

The Journal of Practical Medicine ›› 2026, Vol. 42 ›› Issue (10): 1712-1719.doi: 10.3969/j.issn.1006-5725.2026.10.004
• Feature Reports:Diabetes Mellitus • Previous Articles
Yukun ZHAO,Guojing ZHAO,Ruiqing DONG,Wei QIANG,Hui GUO,Heping LI( )
)
Received:2025-12-05
Online:2026-05-25
Published:2026-05-27
Contact:
Heping LI
E-mail:Lhp_0123@126.com
CLC Number:
Yukun ZHAO,Guojing ZHAO,Ruiqing DONG,Wei QIANG,Hui GUO,Heping LI. A comparative study on clinical outcomes of hospitalized patients with type 2 diabetes mellitus transitioning from continuous subcutaneous insulin infusion (CSII) to insulin degludec-based regimens based on continuous glucose monitoring[J]. The Journal of Practical Medicine, 2026, 42(10): 1712-1719.
Tab.1
Demographic and clinical characteristics of three patient groups"
| 项目 | IDeg (n = 35) | IDegAsp(n = 37) | IDegLira(n = 38) | F/H/χ2值 | P值 |
|---|---|---|---|---|---|
| 年龄( | 52.00 ± 16.04 | 52.06 ± 14.35 | 56.84 ± 9.54 | 1.58 | 0.211 |
| 性别 | 1.46 | 0.482 | |||
| 男 | 26(74.3) | 31(83.8) | 32(84.2) | ||
| 女 | 9(25.7) | 6(16.2) | 6(15.8) | ||
| BMI( | 24.28 ± 3.00 | 22.86 ± 5.01 | 25.60 ± 2.45 | 5.20 | 0.007 |
| 病程[M(P25,P75)]/月 | 60.00(5.00,180.00) | 48.00(12.00,120.00) | 90.00(45.00,159.00) | 2.79 | 0.248 |
| HbA1c( | 10.78 ± 1.34 | 10.70 ± 1.32 | 10.51 ± 1.39 | 2.56 | 0.082 |
| 糖尿病性肾病 | 15(42.9) | 12(32.4) | 8(21.1) | 4.00 | 0.135 |
| 糖尿病性视网膜病变 | 8(22.9) | 8(21.6) | 4(10.5) | 2.30 | 0.316 |
| 周围血管病变 | 26(74.3) | 21(56.8) | 37(97.4) | 17.25 | < 0.001 |
| 糖尿病足 | 2(5.7) | 2(5.4) | 0(0.0) | 2.19 | 0.334 |
| 入院前用药 | 9.51 | 0.301 | |||
| 未用药 | 9(25.7) | 14(37.8) | 8(21.1) | ||
| 口服降糖药 | 13(37.1) | 12(32.4) | 8(21.1) | ||
| 胰岛素±口服药 | 12(34.3) | 11(29.7) | 19(50.0) | ||
| GLP-1RA±口服药 | 0(0.0) | 0(0.0) | 9(23.7) | ||
| 胰岛素+GLP-1RA±口服药 | 1(2.9) | 0(0.0) | 2(5.3) | ||
| 入院前用药种类 | 9.35 | 0.155 | |||
| 0 | 9(25.7) | 14(37.8) | 8(21.1) | ||
| 1 | 12(34.3) | 8(21.6) | 8(21.1) | ||
| 2 | 8(22.9) | 6(16.2) | 16(42.1) | ||
| 3种及以上 | 6(17.1) | 9(24.3) | 6(15.8) | ||
| 高血压 | 7(20.0) | 3(8.1) | 8(21.1) | 2.79 | 0.248 |
| 冠心病 | 2(5.7) | 3(8.1) | 4(10.5) | 0.57 | 0.751 |
| 脂肪肝 | 8(22.9) | 4(10.8) | 12(31.6) | 4.77 | 0.092 |
| 糖尿病家族史 | 8(22.9) | 11(29.7) | 10(26.3) | 0.46 | 0.796 |
Tab.2
Comparison of CGM parameters before and after treatment protocol transition"
| 项目 | 胰岛素泵期间 | 转换后 | P值 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| IDeg(n = 35) | IDegAsp(n = 37) | IDegLira(n = 38) | IDeg(n = 35) | IDegAsp(n = 37) | IDegLira(n = 38) | P1 | P2 | P3 | P4 | |
| GMI/% | 8.05±1.29 | 7.30±0.59 | 7.35±0.69 | 7.28±1.18 | 6.75±0.86 | 6.59±0.49 | 0.001 | <0.001 | <0.001 | 0.003 |
| MG/(mmol/L) | 11.01±3.00 | 9.27±1.37 | 9.38±1.60 | 9.21±2.74 | 7.99±2.00 | 7.62±1.14 | 0.001 | <0.001 | <0.001 | 0.003 |
| CV/% | 32.66±6.18 | 32.38±4.96 | 31.58±6.68 | 30.60±6.86 | 27.22±5.76 | 25.61±5.51 | 0.045 | <0.001 | <0.001 | <0.001 |
| SD/(mmol/L) | 3.57±1.09 | 2.99±0.54 | 2.97±0.79 | 2.81±0.94 | 2.18±0.72 | 1.97±0.55 | 0.001 | <0.001 | <0.001 | <0.001 |
| TIR*/% | 48.67±22.42 | 63.20±16.10 | 63.87±17.68 | 64.44±24.06 | 78.26±20.44 | 84.89±12.45 | <0.001 | <0.001 | <0.001 | <0.001 |
| TITR#/% | 26.82±19.44 | 38.51±17.58 | 40.32±21.61 | 43.80±24.71 | 56.86±23.15 | 61.45±20.58 | <0.001 | <0.001 | <0.001 | 0.004 |
| TAR▲/% | 50.52±23.13 | 35.54±16.86 | 35.52±18.30 | 34.13±24.22 | 20.13±21.04 | 14.64±12.69 | <0.001 | <0.001 | <0.001 | <0.001 |
TBR● [M(P25,P75)]/% | 0.00(0.00,0.01) | 0.00(0.00,0.02) | 0.00(0.00,0.00) | 0.01(0.00,0.02) | 0.00(0.00,0.02) | 0.00(0.00,0.01) | 0.009 | 0.929 | 0.972 | 0.020 |
