实用医学杂志 ›› 2025, Vol. 41 ›› Issue (13): 2039-2044.doi: 10.3969/j.issn.1006-5725.2025.13.014
• 临床研究 • 上一篇
陆煜1,卞兆连2( )
)
Yu LU1,Zhaolian BIAN2()
摘要:
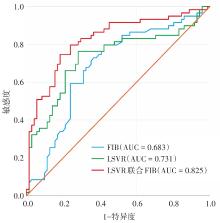
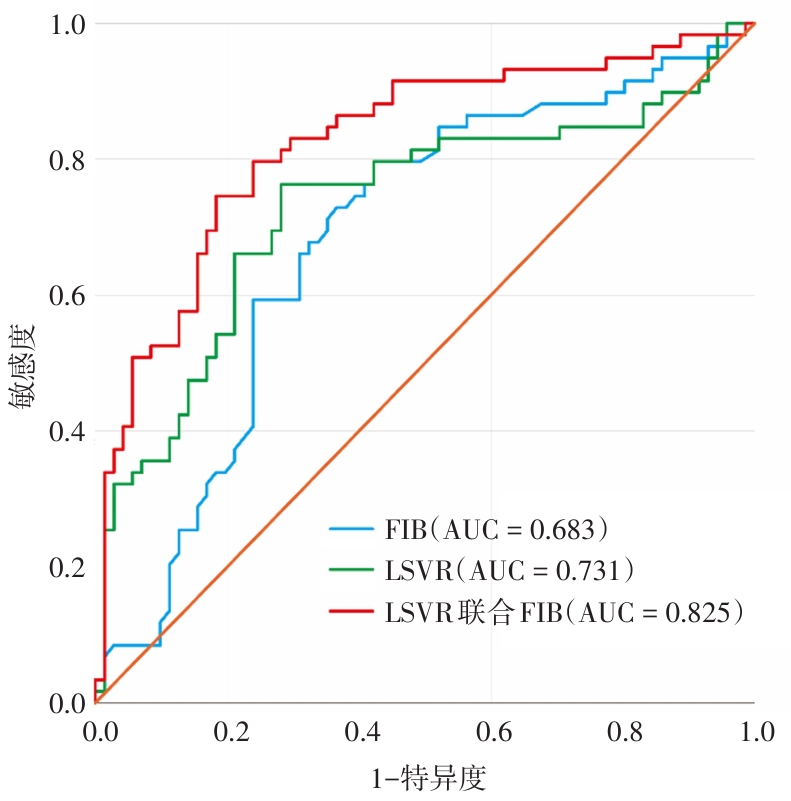
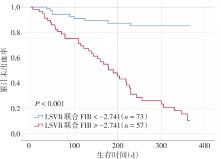
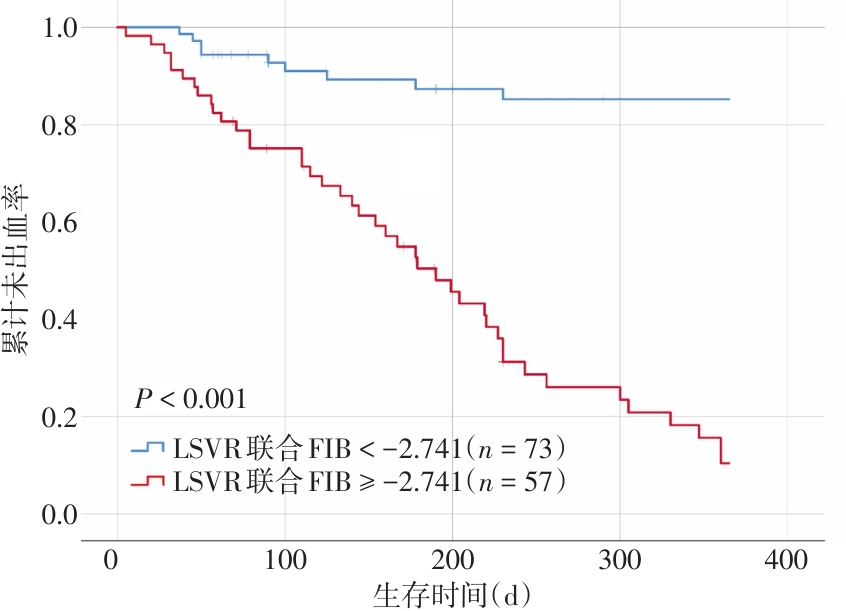
目的 探讨肝脏/脾脏体积比值(liver-to-spleen volume ratio, LSVR)联合血浆纤维蛋白原水平(fibrinogen, FIB)对肝硬化患者食管胃底静脉曲张破裂出血(esophagogastric variceal bleeding, EGVB)风险的预测效能。 方法 采用回顾性病例分析设计,将纳入2020年1月至2022年12月期间在南通市第三人民医院收治的肝硬化合并EGVB患者130例作为观察组。收集患者的临床资料、血常规、血清生化及血凝、CT等检查结果。根据1年内的预后情况将患者分为未出血组(n = 71)和再出血组(n = 59),对于连续变量比较,符合正态分布的变量,采用两样本均数比较的t检验;非正态分布变量,则使用非参数秩和检验;对于分类变量比较,根据数据分布情况,选择χ2检验或Fisher确切概率法进行分析,而后采用logistic回归模型建立LSVR联合FIB的预测模型;ROC曲线分析LSVR、FIB单独及联合的临床效能。计算LSVR联合FIB预测EGVB预后的最佳临界值,Kaplan-Meier法绘制生存曲线。 结果 两组患者AST、FIB、D-二聚体、MELD、ALBI评分、SV、LSVR门静脉直径、脾静脉直径比较差异均有统计学意义(P < 0.05)。多因素分析显示 LSVR(OR = 3.347,95%CI:1.624 ~ 6.899,P = 0.001)和FIB(OR = 0.206,95%CI:0.078 ~ 0.544,P = 0.001)是影响EGVB患者预后的独立危险因素。LSVR联合FIB的ROC曲线下面积(AUC)最大(AUC = 0.825,95%CI:0.751 ~ 0.899),高于单独 LSVR(AUC = 0.731,95%CI:0.639 ~ 0.822)和FIB(AUC = 0.683,95%CI:0.589 ~ 0.777)。LSVR联合FIB最佳临界值为-2.741,特异度为81.7%,敏感度为74.6%,Kaplan-Meier生存分析显示,LSVR联合FIB < -2.741的患者1年未出血率为53.4%(39/73),显著高于LSVR联合FIB ≥ 2.741患者的7.0%(4/57),差异有统计学意义(P < 0.001)。 结论 LSVR联合FIB可以提高单独LSVR和FIB预测EGVB患者1年发生再出血的预测效能。这一模型可能作为一个客观、简单的模型可更好的应用于临床。
中图分类号: