

The Journal of Practical Medicine ›› 2025, Vol. 41 ›› Issue (17): 2637-2645.doi: 10.3969/j.issn.1006-5725.2025.17.005
• Feature Reports: Myocardial Damage • Previous Articles
Yanru LI1,3,Weidong JIN1,3( ),Hao GUO2,3,Minglei HAN1,3,Zhen LIU1,3,Yonglan HOU1,3
),Hao GUO2,3,Minglei HAN1,3,Zhen LIU1,3,Yonglan HOU1,3
Received:2025-04-08
Online:2025-09-10
Published:2025-09-05
Contact:
Weidong JIN
E-mail:jwdtreasure@163.com
CLC Number:
Yanru LI,Weidong JIN,Hao GUO,Minglei HAN,Zhen LIU,Yonglan HOU. Nomogram model of recurrence after RFCA for patients with atrial fibrillation complicated with heart failure[J]. The Journal of Practical Medicine, 2025, 41(17): 2637-2645.
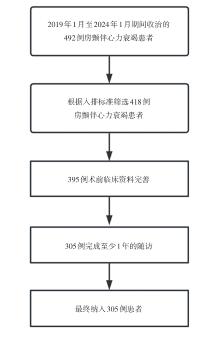
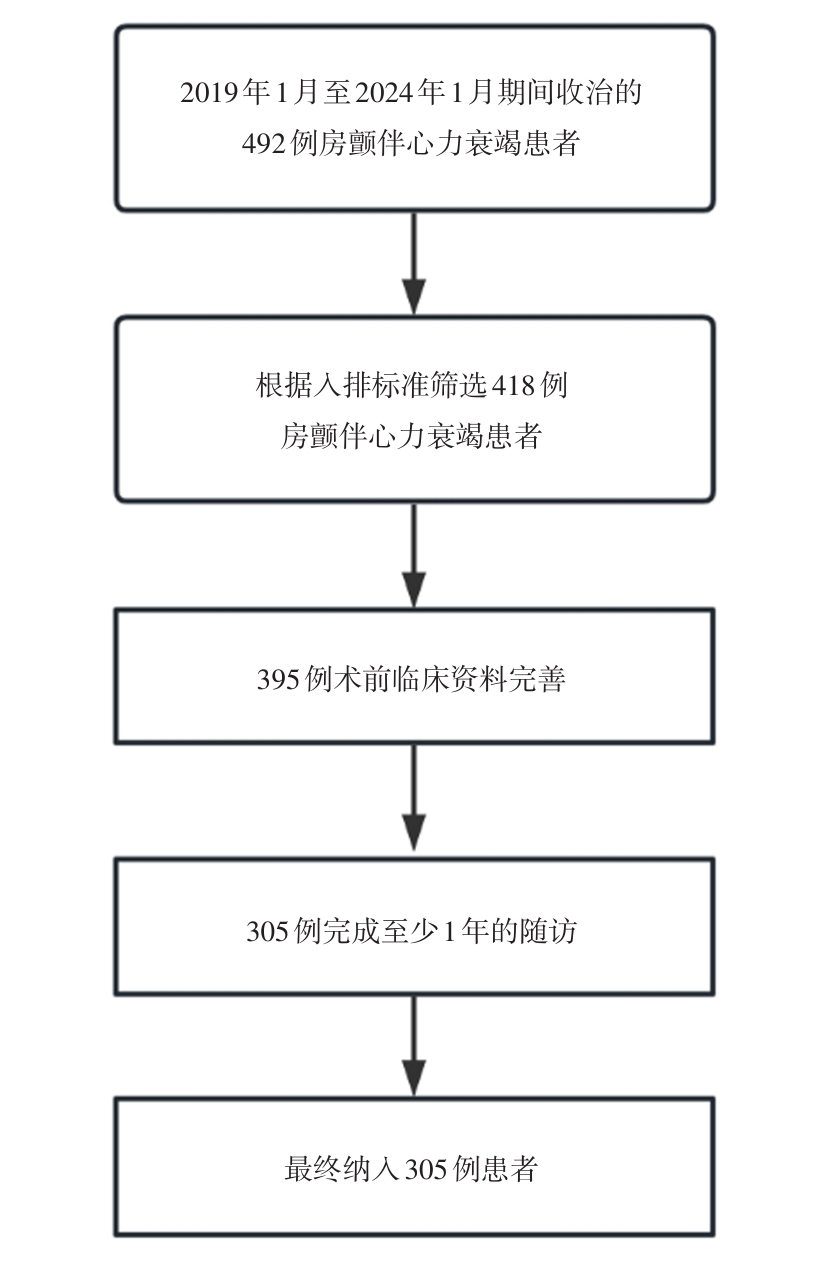
Fig.1
Flow chart of inclusion and exclusion"
Tab.1
Comparison of clinical data of patients between the training set and the validation set"
| 临床资料 | 验证集(n = 92) | 训练集(n = 213) | t/Z/χ2值 | P值 |
|---|---|---|---|---|
| 年龄(x ± s)/岁 | 64.35 ± 9.67 | 63.21 ± 9.73 | 0.94 | 0.349 |
| 性别/[例(%)] | 0.39 | 0.533 | ||
| 男 | 63(68.48) | 138(64.79) | ||
| 女 | 29(31.52) | 75(35.21) | ||
| 入院时NYHA心功能分级/[例(%)] | 0.04 | 0.982 | ||
| Ⅱ级 | 63(68.49) | 144(67.61) | ||
| Ⅲ级 | 23(25.00) | 54(25.35) | ||
| Ⅳ级 | 6(6.51) | 15(7.04) | ||
| 手术时间(x ± s)/min | 141.54 ± 80.23 | 132.41 ± 37.07 | 1.36 | 0.175 |
| BMI(x ± s)/(kg/m2) | 25.47 ± 3.11 | 25.68 ± 3.43 | -0.50 | 0.615 |
| 房颤病程/个月 | 12.00(3.00, 63.00) | 11.00(2.00, 66.00) | -0.90 | 0.370 |
| 房颤类型/[例(%)] | 0.08 | 0.775 | ||
| 持续性 | 27(29.35) | 66(30.99) | ||
| 阵发性 | 65(70.65) | 147(69.01) | ||
| CHA2DS2-VASc评分 | 2.00(1.00, 3.00) | 2.00(1.00, 3.00) | -0.17 | 0.866 |
| 吸烟史/[例(%)] | 26(28.26) | 60(28.17) | 0.01 | 0.987 |
| 饮酒史/[例(%)] | 13(14.13) | 19(8.92) | 1.86 | 0.173 |
| 冠心病/[例(%)] | 50(54.35) | 122(57.28) | 0.22 | 0.636 |
| 高血压/[例(%)] | 48(52.17) | 111(52.11) | 0.01 | 0.992 |
| 糖尿病/[例(%)] | 13(14.13) | 38(17.84) | 0.64 | 0.426 |
| 脑梗死/[例(%)] | 11(11.96) | 24(11.27) | 0.03 | 0.862 |
| 心肌梗死/[例(%)] | 1(1.09) | 3(1.41) | < 0.001 | 1.000 |
| 左心房内径(x ± s)/mm | 37.97 ± 5.42 | 38.19 ± 5.46 | -0.33 | 0.741 |
| 左心室舒张末期内径(x ± s)/mm | 48.35 ± 4.59 | 48.62 ± 4.65 | -0.47 | 0.639 |
| 左心室后壁厚度(x ± s)/mm | 9.11 ± 1.19 | 9.31 ± 1.09 | -1.48 | 0.141 |
| 左室射血分数(x ± s)/分 | 0.62 ± 0.07 | 0.62 ± 0.08 | -0.31 | 0.757 |
| P波时限(x ± s)/ms | 109.49 ± 11.47 | 108.43 ± 12.70 | 0.69 | 0.492 |
| PR间期(x ± s)/ms | 164.53 ± 21.69 | 167.18 ± 23.61 | -0.92 | 0.357 |
| QTc间期(x ± s)/ms | 438.43 ± 27.64 | 438.95 ± 26.26 | -0.16 | 0.876 |
| QRS时限(x ± s)/ms | 96.43 ± 14.83 | 96.29 ± 13.97 | 0.08 | 0.936 |
| NLR | 2.41(1.90, 3.28) | 2.42(1.73, 3.46) | -0.29 | 0.768 |
| C反应蛋白/(mg/L) | 1.10(0.50, 2.70) | 1.20(0.60, 2.75) | -0.46 | 0.647 |
| NT-proBNP/(pg/mL) | 338.19(126.70, 1 051.72) | 335.00(131.00, 942.49) | -0.27 | 0.784 |
| hs-cTn/(ng/mL) | 0.00(0.00, 0.01) | 0.00(0.00, 0.01) | -0.09 | 0.927 |
| D-二聚体/(mg/L) | 0.40(0.21, 0.49) | 0.36(0.19, 0.51) | -0.70 | 0.481 |
| INR | 1.06(0.99, 1.16) | 1.09(1.02, 1.20) | -0.78 | 0.405 |
| 尿素/(mmol/L) | 5.71(4.75, 7.05) | 5.43(4.62, 6.78) | -1.31 | 0.189 |
| 肌酐/(μmol/L) | 72.75(61.27, 86.62) | 71.00(59.50, 81.20) | -1.02 | 0.306 |
| 尿酸/(μmol/L) | 331.20(285.30, 419.30) | 330.60(278.30, 387.80) | -0.91 | 0.365 |
| 总胆固醇(x ± s)/(mmol/L) | 3.94 ± 1.04 | 3.91 ± 0.98 | 0.26 | 0.798 |
| 甘油三酯(x ± s)/(mmol/L) | 1.39 ± 0.87 | 1.37 ± 0.76 | 0.16 | 0.874 |
| 高密度脂蛋白(x ± s)/(mmol/L) | 1.13 ± 0.29 | 1.12 ± 0.28 | 0.30 | 0.763 |
| 低密度脂蛋白/(mmol/L) | 2.15(1.60, 2.77) | 2.11(1.59, 2.59) | -0.75 | 0.451 |
Tab.2
Comparison of clinical data of patients in the training set"
| 临床资料 | 未复发组(n = 152) | 复发组(n = 61) | t/Z/χ2值 | P值 |
|---|---|---|---|---|
| 年龄(x ± s)/岁 | 62.74 ± 9.49 | 64.39 ± 10.31 | -1.12 | 0.262 |
| 性别/[例(%)] | 0.64 | 0.424 | ||
| 男 | 101(66.45) | 37(60.66) | ||
| 女 | 51(33.55) | 24(39.34) | ||
| 入院时NYHA心功能分级/[例(%)] | 0.82 | 0.664 | ||
| Ⅱ级 | 93(66.43) | 51(69.86) | ||
| Ⅲ级 | 38(27.14) | 16(21.92) | ||
| Ⅳ级 | 9(6.43) | 6(8.22) | ||
| 手术时间(x ± s)/min | 129.76 ± 39.39 | 139.03 ± 29.79 | -1.66 | 0.099 |
| BMI(x ± s)/(kg/m2) | 25.68 ± 3.35 | 25.68 ± 3.64 | -0.01 | 0.989 |
| 房颤病程/个月 | 10.00(1.00, 36.00) | 12.00(3.00, 36.00) | -1.01 | 0.314 |
| 房颤类型/[例(%)] | 10.96 | < 0.001 | ||
| 持续性 | 37(24.34) | 29(47.54) | ||
| 阵发性 | 115(75.66) | 32(52.46) | ||
| CHA2DS2-VASc评分/分 | 2.00(1.00, 3.00) | 3.00(3.00, 4.00) | -6.52 | < 0.001 |
| 吸烟史/[例(%)] | 47(30.92) | 13(21.31) | 1.99 | 0.159 |
| 饮酒史/[例(%)] | 11(7.24) | 8(13.11) | 1.85 | 0.174 |
| 冠心病/[例(%)] | 82(53.95) | 40(65.57) | 2.40 | 0.121 |
| 高血压/[例(%)] | 85(55.92) | 26(42.62) | 3.08 | 0.079 |
| 糖尿病/[例(%)] | 26(17.11) | 12(19.67) | 0.20 | 0.658 |
| 脑梗死/[例(%)] | 14(9.21) | 10(16.39) | 2.25 | 0.134 |
| 心肌梗死/[例(%)] | 1(0.66) | 2(3.28) | 0.68 | 0.198 |
| 左心房内径(x ± s)/mm | 37.44 ± 4.61 | 40.07 ± 6.86 | -2.75 | 0.007 |
| 左心室舒张末期内径(x ± s)/mm | 48.88 ± 5.09 | 47.98 ± 3.27 | 1.51 | 0.132 |
| 左心室后壁厚度(x ± s)/mm | 9.28 ± 1.00 | 9.41 ± 1.28 | -0.81 | 0.418 |
| 左室射血分数(x ± s)/分 | 0.62 ± 0.09 | 0.62 ± 0.07 | -0.04 | 0.966 |
| P波时限(x ± s)/ms | 107.73 ± 12.10 | 110.18 ± 14.02 | -1.28 | 0.203 |
| PR间期(x ± s)/ms | 162.71 ± 20.98 | 178.33 ± 26.18 | -4.15 | < 0.001 |
| QTc间期(x ± s)/ms | 438.03 ± 25.18 | 441.26 ± 28.87 | -0.81 | 0.418 |
| QRS时限(x ± s)/ms | 96.17 ± 13.86 | 96.59 ± 14.37 | -0.20 | 0.844 |
| NLR | 2.24(1.66, 3.01) | 3.30(1.96, 5.32) | -3.81 | < 0.001 |
| C反应蛋白/(mg/L) | 1.10(0.50, 2.50) | 1.40(0.80, 3.40) | -1.38 | 0.117 |
| NT-proBNP/(pg/mL) | 263.73(125.00, 688.25) | 589.00(186.00, 1 520.00) | -2.82 | 0.005 |
| hs-cTn/(ng/mL) | 0.00(0.00, 0.01) | 0.00(0.00, 0.01) | -0.19 | 0.829 |
| D-二聚体/(mg/L) | 0.35(0.18, 0.50) | 0.37(0.23, 0.54) | -0.90 | 0.370 |
| INR | 1.08(1.01, 1.20) | 1.11(1.03, 1.18) | -1.20 | 0.228 |
| 尿素/(mmol/L) | 5.33(4.53, 6.57) | 5.98(4.72, 7.28) | -1.74 | 0.081 |
| 肌酐/(μmol/L) | 71.45(59.45, 81.25) | 69.10(59.50, 81.00) | -0.06 | 0.954 |
