

The Journal of Practical Medicine ›› 2025, Vol. 41 ›› Issue (5): 683-690.doi: 10.3969/j.issn.1006-5725.2025.05.010
• Clinical Research • Previous Articles
Dongli LIU1,Zilin QUAN2,Lingxiu ZHONG1,Qiqi CHEN1,Wenqiao CAI1,Senpei ZHUANG1,Ying WEI1,Huiyi PAN1,Yawen. LIN1( )
)
Received:2024-12-27
Online:2025-03-10
Published:2025-03-20
Contact:
Yawen. LIN
E-mail:linyawen@gdph.org.cn
CLC Number:
Dongli LIU,Zilin QUAN,Lingxiu ZHONG,Qiqi CHEN,Wenqiao CAI,Senpei ZHUANG,Ying WEI,Huiyi PAN,Yawen. LIN. Construction and validation of a predictive model for antibiotic-associated diarrhea after surgery in children with congenital heart disease[J]. The Journal of Practical Medicine, 2025, 41(5): 683-690.
Tab.1
Univariate analysis of antibiotic-associated diarrhea (AAD) after congenital heart disease surgery in children M(P25,P75)"
| 临床资料 | 例数 | AAD组(n = 164) | 非AAD组(n = 166) | χ2/Z值 | P值 |
|---|---|---|---|---|---|
| 性别/[例(%)] | 0.430 | 0.512 | |||
| 男 | 171 | 96(58.6) | 75(45.2) | ||
| 女 | 159 | 68(41.4) | 91(54.8) | ||
| 心脏疾病诊断个数/[例(%)] | -2.051 | 0.323 | |||
| 1 ~ 2个 | 98 | 43(26.2) | 55(32.9) | ||
| 3 ~个 | 176 | 88(53.7) | 88(53.1) | ||
| ≥ 5个 | 56 | 33(20.1) | 23(13.9) | ||
| ASA分级/[例(%)] | 0.252 | 0.882 | |||
| Ⅰ级 | 160 | 51(31.0) | 109(65.7) | ||
| Ⅱ级 | 153 | 97(59.1) | 56(33.7) | ||
| Ⅲ级 | 17 | 16(9.7) | 1(0.6) | ||
| STRONGkids营养评分/[例(%)] | 0.138 | 0.710 | |||
| 中度 | 319 | 158(96.3) | 161(96.9) | ||
| 重度 | 11 | 6(3.7) | 5(3.0) | ||
| 禁食/[例(%)] | 329 | 163(99.4) | 166(100) | 1.847 | 0.084 |
| 预防使用抗生素/[例(%)] | 320 | 157(95.7) | 163(98.2) | 3.635 | 0.057 |
| 抗生素给药途径/[例(%)] | 1.629 | 0.202 | |||
| 静脉 | 294 | 139(47.2) | 155(52.7) | ||
| 静脉+口服 | 36 | 25(69.4) | 11(30.6) | ||
| 抗生素联合情况/[例(%)] | -6.282 | < 0.001 | |||
| 单联 | 218 | 88(53.6) | 130(78.3) | ||
| 二联 | 60 | 38(23.2) | 22(13.3) | ||
| 三联 | 52 | 38(23.2) | 14(8.4) | ||
| 青霉素类/[例(%)] | 92 | 56(34.5) | 36(21.7) | 10.088 | 0.059 |
| 碳青霉烯类/[例(%)] | 30 | 16(10.0) | 14(8.4) | 0.046 | 0.831 |
| 大环内酯类/[例(%)] | 12 | 8(66.7) | 4(33.3) | 0.888 | 0.054 |
| 头孢类/[例(%)] | 268 | 135(51.9) | 133(48.1) | 0.178 | 0.673 |
| 糖肽类/[例(%)] | 43 | 30(68.9) | 13(31.1) | 0.176 | 0.675 |
| 恶唑烷酮类/[例(%)] | 14 | 11(78.5) | 3(21.4) | 0.002 | 0.966 |
| 机械通气/[例(%)] | 196 | 130(66.3) | 66(33.6) | 73.092 | < 0.001 |
| 使用微生态制剂/[例(%)] | 147 | 36(24.5) | 111(75.5) | 72.313 | < 0.001 |
| 年龄/月 | 6(4,10) | 5(3,12) | -1.692 | 0.091 | |
| 体质量/kg | 6.5(5.5,8.0) | 6.0(4.9,8.0) | -1.394 | 0.163 | |
| 手术时间/min | 177.6(147.0,220.8) | 142.8(118.8,169.8) | -8.610 | < 0.001 | |
| 住院时间/d | 12(9,17) | 8(6,11) | -8.424 | < 0.001 | |
| 抗生素使用时间/d | 10.0(7.0,13.5) | 4.0(3.0,7.0) | -10.995 | < 0.001 | |
| IgG/(g/L) | 5.781(3.315,9.145) | 3.638(2.477,8.568) | -8.842 | 0.745 | |
| 白细胞计数/(× 109/L) | 10.4(7.7,13.0) | 9.9(8.0,12.5) | -1.185 | 0.036 | |
| 血红蛋白/(g/L) | 105(93,116) | 106(93,120) | -0.252 | 0.801 | |
| 血小板计数/(× 109/L) | 216.5(154.3,259.8) | 230.0(175.0,283.0) | -1.941 | 0.052 | |
| 中性粒细胞/(× 109/L) | 5.9(3.7,8.0) | 6.3(4.5,8.3) | -1.596 | 0.111 | |
| 中性粒细胞比值/% | 0.576(0.474,0.693) | 0.616(0.508,0.717) | -2.177 | 0.069 | |
| 肌酐/(μmol/L) | 21.08(16.32,25.87) | 21.80(17.54,26.97) | -1.005 | 0.315 | |
| 白蛋白/(g/L) | 33.61(31.05,36.48) | 33.30(30.58,35.80) | -1.194 | 0.232 | |
| 肌酸激酶同工酶/(U/L) | 26.2(17.0,43.0) | 30.2(19.0,52.4) | -2.092 | 0.056 | |
| 丙氨酸氨基转移酶/(U/L) | 20(14.3,31.8) | 21.0(15.0,28.0) | -0.215 | 0.830 | |
| 天门冬氨酸氨基转移酶/(U/L) | 48(31,90) | 53(32,90) | -1.443 | 0.149 | |
| C反应蛋白/(mg/L) | 26.61(12.68,58.56) | 16.81(6.20,38.75) | -4.81 | 0.002 | |
Tab.2
Variable assignment"
| 变量 | 类型 | 赋值 |
|---|---|---|
| 抗生素使用情况 | 分类变量 | 一联=0,二联=1,三联=2 |
| 机械通气 | 分类变量 | 否=0,是=1 |
| 使用微生态制剂 | 分类变量 | 否=0,是=1 |
| 手术时间 | 连续变量 | 原值录入 |
| 住院时间 | 连续变量 | 原值录入 |
| 抗生素使用时间 | 连续变量 | 原值录入 |
| 白细胞计数 | 连续变量 | 原值录入 |
| C反应蛋白 | 连续变量 | 原值录入 |
Tab.3
Multivariate logistic regression analysis of antibiotic-associated diarrhea (AAD) after congenital heart disease surgery in children"
| 指标 | β | S.E | Wald χ2 | P值 | OR值 | 95%CI |
|---|---|---|---|---|---|---|
| 抗生素联合情况(二联) | 1.292 | 0.420 | 9.467 | 0.002 | 3.639 | 1.598~8.286 |
| 抗生素联合情况(三联) | 1.695 | 0.554 | 9.362 | 0.002 | 5.446 | 1.839~16.126 |
| 机械通气(是) | 1.895 | 0.345 | 30.092 | < 0.001 | 6.654 | 3.381~13.096 |
| 使用微生态制剂(是) | -2.149 | 0.357 | 36.262 | < 0.001 | 0.117 | 0.058~0.235 |
| 手术时间(min) | 0.020 | 0.004 | 25.393 | < 0.001 | 1.020 | 1.012~1.028 |
| 抗生素使用时间(d) | 0.142 | 0.041 | 12.194 | < 0.001 | 1.153 | 1.064~1.249 |
| C反应蛋白(mg/L) | 0.016 | 0.006 | 8.260 | 0.004 | 1.016 | 1.005~1.027 |
| 常量 | -5.629 | 0.820 | 47.090 | < 0.001 | 0.004 | - |

Fig.1
Nomogram for predicting the risk of antibiotic-associated diarrhea (AAD) after congenital heart disease surgery in children"
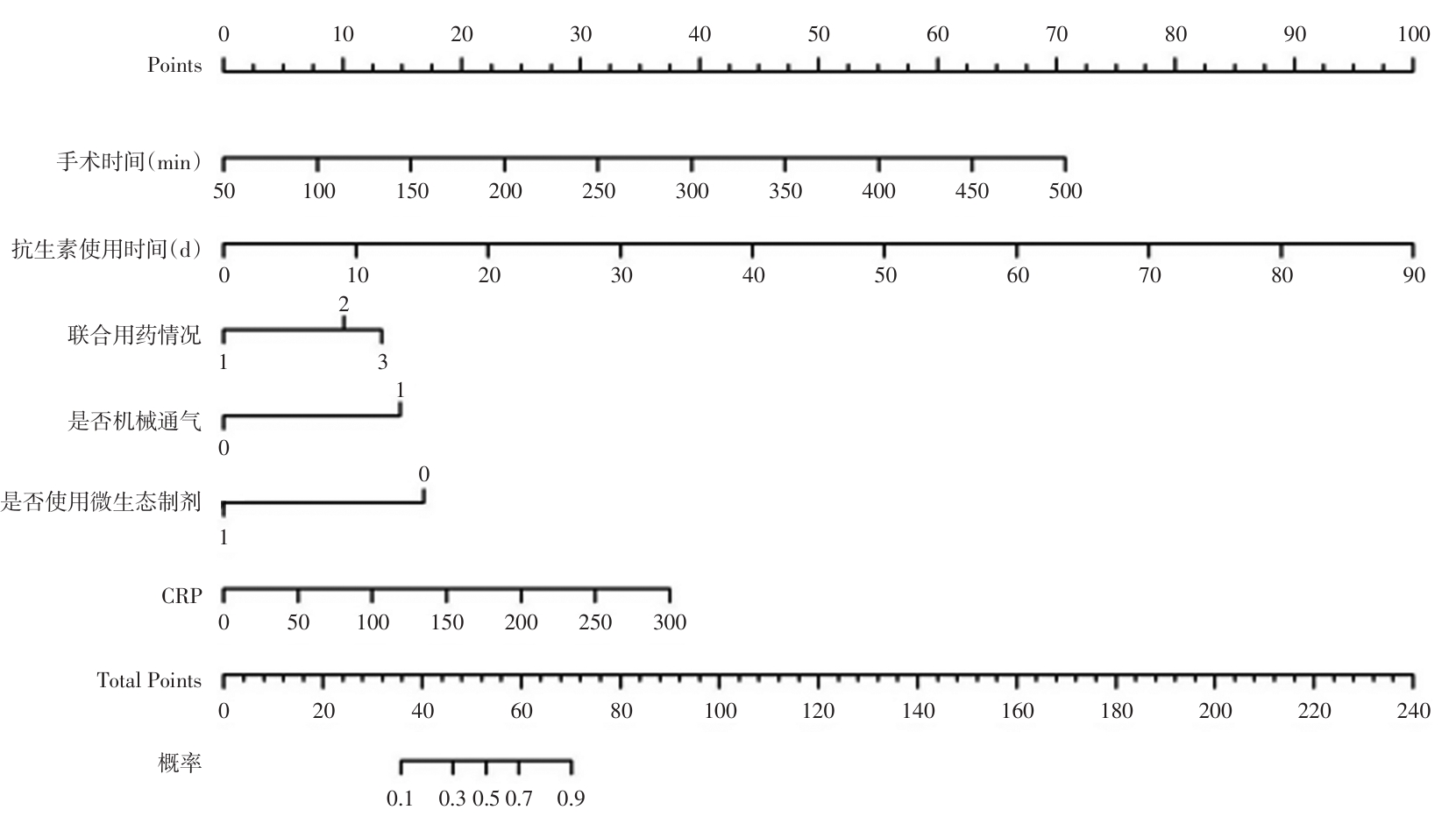
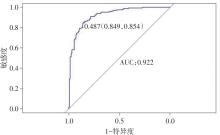
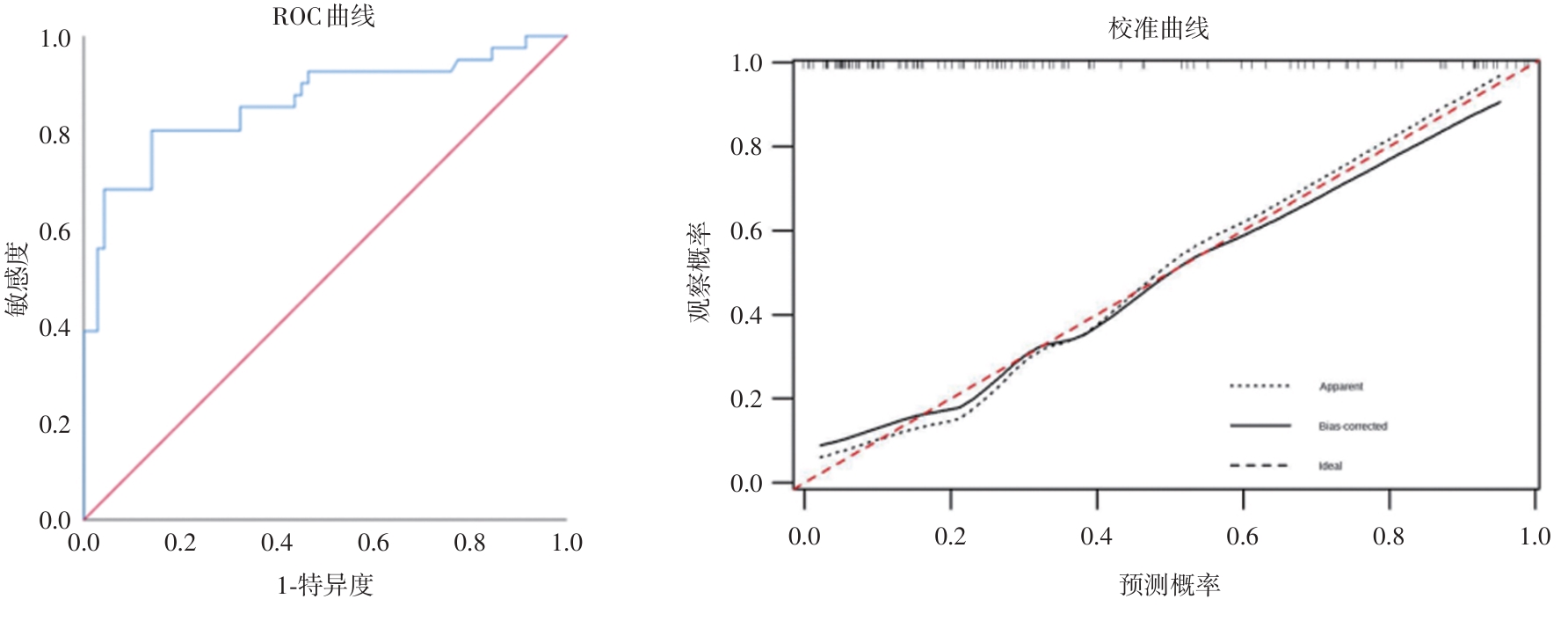
Fig.2
Receiver operating characteristic (ROC) curve of the predictive model for antibiotic-associated diarrhea (AAD) after congenital heart disease surgery in children in the modeling group"
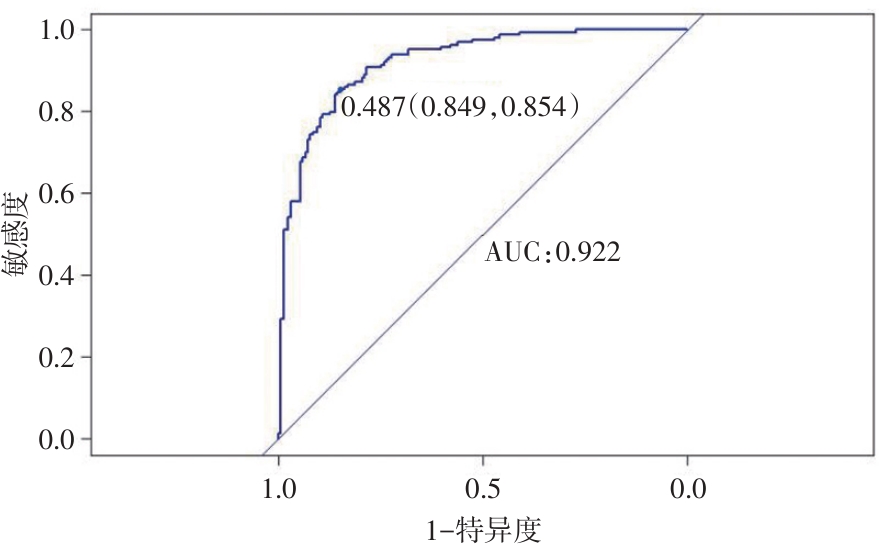
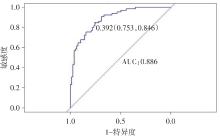
Fig.3
Receiver operating characteristic (ROC) curve of the predictive model for antibiotic-associated diarrhea (AAD) after congenital heart disease surgery in children in the internal validation group"
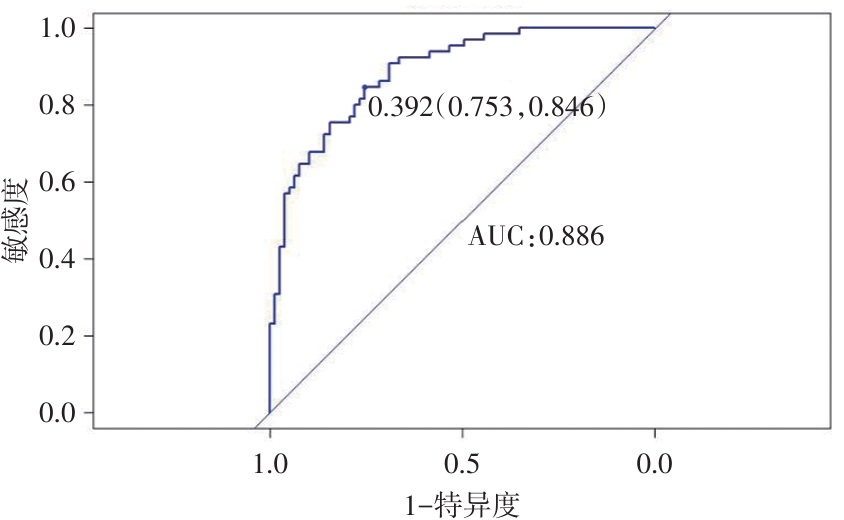
Fig.4
Calibration curve in the modeling group"
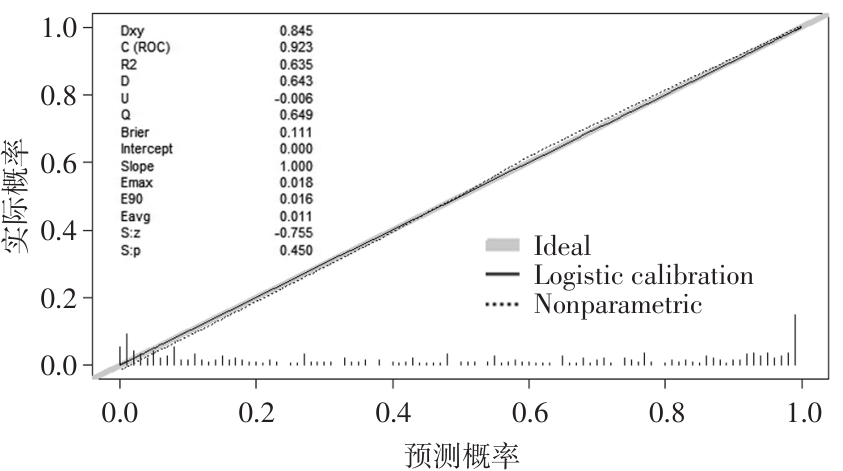
Fig.5
Calibration curve in the internal validation group"
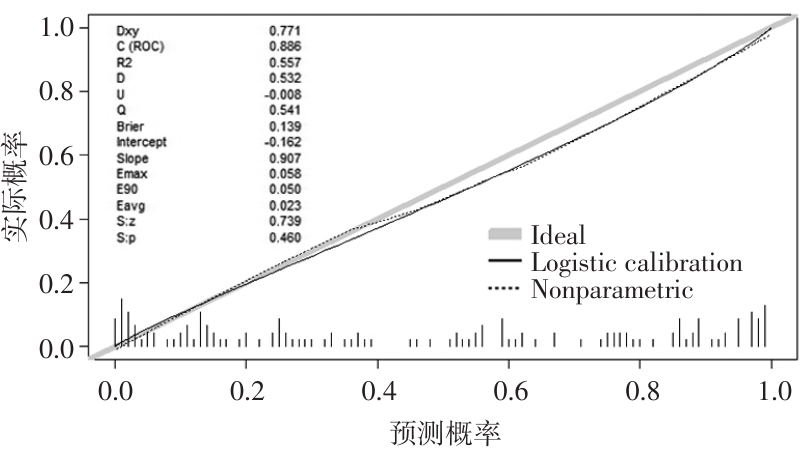
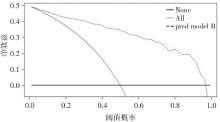
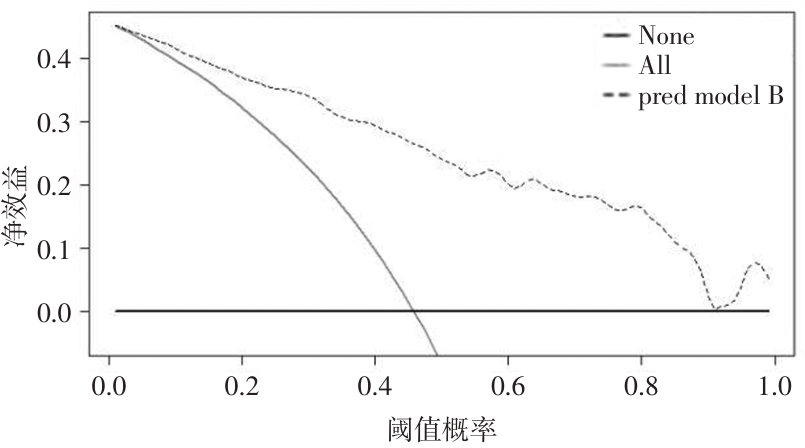
Fig.6
Calibration curve in the modeling group"
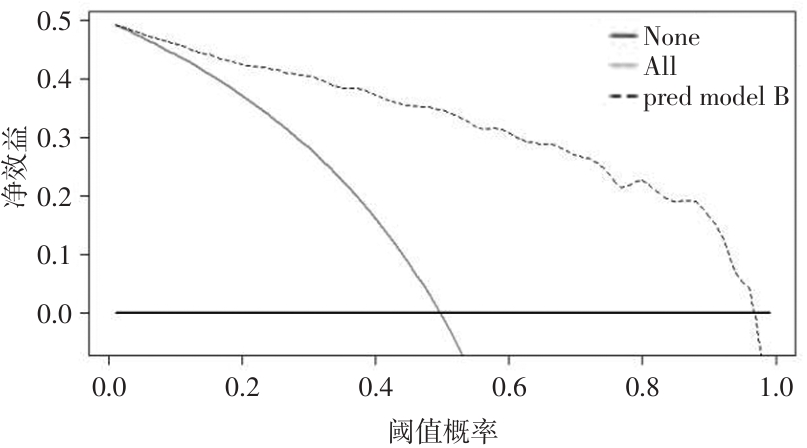
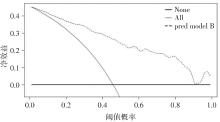
Fig.7
Calibration curve in the internal validation group"
Tab.4
Model-relevant variable data for external patients"
| 相关变量 | 外部验证组(n = 112) | AAD组(n = 41) | 非AAD组(n = 71) | P值 |
|---|---|---|---|---|
| 抗生素联合情况 | ||||
| 二联 | 32(28.6) | 16(39.0) | 16(22.5) | 0.013 |
| 三联 | 24(21.4) | 13(32.0) | 11(15.5) | 0.001 |
| 机械通气 | 76(67.9) | 36(87.8) | 40(56.3) | < 0.001 |
| 使用微生态制剂 | 54(48.2) | 11(26.8) | 43(60.6) | 0.012 |
| 手术时间[M(P25,P75)]/min | 180.7(132.6,217.8) | 199.2(150.3,240.3) | 170.0(127.2,195.0) | 0.376 |
| 抗生素使用时间[M(P25,P75)]/d | 11.6(3,14) | 16(10,21) | 8.21(3,10) | 0.353 |
| C反应蛋白[M(P25,P75)]/(mg/L) | 19.5(4.9,30.6) | 29.8(15.3,39.8) | 13.6(3.9,18.2) | 0.002 |
Fig.8
Receiver operating characteristic(ROC)curve and calibration curve of the predictive model for antibiotic?associated diarrhea(AAD) after congenital heart disease surgery in children in the external validation group"
| 1 | 中国生物医学工程学会体外循环分会,侯晓彤.2023年中国心血管外科手术和体外循环数据白皮书[J]. 中国体外循环杂志, 2024, 22(4):197-200. |
| 2 |
GELIJNS A C, MOSKOWITZ A J, ACKER M A, et al. Cardiothoracic Surgical Trials Network (CTSN). Management practices and major infections after cardiac surgery[J]. J Am Coll Cardiol. 2014,64(4):372-381. doi:10.1016/j.jacc.2014.04.052
doi: 10.1016/j.jacc.2014.04.052 |
| 3 | 王丽平,张明杰,陈曦,等. 小儿先天性心脏病术后早期死亡因素分析[J]. 中国小儿急救医学, 2020, 27(7):527-530. |
| 4 |
LUKASIK J, DIERIKX T, BESSELING-VAN DER VAART I,et al. Multispecies Probiotic in AAD Study Group. Multispecies Probiotic for the Prevention of Antibiotic-Associated Diarrhea in Children: A Randomized Clinical Trial[J]. JAMA Pediatr,2022,176(9):860-866. doi:10.1001/jamapediatrics.2022.1973
doi: 10.1001/jamapediatrics.2022.1973 |
| 5 |
MCFARLAND L V, OZEN M, DINLEYICI E C,et al. Comparison of pediatric and adult antibiotic-associated diarrhea and Clostridium difficile infections[J]. World J Gastroenterol, 2016,22(11):3078-3104. doi:10.3748/wjg.v22.i11.3078
doi: 10.3748/wjg.v22.i11.3078 |
| 6 |
ABAD C L R, SAFDAR N. A Review of Clostridioides difficile Infection and Antibiotic-Associated Diarrhea[J]. Gastroenterol Clin North Am,2021,50(2):323-340. doi:10.1016/j.gtc.2021.02.010
doi: 10.1016/j.gtc.2021.02.010 |
| 7 |
ROHIT M, RAJAN P. Approach to Cyanotic Congenital Heart Disease in Children[J]. Indian J Pediatr,2020,87(5):372-380. doi:10.1007/s12098-020-03274-3
doi: 10.1007/s12098-020-03274-3 |
| 8 |
DIAB N S, BARISH S, DONG W, et al. Molecular Genetics and Complex Inheritance of Congenital Heart Disease[J]. Genes (Basel),2021,12(7):1020. doi:10.3390/genes12071020
doi: 10.3390/genes12071020 |
| 9 | 郑跃杰,武庆斌,方峰,等. 儿童抗生素相关性腹泻诊断、治疗和预防专家共识[J]. 中华实用儿科临床杂志,2021,36(6):424-430. |
| 10 | 胡盛寿. 《先天性心脏病外科治疗中国专家共识》述评[J]. 中国胸心血管外科临床杂,2021,28(1):1-3. |
| 11 | 中华人民共和国卫生部. 医院感染诊断标准(试行) [J]. 中华医学杂志, 2001, 81(5):314-320. |
| 12 | 王富海,余健全,罗家怡. 基层医院儿童抗生素相关性腹泻影响因素及肠道感染菌群特征性研究[J]. 广州医学院学报, 2019,47(3):82-86. |
| 13 |
MULLISH B H, WILLIAMS H R. Clostridium difficile infection and antibiotic-associated diarrhoea[J]. Clin Med (Lond),2018,18(3):237-241. doi:10.7861/clinmedicine.18-3-237
doi: 10.7861/clinmedicine.18-3-237 |
| 14 |
ZHANG L, ZENG X, GUO D, et al. Early use of probiotics might prevent antibiotic-associated diarrhea in elderly (>65 years): a systematic review and meta-analysis[J]. BMC Geriatr,2022,22(1):562. doi:10.1186/s12877-022-03257-3
doi: 10.1186/s12877-022-03257-3 |
| 15 | 李珂, 孙建芳, 王吉平. 护士参与抗菌药物管理的研究进展[J]. 中华护理杂志, 2020,55(4):632-636. |
| 16 | 陈丽君,金小娟,傅晓珍,等. 小儿细菌性重症肺炎并发抗生素相关性腹泻危险因素分析[J]. 中国妇幼保健, 2021, 36(9):2114-2117. |
| 17 | 刘秀, 刘滨滨, 权明桃, 等. ICU机械通气患者膈肌锻炼方案的构建及应用研究[J]. 中华护理杂志, 2023,58(3):261-267. |
| 18 | 郭利涛,樊静群,李萌,等. ICU患者应用碳青霉烯类抗菌药物治疗时发生抗生素相关性腹泻的相关因素分析[J]. 中华实用诊断与治疗杂志, 2019, 33(8):823-825. |
| 19 | 林华兰,林美玫,吴明,等. 儿童感染性腹泻病原菌类型及血清SAA,CRP水平对感染的鉴别价值分析[J]. 中国病原生物学杂志, 2023, 18(8):961-964. |
| 20 |
WANG L, GUO G, XU Y, et al. The effect of fecal microbiota transplantation on antibiotic-associated diarrhea and its impact on gut microbiota[J]. BMC Microbiol,2024,24(1):160. doi:10.1186/s12866-024-03261-0
doi: 10.1186/s12866-024-03261-0 |
| 21 |
CHEN K, D'ARC S, SETTY N, et al. In recurrent C. difficile, the CRP response to the primary C. difficile infection predicts whether the same strain or a different strain will cause a second infection[J]. Dig Dis Sci,2013,58(6):1683-1688. doi:10.1007/s10620-012-2534-4
doi: 10.1007/s10620-012-2534-4 |
| 22 | 路钰夏,杨辉,王向辉,等. 病毒感染性腹泻对儿童人群肠道菌群及IL-6,TNF-α,hs-CRP,IFN-γ水平的影响[J]. 中国实验诊断学, 2022, 26(6):842-846. |
| 23 | 郭苗苗,张佳慧. 抗生素相关性腹泻患儿肠道菌群变化与血清细胞因子的关系[J]. 中国微生态学杂志, 2020,32(9):1056-1059,1064. |
| 24 | 刘金响,杜晓泉,史英. 双歧杆菌制剂辅助治疗儿童抗生素相关性腹泻的系统评价与Meta分析[J]. 中国微生态学杂志, 2020,32(2):151-155. |
| 25 |
MEKONNEN S A, MERENSTEIN D, FRASER C M, et al. Molecular mechanisms of probiotic prevention of antibiotic-associated diarrhea[J]. Curr Opin Biotechnol,2020,61:226-234. doi:10.1016/j.copbio.2020.01.005
doi: 10.1016/j.copbio.2020.01.005 |
| 26 | 安佳,德钦卓嘎,郁迪,等. 围手术期使用益生菌对先天性心脏病患儿术后炎症反应的影响[J]. 中华小儿外科杂志, 2024, 45(7):606-612. |
| 27 | 中华预防医学会微生态学分会,舒赛男,王文建. 益生菌儿科临床应用循证指南(2023)[J]. 中国实用儿科杂志,2024,39(1):1-15,20. |
| 28 | 孙芳,许永波,崔广和,等. 基于超声特征构建机器学习模型预测浸润性乳腺癌Luminal分型)[J]. 实用医学杂志,2022,38(18):2306-2311. |
| [1] | Wei LIU,Jun HOU,Longquan TANG,Peng ZHOU,Yan ZHONG,Qinyan LUO,Xiaoyu KUANG,Hua LIU,Ziqing XIONG,Wei XIONG,Chenggao WU,Aiping. LE. Analysis of influencing factors of blood transfusion in children with traumatic brain injury and construction of prediction model: A multi⁃center retrospective study [J]. The Journal of Practical Medicine, 2025, 41(4): 553-560. |
| [2] | Peng XU,Yun ZHOU,Rong JIA,Can QI,Linmeng SHI,Jingda GAO,Dengwei CHU,Xu. GAO. Clinical efficacy of testicular fascial compartment decompression in the treatment of testicular torsion in children [J]. The Journal of Practical Medicine, 2025, 41(2): 220-224. |
| [3] | Zhao WANG,Jiepeng ZUO,Hang CHE,Lingyun REN,Zhe XU,Lei. WANG. Evaluation of plasma PPARγ as a potential diagnostic marker for female interstitial cystitis/painful bladder syndrome and its predictive model [J]. The Journal of Practical Medicine, 2025, 41(2): 258-263. |
| [4] | Bingjie QUAN,Yijing LIU,Xiaoqin LI,Fang ZHOU. Clinical features of hepatitisassociatedaplastic anemia in children [J]. The Journal of Practical Medicine, 2025, 41(1): 84-89. |
| [5] | Qingwen WANG,Shuya ZHANG,Weilin XIONG,Xiaolei HU,Ziwei LI,Qingyin. GUO. Characteristics of oral flora and its metabolites in children with henoch⁃schonlein purpura [J]. The Journal of Practical Medicine, 2024, 40(9): 1244-1250. |
| [6] | Qingqing WANG,Jie DING,Haiwen LI,Zhijian DONG,Yiying WANG,Siqi LIU,Guoji CHANG,Lijuan HUA,Huayi CHEN,Shenghao LI,Yongrui. YANG. Analysis of factors influencing short⁃term adverse clinical outcome in cirrhotic patients with grade 2/3 ascites [J]. The Journal of Practical Medicine, 2024, 40(8): 1114-1120. |
| [7] | Xiaotong LIU,Xianhua SU,Zhijun XIN,Fengqiong GAO,Jiayi FENG,Tongxia. XIA. Risk factors of postoperative complications in patients with spinal tuberculosis and the predictive value of prognostic nutritional index [J]. The Journal of Practical Medicine, 2024, 40(7): 972-978. |
| [8] | Changzhi GUO,Tao SUN,Shuman HAN,Lingxiang WANG,Mengjing. NIU. Risk factors of peripheral infections of knee joint tumor prosthesis and predictive value of serum D⁃dimer and TLR2 [J]. The Journal of Practical Medicine, 2024, 40(6): 814-819. |
| [9] | Xilin WANG,Chanjuan YANG,Daomeng. CHENG. Construction of a nomogram prediction model for aggressive behavior in patients with bipolar disorder [J]. The Journal of Practical Medicine, 2024, 40(5): 677-681. |
| [10] | Hang DENG,Hao. ZHANG. Clinical application of hepatocellular carcinoma prediction models: current challenges and future directions [J]. The Journal of Practical Medicine, 2024, 40(24): 3561-3567. |
| [11] | Huiqun WANG,Chao YE,Chao XU,Si CHEN,Kaiguang ZHANG,Mei. XIAO. A 5⁃year follow⁃up study of rebleeding after endoscopic treatment of esophageal gastric varices rebleeding associated with liver cirrhosis [J]. The Journal of Practical Medicine, 2024, 40(22): 3155-3159. |
| [12] | Shijun LUO,Lizi ZHANG,Dunjin. CHEN. Diagnosis, prevention and treatment of placenta accreta spectrum with non⁃traumatic factors [J]. The Journal of Practical Medicine, 2024, 40(21): 2971-2975. |
| [13] | Lili TANG,Xueming LI,Liming LEI,Xiaodong ZENG,Yun LING,Qiongyu LIN,Sumin. ZHU. Risk factors for prolonged ICU stay after surgery in patients with infective endocarditis [J]. The Journal of Practical Medicine, 2024, 40(20): 2854-2859. |
| [14] | Xing HU,Qingrong LI,Jiang LI,Wei HE,Ping′an HE,Mei LV,Xu. YANG. The Nomogram model was established for the risk assessment of intestinal colonization with neonatal CRKP [J]. The Journal of Practical Medicine, 2024, 40(2): 231-236. |
| [15] | Xiuhua YANG,Yongling YANG,Zhen ZHANG,Jianjun LONG,Tao CHENG,Jian CHEN,Cunhao TIAN. Epidemiological study on common congenital heart disease in children in ethnic minority areas in southeastern Guizhou and influencing factors of delayed medical treatment [J]. The Journal of Practical Medicine, 2024, 40(2): 253-260. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||