| TIR-TITR/% | 21.85±9.01 | 24.69±5.64 | 23.55±8.14 | 20.64±10.05 | 21.40±12.27 | 23.44±11.19 | 0.441 | 0.145 | 0.939 | 0.543 |
| LBGI | 1.62±1.30 | 1.74±1.82 | 1.17±1.08 | 1.99±1.32 | 1.64±1.28 | 1.07±0.69 | 0.237 | 0.729 | 0.442 | 0.004 |
| HBGI | 15.20±10.21 | 9.39±3.31 | 9.67±4.28 | 10.07±8.83 | 6.06±5.49 | 4.49±2.40 | 0.005 | <0.001 | <0.001 | 0.002 |
| ADRR | 14.20±10.45 | 8.38±3.48 | 8.67±4.19 | 9.08±8.79 | 5.53±5.31 | 3.76±2.26 | 0.006 | 0.002 | <0.001 | 0.002 |
| MODD(mmol/L) | 3.22±1.11 | 2.75±0.68 | 2.76±0.84 | 2.56±0.97 | 2.06±0.93 | 1.74±0.52 | 0.002 | <0.001 | <0.001 | <0.001 |
| CV夜间/% | 24.38±8.41 | 25.75±8.07 | 25.67±9.07 | 24.27±10.33 | 21.93±8.34 | 17.77±5.69 | 0.961 | 0.041 | <0.001 | 0.025 |
| CV白天/% | 32.66±6.18 | 31.83±4.62 | 31.22±6.49 | 29.66±6.23 | 27.04±5.15 | 25.24±4.68 | 0.002 | <0.001 | <0.001 | 0.014 |
| CVFBS/% | 37.43±26.49 | 37.17±13.75 | 28.10±10.77 | 26.49±12.73 | 21.07±8.84 | 21.18±9.35 | 0.003 | <0.001 | 0.006 | 0.139 |

Fig.1
Distribution of nocturnal blood glucose trough values"
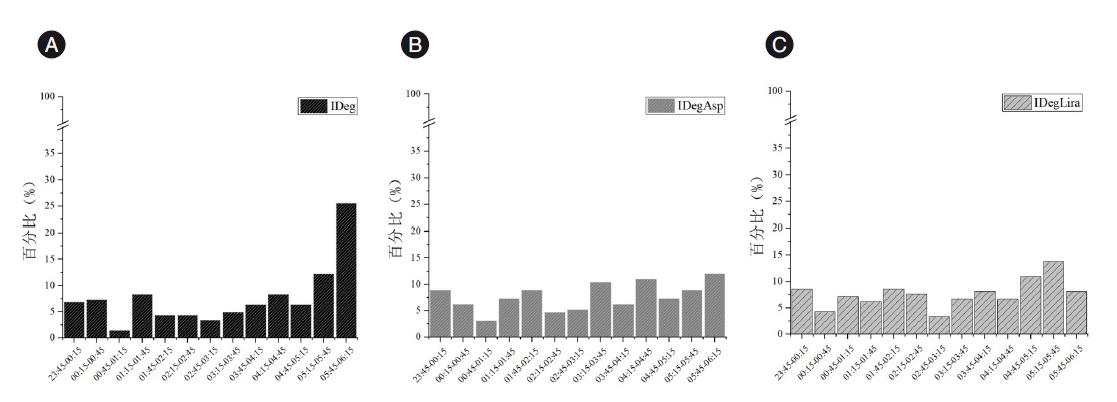

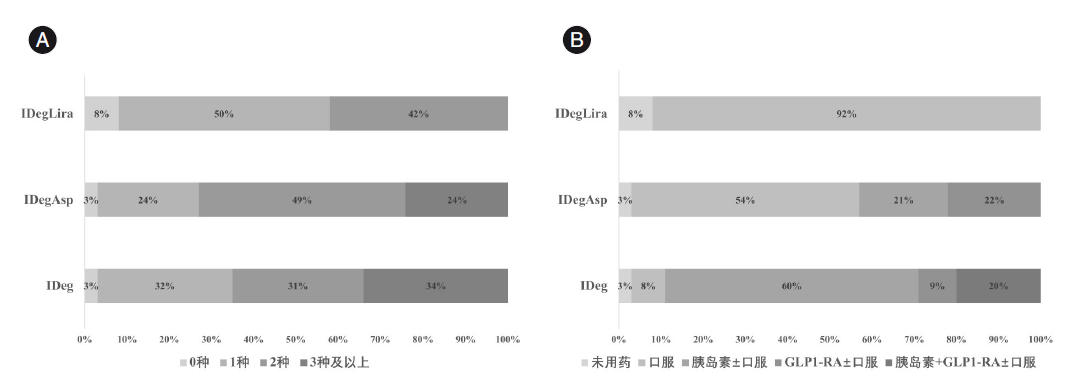
Fig.2
Post-discharge combination therapy status"
| [1] |
叶健华, 赵玉钏. 2型糖尿病缓解标准与治疗策略[J]. 实用医学杂志, 2023, 39(14): 1729-1732. doi:10.3969/j.issn.1006-5725.2023.14.001 .
doi: 10.3969/j.issn.1006-5725.2023.14.001 |
| [2] |
中华医学会糖尿病学分会. 中国2型糖尿病防治指南(2013年版)[J]. 中国糖尿病杂志, 2014, 22(8): 后插2-后插42. doi:10.3969/j.issn.1006-6187.2014.08.027 .
doi: 10.3969/j.issn.1006-6187.2014.08.027 |
| [3] |
刘烈华, 李延兵. 2型糖尿病的缓解: 百家争鸣与脚踏实地[J]. 实用医学杂志, 2024, 40(16): 2206-2210. doi:10.3969/j.issn.1006-5725.2024.16.002 .
doi: 10.3969/j.issn.1006-5725.2024.16.002 |
| [4] |
HINNEN D A. Therapeutic options for the management of postprandial glucose in patients with type 2 diabetes on basal insulin[J]. Clin Diabetes, 2015, 33(4): 175-180. doi:10.2337/diaclin.33.4.175 .
doi: 10.2337/diaclin.33.4.175 |
| [5] |
MOSENZON O, RAZ I. Intensification of insulin therapy for type 2 diabetic patients in primary care: Basal-bolus regimen versus premix insulin analogs: When and for whom?[J]. Diabetes Care, 2013, 36(): S212-S218. doi:10.2337/dcS13-2007 .
doi: 10.2337/dcS13-2007 |
| [6] |
SAISHO Y. β-cell dysfunction: Its critical role in prevention and management of type 2 diabetes[J]. World J Diabetes, 2015, 6(1): 109-124. doi:10.4239/wjd.v6.i1.109 .
doi: 10.4239/wjd.v6.i1.109 |
| [7] |
KATAOKA M, VENN B J, WILLIAMS S M, et al. Glycaemic responses to glucose and rice in people of Chinese and European ethnicity[J]. Diabet Med, 2013, 30(3): e101-e107. doi:10.1111/dme.12080 .
doi: 10.1111/dme.12080 |
| [8] |
PHILIS-TSIMIKAS A, ASTAMIROVA K, GUPTA Y, et al. Similar glycaemic control with less nocturnal hypoglycaemia in a 38-week trial comparing the IDegAsp co-formulation with insulin glargine U100 and insulin aspart in basal insulin-treated subjects with type 2 diabetes mellitus[J]. Diabetes Res Clin Pract, 2019, 147: 157-165. doi:10.1016/j.diabres.2018.10.024 .
doi: 10.1016/j.diabres.2018.10.024 |
| [9] |
LUO Q, ZHOU L, ZHOU N, et al. Cost-effectiveness of insulin degludec/insulin aspart versus biphasic insulin aspart in Chinese population with type 2 diabetes[J]. Front Public Health, 2022, 10: 1016937. doi:10.3389/fpubh.2022.1016937 .
doi: 10.3389/fpubh.2022.1016937 |
| [10] |
KAWAGUCHI Y, MIYAMOTO S, HAJIKA Y, et al. Efficacy of IDegLira versus IDegAsp therapy in patients with type 2 diabetes: A randomized crossover study by isCGM[J]. Adv Ther, 2022, 39(6): 2688-2700. doi:10.1007/s12325-022-02138-w .
doi: 10.1007/s12325-022-02138-w |
| [11] |
KING A B, PHILIS-TSIMIKAS A, KILPATRICK E S, et al. A fixed ratio combination of insulin degludec and liraglutide (IDegLira) reduces glycemic fluctuation and brings more patients with type 2 diabetes within blood glucose target ranges[J]. Diabetes Technol Ther, 2017, 19(4): 255-264. doi:10.1089/dia.2016.0405 .
doi: 10.1089/dia.2016.0405 |
| [12] |
CHEN M, ZHANG P, ZHAO Y, et al. Where to initiate basal insulin therapy: Inpatient or outpatient department? real-world observation in China[J]. Diabetes Metab Syndr Obes, 2022, 15: 3375-3385. doi:10.2147/DMSO.S386230 .
doi: 10.2147/DMSO.S386230 |
| [13] |
BROD M, ALOLGA S L, MENEGHINI L. Barriers to initiating insulin in type 2 diabetes patients: Development of a new patient education tool to address myths, misconceptions and clinical realities[J]. Patient, 2014, 7(4): 437-450. doi:10.1007/s40271-014-0068-x .
doi: 10.1007/s40271-014-0068-x |
| [14] |
中华医学会内分泌学分会, 中华医学会糖尿病学分会, 中国医师协会内分泌代谢科医师分会. 中国胰岛素泵治疗指南(2021年版)[J]. 中华内分泌代谢杂志, 2021, 37(8): 679-701. doi:10.3760/cma.j.cn311282-20210428-00265 .
doi: 10.3760/cma.j.cn311282-20210428-00265 |
| [15] |
QIANG W, LI M, SONG S, et al. Initiation of insulin degludec in Chinese hospitalized patients with type 2 diabetes-a single center’s experience[J]. Diabetes Metab Syndr Obes, 2024, 17: 3535-3546. doi:10.2147/DMSO.S468070 .
doi: 10.2147/DMSO.S468070 |
| [16] |
DANNE T, NIMRI R, BATTELINO T, et al. International consensus on use of continuous glucose monitoring[J]. Diabetes Care, 2017, 40(12): 1631-1640. doi:10.2337/dc17-1600 .
doi: 10.2337/dc17-1600 |
| [17] |
FRONTONI S, DI BARTOLO P, AVOGARO A, et al. Glucose variability: An emerging target for the treatment of diabetes mellitus[J]. Diabetes Res Clin Pract, 2013, 102(2): 86-95. doi:10.1016/j.diabres.2013.09.007 .
doi: 10.1016/j.diabres.2013.09.007 |
| [18] |
KONG A P S, LIM S, YOO S H, et al. Asia-Pacific consensus recommendations for application of continuous glucose monitoring in diabetes management[J]. Diabetes Res Clin Pract, 2023, 201: 110718. doi:10.1016/j.diabres.2023.110718 .
doi: 10.1016/j.diabres.2023.110718 |
| [19] |
中华医学会糖尿病学分会. 中国血糖监测临床应用指南(2011年版)[J]. 中华医学杂志, 2011, 91(10): 656-664. doi:10.3760/cma.j.issn.0376-2491.2011.10.003
doi: 10.3760/cma.j.issn.0376-2491.2011.10.003 |
| [20] |
ELSAYED N A, ALEPPO G, BANNURU R R, et al. 9. pharmacologic approaches to glycemic treatment: Standards of care in diabetes—2024 [J]. Diabetes Care, 2024, 47(): S158-S178. doi:10.2337/dc24-s009 .
doi: 10.2337/dc24-s009 |
| [21] |
SEBASTIAN S A, CO E L, MEHENDALE M, et al. Insulin analogs in the treatment of type II diabetes and future perspectives[J]. Dis Mon, 2023, 69(3): 101417. doi:10.1016/j.disamonth.2022.101417 .
doi: 10.1016/j.disamonth.2022.101417 |
| [22] |
GOLDENBERG R M, ARODA V R, BILLINGS L K, et al. Effect of insulin degludec versus insulin glargine U100 on time in range: SWITCH PRO, a crossover study of basal insulin-treated adults with type 2 diabetes and risk factors for hypoglycaemia[J]. Diabetes Obes Metab, 2021, 23(11): 2572-2581. doi:10.1111/dom.14504 .
doi: 10.1111/dom.14504 |
| [23] |
ROSENSTOCK J, BAJAJ H S, LINGVAY I, et al. Clinical perspectives on the frequency of hypoglycemia in treat-to-target randomized controlled trials comparing basal insulin analogs in type 2 diabetes: A narrative review[J]. BMJ Open Diabetes Res Care, 2024, 12(3): e003930. doi:10.1136/bmjdrc-2023-003930 .
doi: 10.1136/bmjdrc-2023-003930 |
| [24] | 中华医学会内分泌学分会, 国家高性能医疗器械创新中心, 纪立农, 等. 动态葡萄糖图谱报告临床应用专家共识(2023版)[J]. 中华糖尿病杂志, 2024, 16(2): 190-201. |
| [25] |
FADINI G P, BUZZETTI R, FITTIPALDI M R, et al. IDegLira for the real-world treatment of type 2 diabetes in Italy: Protocol and interim results from the REX observational study[J]. Diabetes Ther, 2022, 13(8): 1483-1497. doi:10.1007/s13300-022-01287-z .
doi: 10.1007/s13300-022-01287-z |
| [26] |
WANG R, LUO S, XIAO Z, et al. Efficacy and safety of fixed-ratio combination insulin degludec/liraglutide in type 2 diabetes: A systematic review and meta-analysis of randomised controlled trials[J]. Diabetes Metab Res Rev, 2024, 40(3): e3752. doi:10.1002/dmrr.3752 .
doi: 10.1002/dmrr.3752 |
| [27] |
ŠKRHA J, ŠOUPAL J, ŠKRHA J Jr, et al. Glucose variability, HbA1c and microvascular complications[J]. Rev Endocr Metab Disord, 2016, 17(1): 103-110. doi:10.1007/s11154-016-9347-2 .
doi: 10.1007/s11154-016-9347-2 |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||