| 尿酸/(μmol/L) | 339.65(293.57, 388.90) | 319.60(272.00, 362.80) | -1.18 | 0.239 |
| 总胆固醇(x ± s)/(mmol/L) | 3.96 ± 0.98 | 3.78 ± 0.96 | 1.27 | 0.206 |
| 甘油三酯(x ± s)/(mmol/L) | 1.39 ± 0.78 | 1.31 ± 0.71 | 0.69 | 0.491 |
| 高密度脂蛋白(x ± s)/(mmol/L) | 1.11 ± 0.28 | 1.13 ± 0.28 | -0.41 | 0.679 |
| 低密度脂蛋白(mmol/L) | 2.17(1.76, 2.60) | 1.83(1.48, 2.41) | -1.92 | 0.055 |
Tab.3
Univariate and multivariate analyses of recurrence in patients with atrial fibrillation and heart failure at 1 year after RFCA"
| 指标 | 多因素 | ||||
|---|---|---|---|---|---|
| β | S.E | Wald χ2 | P值 | OR(95%CI) | |
| CHA2DS2-VASc 评分 | 0.84 | 0.15 | 31.36 | < 0.001 | 2.32(1.72 ~ 3.13) |
| 左心房内径 | 0.11 | 0.04 | 7.56 | 0.004 | 1.11(1.04 ~ 1.20) |
| PR间期 | 0.03 | 0.01 | 9.00 | < 0.001 | 1.03(1.01 ~ 1.04) |
| NLR | 0.31 | 0.10 | 9.61 | 0.002 | 1.37(1.13 ~ 1.66) |

Fig.2
A nomogram model of recurrence in patients with atrial fibrillation and heart failure at 1 year after RFCA"
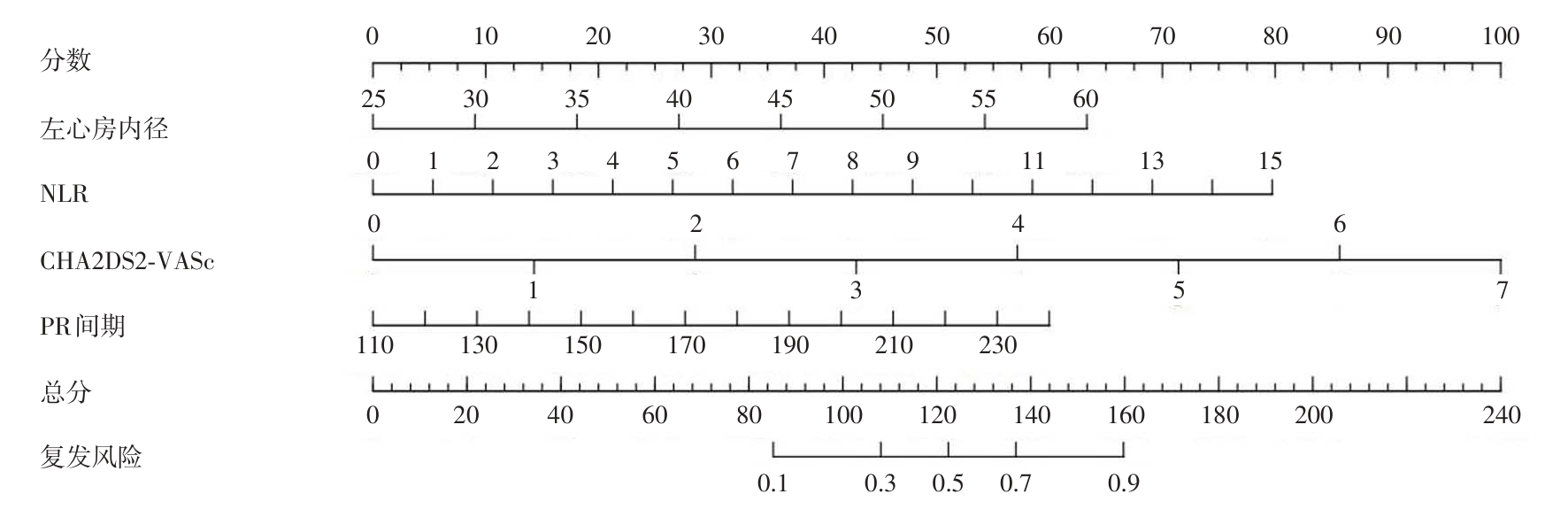
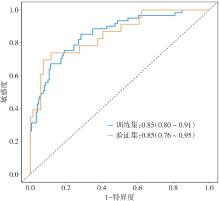
Fig.3
ROC curves of nomogram model for predicting recurrence after treatment"
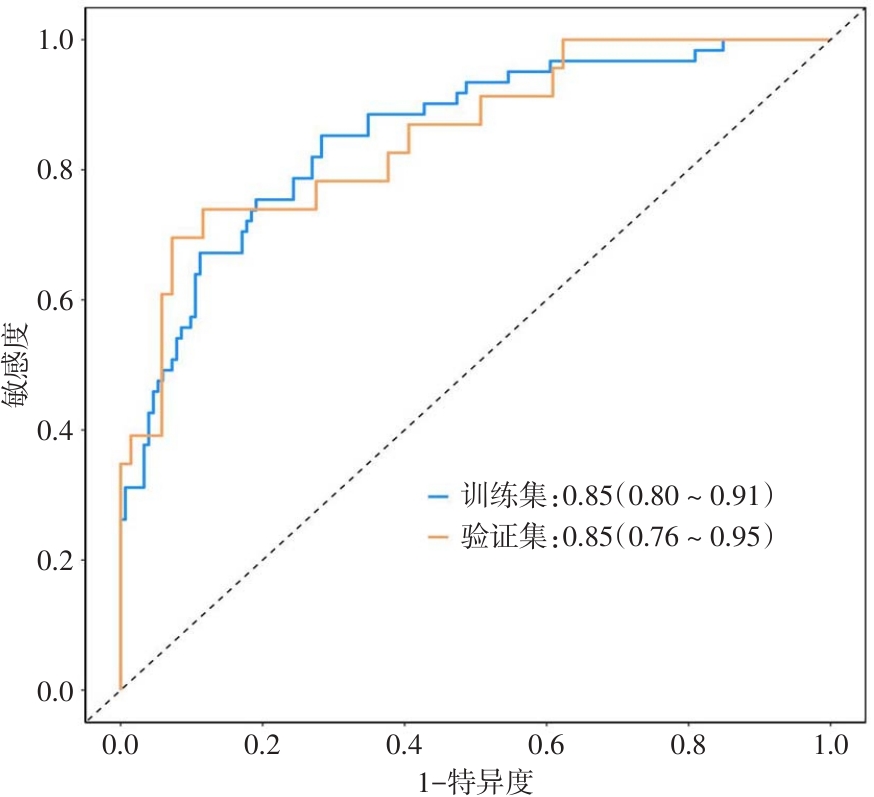
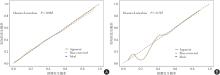
Fig.4
Calibration curves of nomogram model for predicting recurrence after treatment"
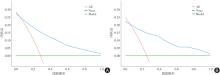
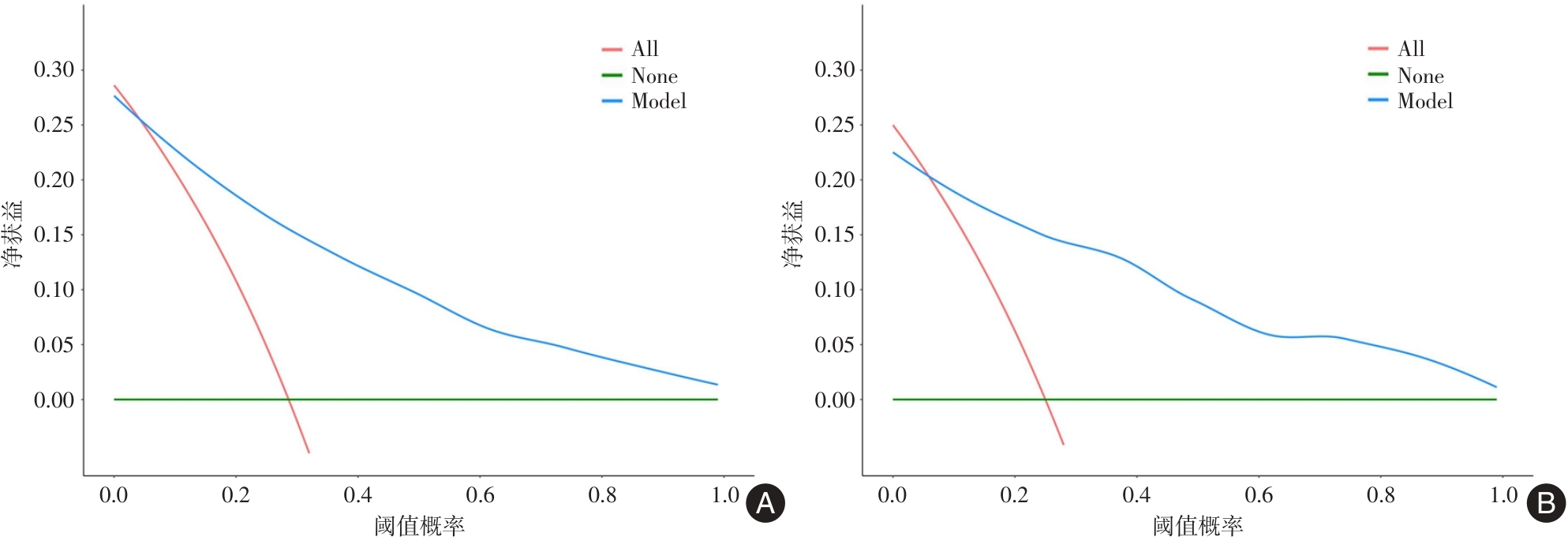
Fig.5
Decision curves of nomogram model for predicting recurrence after treatment"
| [1] | 赵志宏,张邢炜. 中国心房颤动流行病学调查20年[J]. 中国心脏起搏与心电生理杂志,2023,37(3):232-235. |
| [2] | 胡华超,陈娴雅,谢思媛,等. 心房颤动合并心力衰竭患者的临床特点及治疗现状分析的多中心研究[J]. 中国全科医学,2023,26(5):541-549. |
| [3] |
NEWMAN J D, O'MEARA E, BÖHM M, et al. Implications of atrial fibrillation for guideline-directed therapy in patients with heart failure: JACC State-of-the-Art Review [J]. J Am Coll Cardiol, 2024,83(9):932-950. doi:10.1016/j.jacc.2023.12.033
doi: 10.1016/j.jacc.2023.12.033 |
| [4] |
BULHÕES E, ANTUNES V L, MAZETTO R, et al. Catheter ablation versus medical therapy for atrial fibrillation in patients with heart failure with preserved ejection fraction: A systematic review and meta-analysis [J]. Heart Rhythm, 2024,21(9):1595-1603. doi:10.1016/j.hrthm.2024.04.058
doi: 10.1016/j.hrthm.2024.04.058 |
| [5] |
FUJIMOTO H, DOI N, OKAYAMA S, et al. Long-term prognosis of patients undergoing radiofrequency catheter ablation for atrial fibrillation: Comparison between heart failure subtypes based on left ventricular ejection fraction [J]. Europace, 2022,24(4):576-586. doi:10.1093/europace/euab201
doi: 10.1093/europace/euab201 |
| [6] | 念思琦,赵璐露,华宝桐. 心房颤动导管消融术后房性心律失常复发的研究进展[J]. 实用医学杂志,2024,40(10):1338-1343. |
| [7] | 黄义梅,赵璐露,华宝桐. 植入式心电事件监测仪在房颤中的应用及进展[J]. 实用医学杂志,2024,40(21):3095-3100. |
| [8] | 中国医师协会心律学专业委员会心房颤动防治专家工作委,中华医学会心电生理和起搏分会. 心房颤动:目前的认识和治疗建议-2015[J]. 中华心律失常学杂志,2015,19(5):321-384. |
| [9] | 中华医学会心血管病学分会,中国医师协会心血管内科医师分会,中国医师协会心力衰竭专业委员会,等. 中国心力衰竭诊断和治疗指南2024[J]. 中华心血管病杂志,2024,52(3):235-275. |
| [10] | 贾秋蕾,杨亦含,胡元会,等. 阵发性心房颤动进展为持续性心房颤动的危险因素分析[J]. 中国循证心血管医学杂志,2024,16(7):834-836,849. |
| [11] | 张坤,孙光瑶,白金龙,等. 使用二代冷冻球囊消融右下肺静脉难易程度的影响因素[J]. 中国介入心脏病学杂志,2024,32(3):141-146. |
| [12] |
SOHNS C, FOX H, MARROUCHE N F, et al. Catheter ablation in end-stage heart failure with atrial fibrillation [J]. N Engl J Med, 2023,389(15):1380-1389. doi:10.1056/nejmoa2306037
doi: 10.1056/nejmoa2306037 |
| [13] |
BOYALLA V, HARLING L, SNELL A, et al. Biomarkers as predictors of recurrence of atrial fibrillation post ablation: An updated and expanded systematic review and meta-analysis [J]. Clin Res Cardiol, 2022,111(6):680-691. doi:10.1007/s00392-021-01978-w
doi: 10.1007/s00392-021-01978-w |
| [14] | 张宇航,王婧. 超声心动图预测经射频消融治疗后心房颤动复发研究进展[J]. 中国介入影像与治疗学,2024,21(10):628-631. |
| [15] | 熊玉玲,王志燕,华畅,等. 心力衰竭合并持续性心房颤动患者导管射频消融的回顾性研究[J]. 中国介入心脏病学杂志,2024,32(12):683-688. |
| [16] | 吴治胜,史琪,武洋,等. 实时三维超声心动图评价心房颤动患者射频消融术前后左心房功能及二尖瓣构型的变化[J]. 中国医学影像学杂志,2021,29(2):142-147. |
| [17] |
KRANERT M, SHCHETYNSKA MARINOVA T, LIEBE V, et al. Recurrence of atrial fibrillation in dependence of left atrial volume index [J]. In Vivo, 2020,34(2):889-896. doi:10.21873/invivo.11854
doi: 10.21873/invivo.11854 |
| [18] | TAYLAN G, GÖK M, KURTUL A, et al. Integrating the left atrium diameter to improve the predictive ability of the age, creatinine, and ejection fraction score for atrial fibrillation recurrence after cryoballoon ablation [J]. Anatol J Cardiol, 2023,27(10):567-572. |
| [19] | 刘晓宇,郑杰,李库林,等. 左心房大小对磁导航指导下心房颤动射频消融的影响[J]. 中华心律失常学杂志,2019,23(1):57-62. |
| [20] | 黄璇,潘璐,纳丽莎,等. 左心房应变联合心电P波参数预测肺静脉隔离后阵发性心房颤动复发[J]. 中国介入影像与治疗学,2024,21(7):385-389. |
| [21] |
YARMOHAMMADI H, WAN E Y, BIVIANO A, et al. Prolonged PR interval and incidence of atrial fibrillation, heart failure admissions, and mortality in patients with implanted cardiac devices: A real-world survey [J]. Heart Rhythm O2, 2022,4(3):171-179. doi:10.1016/j.hroo.2022.12.009
doi: 10.1016/j.hroo.2022.12.009 |
| [22] |
MARINELLI A, TRACHANAS K, CORSO M, et al. Epicardial adipose tissue, pulmonary veins anatomy, and the P-wave/PR interval ratio in young patients with atrial fibrillation [J]. Heart Rhythm O2, 2023,4(11):692-699. doi:10.1016/j.hroo.2023.09.010
doi: 10.1016/j.hroo.2023.09.010 |
| [23] | 蔡玲,成瑶,张磊. 24小时动态心电图对预激综合征伴心房颤动患者射频消融术后心房颤动复发的预测价值[J]. 中国医药,2024,19(10):1446-1450. |
| [24] |
NISKALA A, HEIJMAN J, DOBREV D, et al. Targeting the NLRP3 inflammasome signalling for the management of atrial fibrillation [J]. Br J Pharmacol, 2024,181(24):4939-4957. doi:10.1111/bph.16470
doi: 10.1111/bph.16470 |
| [25] |
SIDDIQI T J, USMAN M S, SHAHID I, et al. Utility of the CHA2DS2-VASc score for predicting ischaemic stroke in patients with or without atrial fibrillation: A systematic review and meta-analysis [J]. Eur J Prev Cardiol, 2022,29(4):625-631. doi:10.1093/eurjpc/zwab018
doi: 10.1093/eurjpc/zwab018 |
| [26] | 王彦涵,张莱,王君,等. 心房颤动伴中度及以上心房功能性二尖瓣反流患者的临床特征[J]. 南京医科大学学报(自然科学版),2024,44(11):1558-1564. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||