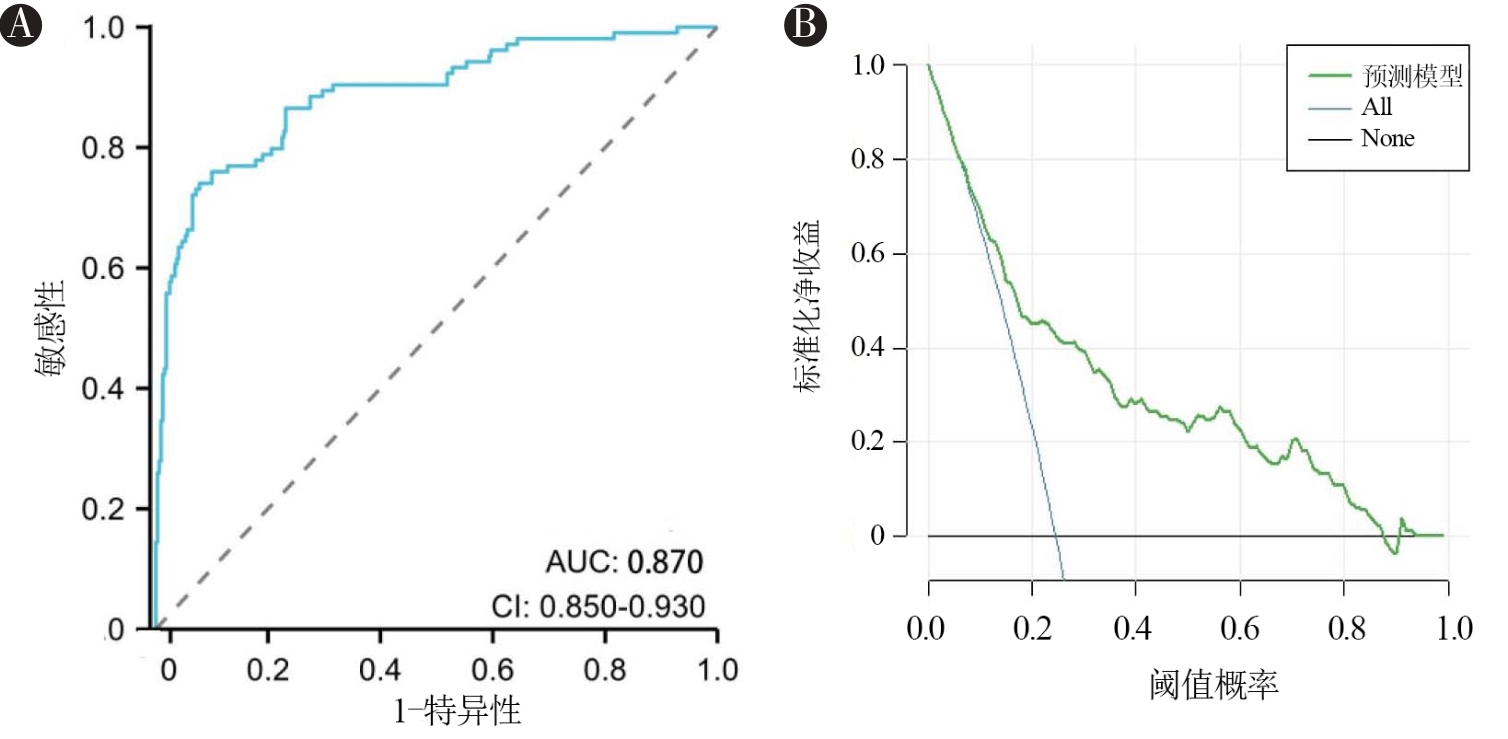
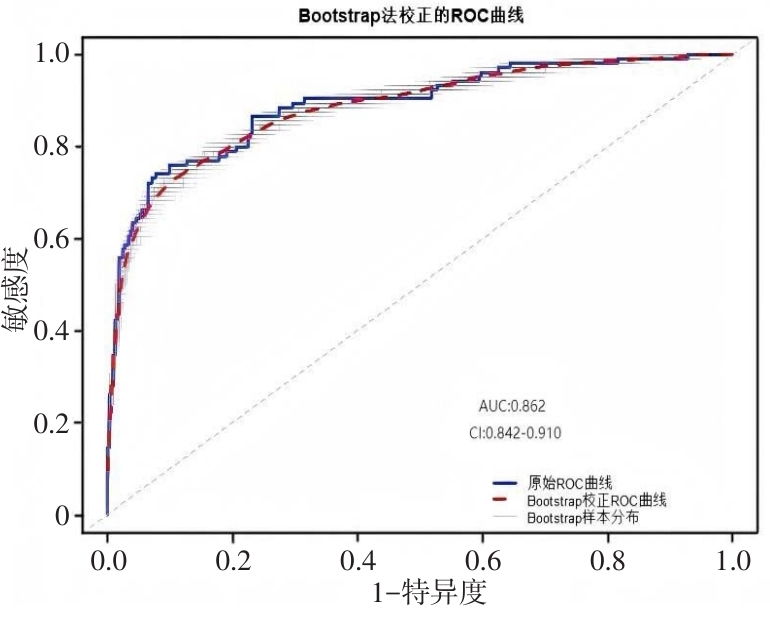
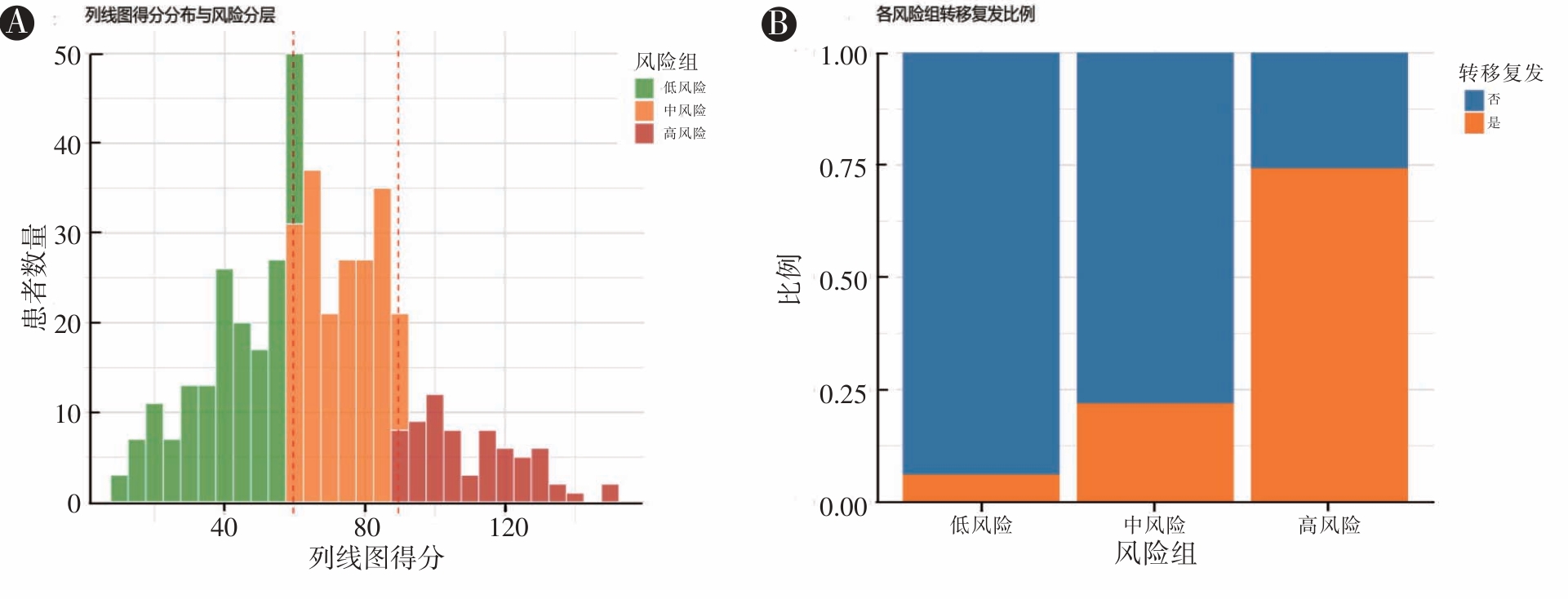
目的 构建多模态列线图预测未辅助治疗的Ⅱ期结直肠癌(CRC)患者术后转移复发风险。 方法 回顾性纳入2016年1月至2021年12月于本院行根治性手术的Ⅱ期CRC未辅助治疗患者424例。提取患者临床病理特征(T分期、CEA、分化程度等)、炎症指标(术前中性粒细胞计数与淋巴细胞计数比值、术前淋巴细胞计数与单核细胞计数比值)、影像组学参数(MRI纹理熵值)及分子标志物(KRAS突变状态)。以影像学证实的转移复发为主要终点,通过单因素及多因素logistic回归分析筛选独立危险因素,构建列线图模型,ROC曲线分析模型的预测价值,Bootstrap法进行内部验证,Hosmer-Lemeshow拟合优度检验评价模型的校准度,绘制决策曲线分析,检验模型获益,并进行风险分层。 结果 104例(24.53%)患者术后3年内发生转移复发。多因素分析显示:CEA > 5 μg/L、中低分化、有脉管癌栓、有神经侵犯、NLR升高、熵值升高、有KRAS基因突变为独立危险因素(P < 0.05)。基于上述因素构建的列线图预测效能显著(AUC = 0.870,95%CI: 0.850 ~ 0.930),校准曲线显示模型拟合良好。风险分层后:低危组复发率仅6.1%,而高危组达74.2%(P < 0.05)。 结论 在未辅助治疗Ⅱ期CRC人群中构建的临床-炎症-影像组学联合预测模型,可用于识别该类患者术后转移复发风险。
中图分类号: