

The Journal of Practical Medicine ›› 2025, Vol. 41 ›› Issue (14): 2143-2151.doi: 10.3969/j.issn.1006-5725.2025.14.004
• Feature Reports:Breast carcinoma • Previous Articles Next Articles
Hai QIU,Yifei GUI( ),Yuan. LIU
),Yuan. LIU
Received:2025-04-09
Online:2025-07-25
Published:2025-07-29
Contact:
Yifei GUI
E-mail:guiyifei@hotmail.com
CLC Number:
Hai QIU,Yifei GUI,Yuan. LIU. Predictors of sentinel lymph node metastasis in clinical T1⁃2 N0 breast cancer patients with preoperatively normal axillary ultrasound[J]. The Journal of Practical Medicine, 2025, 41(14): 2143-2151.
Tab.1
Baseline characteristics"
| 临床病理特征 | 合计(n = 427) |
|---|---|
| 肿瘤最大径 | |
| ≤ 2 cm | 209(48.9) |
| > 2 cm | 218(51.1) |
| 肿瘤位置 | |
| 外上象限 | 173(40.5) |
| 外下象限 | 50(11.7) |
| 内下象限 | 35(8.2) |
| 内上象限 | 104(24.4) |
| 其他 | 65(15.2) |
| 组织学类型 | |
| 导管癌 | 356(83.4) |
| 小叶癌 | 24(5.6) |
| 其他 | 47(11.0) |
| 组织学分级 | |
| Ⅰ | 49(11.5) |
| Ⅱ | 249(58.3) |
| Ⅲ | 78(18.3) |
| 不明确 | 51(11.9) |
| 脉管癌栓 | 100(23.4) |
| 神经侵犯 | 119(27.9) |
| ER阳性 | 356(83.4) |
| PR阳性 | 335(78.5) |
| Her-2阳性 | 78(18.3) |
| Ki-67 | |
| ≤ 14% | 120(28.1) |
| > 14% | 307(71.9) |
| SLN阳性 | 78(18.3) |
| SLN转移数目 | |
| 0枚 | 274(64.2) |
| 1 ~ 2枚 | 69(16.1) |
| ≥ 3枚 | 9(2.1) |
| 未行SLNB | 75(17.6) |
| SLN转移情况 | |
| 无转移或ITC | 274(64.2) |
| 微转移 | 3(0.7) |
| 宏转移 | 75(17.6) |
| 腋窝超声阳性 | 47(11.0) |
| ALN最长径 | |
| > 2.0 cm | 13(3.0) |
| > 1.0 cm且≤ 2.0 cm | 29(6.8) |
| ≤ 1.0 cm | 5(1.2) |
| 阴性 | 380(89.0) |
| ALN最短径 | |
| > 0.5 cm | 36(8.4) |
| ≤ 0.5 cm | 11(2.6) |
| 阴性 | 380(89.0) |
| 超声ALN数目 | |
| 多发 | 27(6.3) |
| 单发 | 20(4.7) |
| 阴性 | 380(89.0) |
Tab.2
Univariate analysis of SLN metastasis"
| 项目 | SLN(-)(n = 274) | SLN(+)(n = 78) | χ2 值 | P值 |
|---|---|---|---|---|
| 年龄 | 1.513 | 0.219 | ||
| ≤ 50岁 | 134(48.9) | 32(41.0) | ||
| > 50岁 | 140(51.1) | 46(59.0) | ||
| 月经状态 | 0.256 | 0.613 | ||
| 绝经前 | 129(47.1) | 36(46.2) | ||
| 绝经后 | 145(52.9) | 42(53.8) | ||
| 肿瘤最大径 | 14.407 | < 0.001 | ||
| ≤ 2 cm | 158(57.7) | 26(33.3) | ||
| > 2 cm | 116(42.3) | 52(66.7) | ||
| 肿瘤位置 | 11.345 | 0.023 | ||
| 外上象限 | 98(35.8) | 40(51.3) | ||
| 外下象限 | 32(11.7) | 9(11.5) | ||
| 内下象限 | 28(10.2) | 3(3.9) | ||
| 内上象限 | 69(25.2) | 21(26.9) | ||
| 其他 | 47(17.2) | 5(6.4) | ||
| 组织学类型 | 4.858 | 0.088 | ||
| 导管癌 | 218(79.6) | 70(89.8) | ||
| 小叶癌 | 18(6.6) | 4(5.1) | ||
| 其他 | 38(13.9) | 4(5.1) | ||
| 组织学分级 | 6.289 | 0.098 | ||
| Ⅰ | 35(12.8) | 8(10.3) | ||
| Ⅱ | 148(54.0) | 54(69.2) | ||
| Ⅲ | 49(17.9) | 10(12.8) | ||
| 不明确 | 42(15.3) | 6(7.7) | ||
| 脉管癌栓 | 26(9.5) | 36(46.2) | 56.247 | < 0.001 |
| 神经侵犯 | 50(18.2) | 44(56.4) | 45.176 | < 0.001 |
| ER阳性 | 221(80.7) | 71(91.0) | 4.616 | 0.032 |
| PR阳性 | 220(80.3) | 62(79.5) | 0.025 | 0.875 |
| Her-2阳性 | 49(17.9) | 14(17.9) | 0.000 | 0.989 |
| Ki-67 | 0.808 | 0.369 | ||
| ≤ 14% | 81(29.6) | 19(24.4) | ||
| > 14% | 193(70.4) | 59(75.6) | ||
| 乳腺手术方式 | 1.160 | 0.281 | ||
| 保乳 | 117(42.7) | 28(35.9) | ||
| 全切 | 157(57.3) | 50(64.1) | ||
| 腋窝超声阳性 | 20(7.3) | 4(5.1) | 0.450 | 0.502 |
Tab.3
Correlation analysis of ALN clinical characteristics with metastatic SLN number and pN-stage classification"
| 临床特征 | SLN转移(n = 352) | χ2值 | P值 | pN分期(n = 427) | χ2值 | P值 | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 0枚(n = 274) | 1~2枚(n = 69) | ≥ 3枚(n = 9) | N0(n = 326) | N1(n = 81) | N2(n = 15) | N3(n = 5) | |||||
| 腋窝超声 | 1.074 | 0.584 Δ | 9.181 | 0.027 Δ | |||||||
| 阳性 | 20(5.7) | 3(0.8) | 1(0.3) | 31(7.3) | 12(2.8) | 1(0.2) | 3(0.7) | ||||
| 阴性 | 254(72.2) | 66(18.7) | 8(2.3) | 295(69.1) | 69(16.1) | 14(3.3) | 2(0.5) | ||||
| 超声ALN最长径 | 1.839 | 0.765 Δ | 9.779 | 0.134 Δ | |||||||
| > 1.0 cm | 18(5.1) | 3(0.8) | 1(0.3) | 29(6.8) | 11(2.6) | 1(0.2) | 3(0.7) | ||||
| ≤ 1.0 cm | 2(0.6) | 0(0.0) | 0(0.0) | 2(0.5) | 1(0.2) | 0(0.0) | 0(0.0) | ||||
| 阴性 | 254(72.2) | 66(18.7) | 8(2.3) | 295(69.1) | 69(16.1) | 14(3.3) | 2(0.5) | ||||
| 超声ALN最短径 | 4.231 | 0.376 Δ | 20.185 | 0.003 Δ | |||||||
| > 0.5 cm | 16(4.5) | 1(0.3) | 1(0.3) | 27(6.3) | 5(1.2) | 1(0.2) | 3(0.7) | ||||
| ≤ 0.5 cm | 4(1.1) | 2(0.6) | 0(0.0) | 4(0.9) | 7(1.6) | 0(0.0) | 0(0.0) | ||||
| 阴性 | 254(72.2) | 66(18.7) | 8(2.3) | 295(69.1) | 69(16.1) | 14(3.3) | 2(0.5) | ||||
| 超声ALN数目 | 5.909 | 0.206 Δ | 14.824 | 0.022 Δ | |||||||
| 多发 | 8(2.3) | 0(0.0) | 1(0.3) | 18(4.2) | 5(1.2) | 1(0.2) | 3(0.7) | ||||
| 单发 | 12(3.4) | 3(0.8) | 0(0.0) | 13(3.1) | 7(1.6) | 0(0.0) | 0(0.0) | ||||
| 阴性 | 254(72.2) | 66(18.7) | 8(2.3) | 295(69.1) | 69(16.1) | 14(3.3) | 2(0.5) | ||||
Tab.4
Correlation analysis of ALN clinical characteristics with metastatic burden and pN-stage in patients with 1-2 metastatic SLN"
| 临床特征 | ALN转移(n = 55) | χ2 值 | P值 | pN分期变化 | χ2 值 | P值 | |||
|---|---|---|---|---|---|---|---|---|---|
0枚 (n = 40) | 1~2枚 (n = 9) | 3~7/8枚 (n = 6) | 无 (n = 63) | 有 (n = 6) | |||||
| 腋窝超声 | 1.552 | 0.460 Δ | 1.000? | ||||||
| 阳性 | 1(1.8) | 1(1.8) | 0(0.0) | 3(4.3) | 0(0.0) | ||||
| 阴性 | 39(70.9) | 8(14.6) | 6(10.9) | 60(87.0) | 6(8.7) | ||||
| 超声ALN最长径 | 1.552 | 0.460 Δ | 1.000? | ||||||
| > 1.0 cm | 1(1.8) | 1(1.8) | 0(0.0) | 3(4.3) | 0(0.0) | ||||
| 阴性 | 39(70.9) | 8(14.6) | 6(10.9) | 60(87.0) | 6(8.7) | ||||
| 超声ALN最短径 | 1.552 | 0.460 Δ | 0.559 | 0.756 Δ | |||||
| > 0.5 cm | 0(0.0) | 0(0.0) | 0(0.0) | 1(1.4) | 0(0.0) | ||||
| ≤ 0.5 cm | 1(1.8) | 1(1.8) | 0(0.0) | 2(2.9) | 0(0.0) | ||||
| 阴性 | 39(70.9) | 8(14.6) | 6(10.9) | 60(87.0) | 6(8.7) | ||||
| 超声ALN数目 | 1.552 | 0.460 Δ | 1.000* | ||||||
| 单发 | 1(1.8) | 1(1.8) | 0(0.0) | 3(4.3) | 0(0.0) | ||||
| 阴性 | 39(70.9) | 8(14.6) | 6(10.9) | 60(87.0) | 6(8.7) | ||||
Tab.5
Multivariate logistic regression analysis of SLN metastasis"
| 影响因素 | β | SE | P值 | Wald | OR | 95%CI |
|---|---|---|---|---|---|---|
| 肿瘤位于外上象限 | 1.415 | 0.569 | 0.013 | 6.178 | 4.118 | 1.349 ~ 12.571 |
| 肿瘤最大径> 2 cm | 0.809 | 0.298 | 0.007 | 7.363 | 2.246 | 1.252 ~ 4.029 |
| 脉管癌栓 | 1.499 | 0.361 | < 0.001 | 17.259 | 4.477 | 2.207 ~ 9.081 |
| 神经侵犯 | 1.103 | 0.332 | 0.001 | 11.061 | 3.013 | 1.573 ~ 5.771 |
Tab.6
Analysis of correlation between independent risk"
| 临床病理特征 | 1~2枚SLN转移(n = 69) | ≥ 3枚SLN转移(n = 9) | P值 |
|---|---|---|---|
| 肿瘤最大径 | 1.000? | ||
| ≤ 2 cm | 23(33.3) | 3(33.3) | |
| > 2 cm | 46(66.7) | 6(66.7) | |
| 肿瘤位置 | 0.482? | ||
| 外上象限 | 34(49.3) | 6(66.7) | |
| 其他 | 35(50.7) | 3(33.3) | |
| 脉管癌栓 | 0.001? | ||
| 有 | 27(39.1) | 9(100.0) | |
| 无 | 42(60.9) | 0(0.0) | |
| 神经侵犯 | 0.004? | ||
| 有 | 35(50.7) | 9 (100.0) | |
| 无 | 34(49.3) | 0(0.0) |
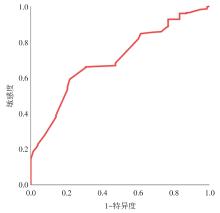
Fig.1
ROC curve of predictive nomogram for SLN metastasis"
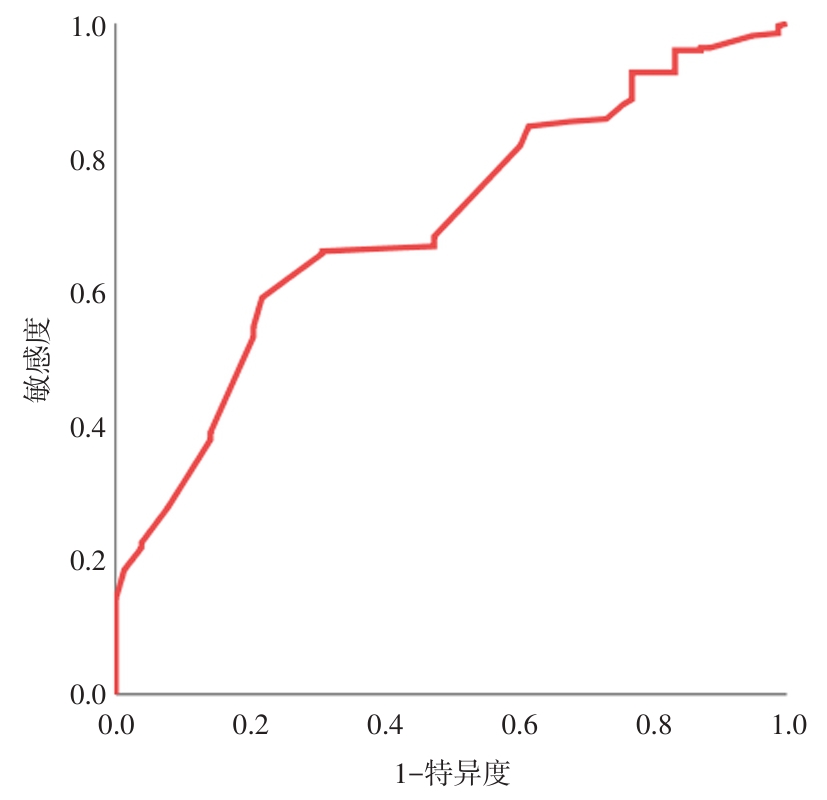
Tab.7
Predictive analysis of the correlation between predictive models and independent risk factors in SLN metastasis"
| 因素 | AUC(95%CI) | P值 | 敏感度/% | 特异度/% |
|---|---|---|---|---|
| 预测模型 | 0.702(0.651 ~ 0.749) | < 0.0001 | 78.21 | 59.12 |
| 肿瘤位于外上象限 | 0.592(0.539 ~ 0.644) | 0.007 | 51.28 | 64.23 |
| 肿瘤最大径> 2 cm | 0.622(0.569 ~ 0.673) | 0.0001 | 66.67 | 57.66 |
| 脉管癌栓 | 0.683(0.632 ~ 0.732) | < 0.0001 | 46.15 | 90.51 |
| 神经侵犯 | 0.691(0.640 ~ 0.739) | < 0.0001 | 56.41 | 81.75 |
| [1] |
MATTAR A, ANTONINI M, CAVALCANTE F P, et al. CADONOT: Comparing axillary dissection or not in breast cancer surgery [J]. Breast, 2025, 81: 104453. doi:10.1016/j.breast.2025.104453
doi: 10.1016/j.breast.2025.104453 |
| [2] |
HASSAN A M, HAJJ J P, LEWIS J P, et al. Long-Term Outcomes of Lymphedema After Immediate Lymphatic Reconstruction Following Axillary Lymph Node Dissection [J]. Ann Surg Oncol, 2025.doi: 10.1245/s10434-025-17301-0 . Online ahead of print.
doi: 10.1245/s10434-025-17301-0 |
| [3] |
LI Q, XU H, BAO B, et al. Predicting sentinel lymph node metastasis in breast cancer: A study based on the SEER database [J]. Clin Exp Med, 2025, 25(1): 82. doi:10.1007/s10238-025-01591-5
doi: 10.1007/s10238-025-01591-5 |
| [4] | 李文肖, 刘燕, 曹春莉, 等. 常规超声联合超声造影预测乳腺癌腋窝淋巴结转移的价值 [J]. 实用医学杂志, 2022, 38(18): 2272-2278. |
| [5] |
COMBI F, ANDREOTTI A, GAMBINI A, et al. Application of OSNA Nomogram in Patients With Macrometastatic Sentinel Lymph Node: A Retrospective Assessment of Accuracy [J]. Breast Cancer (Auckl), 2021, 15: 11782234211014796. doi:10.1177/11782234211014796
doi: 10.1177/11782234211014796 |
| [6] | GALIMBERTI V, COLE B F, VIALE G, et al. Axillary dissection versus no axillary dissection in patients with breast cancer and sentinel-node micrometastases (IBCSG 23-01): 10-year follow-up of a randomised, controlled phase 3 trial [J].Lancet Oncol, 2018, 19(10): 1385-1393. |
| [7] |
GIULIANO A E, BALLMAN K V, MCCALL L, et al. Effect of Axillary Dissection vs No Axillary Dissection on 10-Year Overall Survival Among Women With Invasive Breast Cancer and Sentinel Node Metastasis: The ACOSOG Z0011 (Alliance) Randomized Clinical Trial [J]. JAMA, 2017, 318(10): 918-926. doi:10.1001/jama.2017.11470
doi: 10.1001/jama.2017.11470 |
| [8] |
FU F, ZHANG Y, SUN J, et al. Predictors of sentinel lymph node metastasis in Chinese women with clinical T1-T2 N0 breast cancer and a normal axillary ultrasound [J]. Acta Radiol, 2022, 63(11): 1463-1468. doi:10.1177/02841851211054191
doi: 10.1177/02841851211054191 |
| [9] |
暴珞宁, 王瑛, 陈东, 等. 超声影像组学标签预测乳腺癌前哨淋巴结转移的价值 [J]. 实用医学杂志, 2021, 37(15): 2007-2011. doi:10.3969/j.issn.1006-5725.2021.15.020
doi: 10.3969/j.issn.1006-5725.2021.15.020 |
| [10] | GENTILINI O D, BOTTERI E, SANGALLI C, et al. Sentinel Lymph Node Biopsy vs No Axillary Surgery in Patients With Small Breast Cancer and Negative Results on Ultrasonography of Axillary Lymph Nodes: The SOUND Randomized Clinical Trial [J]. JAMA Oncol, 2023, 9(11): 1557-1564. |
| [11] |
WINTRAECKEN V M, BOERSMA L J, VAN ROOZENDAAL L M, et al. Quality assurance of radiation therapy after breast-conserving surgery among patients in the BOOG 2013-08 trial [J]. Radiother Oncol, 2024, 191: 110069. doi:10.1016/j.radonc.2023.110069
doi: 10.1016/j.radonc.2023.110069 |
| [12] | 丛斌斌, 曹晓珊, 王春建, 等. 临床查体阴性但超声检查及穿刺确诊腋窝淋巴结转移的乳腺癌前哨淋巴结活检的可行性分析 [J]. 中国癌症杂志, 2023, 33(6): 574-580. |
| [13] |
DING W, CHEN Y, LIN Y, et al. The impact of axillary lymph node dissection on the prognosis of breast cancer patients undergoing up-front mastectomy with Sentinel lymph node micrometastases [J]. Sci Rep, 2025, 15(1): 10525. doi:10.1038/s41598-025-91405-1
doi: 10.1038/s41598-025-91405-1 |
| [14] | 罗海愉, 朱丽璋, 张屿森, 等. 术前超声与临床T1-2期乳腺癌腋窝淋巴结负荷的相关性分析 [J]. 中国超声医学杂志, 2021, 37(8): 859-861. |
| [15] |
MINAMI S, SAKIMURA C, IRIE J, et al. Predictive Factors Among Clinicopathological Characteristics for Sentinel Lymph Node Metastasis in T1-T2 Breast Cancer [J]. Cancer Manag Res, 2021, 13: 215-223. doi:10.2147/cmar.s284922
doi: 10.2147/cmar.s284922 |
| [16] |
HERMANSYAH D, INDRA W, PARAMITA D A, et al. Role of Hormonal Receptor in Predicting Sentinel Lymph Node Metastasis in Early Breast Cancer [J]. Med Arch, 2022, 76(1): 34-38. doi:10.5455/medarh.2022.76.34-38
doi: 10.5455/medarh.2022.76.34-38 |
| [17] | 甘丽. 不同象限早期浸润性乳腺癌前哨淋巴结转移与其临床病理特征的关系研究 [D]. 郑州:郑州大学, 2024. |
| [18] | 王文彦, 孟祥志, 李霓, 等. 基于SEER数据库回顾性分析T1期乳腺癌腋窝淋巴结转移和预后影响因素 [J]. 中华医学杂志, 2021, 101(27): 2152-2158. |
| [19] |
FU W D, WANG X H, LU K K, et al. Real-world outcomes for Chinese breast cancer patients with tumor location of central and nipple portion [J]. Front Surg, 2022, 9: 993263. doi:10.3389/fsurg.2022.993263
doi: 10.3389/fsurg.2022.993263 |
| [20] |
YANG J, YANG Q, MUKHERJEE A, et al. Distance Between the Tumour and Nipple as a Predictor of Axillary Lymph Node Involvement in Breast Cancer [J]. Cancer Manag Res, 2021, 13: 193-199. doi:10.2147/cmar.s262413
doi: 10.2147/cmar.s262413 |
| [21] |
YIMING A, WUBULIKASIMU M, YUSUYING N. Analysis on factors behind sentinel lymph node metastasis in breast cancer by color ultrasonography, molybdenum target, and pathological detection [J]. World J Surg Oncol, 2022, 20(1): 72. doi:10.1186/s12957-022-02531-3
doi: 10.1186/s12957-022-02531-3 |
| [22] |
LYU W, GUO Y, PENG H, et al. Analysis of the Influencing Factors of Sentinel Lymph Node Metastasis in Breast Cancer [J]. Evid Based Complement Alternat Med, 2022, 2022: 5775971. doi:10.1155/2022/5775971
doi: 10.1155/2022/5775971 |
| [23] |
ZHAO Y, YANG N, WANG X, et al. Potential roles of lymphovascular space invasion based on tumor characteristics provide important prognostic information in T1 tumors with ER and HER2 positive breast cancer [J]. Clin Transl Oncol, 2020, 22(12): 2275-2285. doi:10.1007/s12094-020-02369-9
doi: 10.1007/s12094-020-02369-9 |
| [24] |
WEI C, DENG Y, WEI S, et al. Lymphovascular invasion is a significant risk factor for non-sentinel nodal metastasis in breast cancer patients with sentinel lymph node (SLN)-positive breast cancer: a cross-sectional study [J]. World J Surg Oncol, 2023, 21(1): 386. doi:10.1186/s12957-023-03273-6
doi: 10.1186/s12957-023-03273-6 |
| [25] | 李卓璇, 童一苇, 陈小松, 等. 腋窝临床淋巴结阳性超声特征与乳腺癌淋巴结转移负荷及预后的相关性研究 [J]. 中国癌症防治杂志, 2022, 14(4): 393-399. |
| [1] | Jingshuo LI,Shoushi LIU,Hongwei. GUO. Advances in the mechanism and therapeutic potential of Erianin⁃induced apoptosis in breast cancer cells [J]. The Journal of Practical Medicine, 2025, 41(14): 2132-2137. |
| [2] | Yuling DUAN,Xuezhi ZHOU,Yongyi LI,Lixia MA,Desheng YANG,Jiao CHENG,Yan WU,Tao LIU,Guoyuan JIANG,Mei. WANG. Clinical value analysis of different MRI measurement methods in evaluating the efficacy of neoadjuvant therapy for breast cancer [J]. The Journal of Practical Medicine, 2025, 41(14): 2152-2159. |
| [3] | Lu JIANG,Weipeng LYU,Sijing CHEN,Yanhua FANG,Shanshan LIANG. Inhibitory effect of disitamab vedotin on breast cancer cells with different HER⁃2 expression levels in tumor organoid culture system [J]. The Journal of Practical Medicine, 2025, 41(12): 1808-1815. |
| [4] | Yaqian DENG,Wenxiao LI,Zelin XU,Jinmei MA,Tingting DU,Wen LIU,Jun LI. Predictive value of growth orientation quantification combined with S⁃Detect technique for axillary lymph node metastasis in breast cancer [J]. The Journal of Practical Medicine, 2025, 41(1): 100-107. |
| [5] | Zixu SONG,Guangzheng ZHU,Chenxu GUO,Jiaqi WU,Ligong ZHANG,Jun. QIAN. Expression of SLC35A2 and PFDN2 in breast cancer and its relationship with clinical observables and prognosis [J]. The Journal of Practical Medicine, 2024, 40(4): 496-502. |
| [6] | Fen LIU,Hui ZHAO,Limin. GUO. Relationship between multi⁃omics combined detection and clinicopathological characteristics, neoadjuvant chemotherapy effect of breast cancer [J]. The Journal of Practical Medicine, 2024, 40(24): 3539-3546. |
| [7] | Yinghua ZENG,Wenji LI,Li. ZHENG. The Impact of the timing of initial dressing change following PICC catheterization on postoperative breast cancer patients [J]. The Journal of Practical Medicine, 2024, 40(19): 2772-2777. |
| [8] | Che CHEN,Dehong LUO,Huangfei YU,Qin ZHANG,Xiaochi HU,Shenghua YU,Yajun. LI. Clinical Application of automatic delineation in whole breast radiotherapy with simultaneous integrated boost to the medial tumor beds [J]. The Journal of Practical Medicine, 2024, 40(17): 2406-2411. |
| [9] | Shaojin LI,Shipeng. ZHENG. Relevant preoperative imaging pathological features and tumor markers serve as predictive indicators for the risk of sentinel lymph node metastasis in breast cancer [J]. The Journal of Practical Medicine, 2024, 40(17): 2418-2424. |
| [10] | Lingyu FANG,Jinghua HU,Junfeng WEN,Shiqi HAN,Yali WANG,Lulan PU,Jingjia LI,Yi YANG,Shishan DENG,Lingmi HOU,Fangfang. ZHOU. Expression and significance of ubiquitin⁃specific proteases 20 and hypoxia inducible factor⁃1α in breast cancer [J]. The Journal of Practical Medicine, 2024, 40(16): 2270-2276. |
| [11] |
AI Yongbiao, HUANG Jun, YUAN Jie, LI Wenfang..
Androgen receptor expression in early triple negative breast cancer and its association with the clinicopath⁃ ological features and prognosis [J]. The Journal of Practical Medicine, 2023, 39(8): 975-979. |
| [12] |
TANG Chunfang, ZHANG Maoling, CHEN Miaohong, RUAN Jing, LÜ Qiyuan..
Prevalence and predictors of intimate partner violence among women with infertility [J]. The Journal of Practical Medicine, 2023, 39(8): 1045-1051. |
| [13] | Xiran SHI,Heng WANG,Libing HE,Zhiqiang QIU,Hongjian LI,Xiaoxue. XU. Advance in predicting lymph node metastasis of breast cancer by multimodal MRI [J]. The Journal of Practical Medicine, 2023, 39(22): 2861-2865. |
| [14] | Yadan CHE,Lixia. LI. Reaserch progress on small molecule anti⁃angiogenic drugs for advanced breast cancer [J]. The Journal of Practical Medicine, 2023, 39(22): 2866-2871. |
| [15] | Zhaowei ZHUANG,Wumei YUAN,Zuodong REN,Shangfei LI,Minggui CHEN,Yan. ZENG. Expression and significance of granzyme B and perforin in peripheral blood of patients with breast cancer [J]. The Journal of Practical Medicine, 2023, 39(22): 2872-2877. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||