

The Journal of Practical Medicine ›› 2026, Vol. 42 ›› Issue (7): 1257-1264.doi: 10.3969/j.issn.1006-5725.2026.07.019
• Chronic Disease Control • Previous Articles
Ranran DU1,Yuegu WANG2( ),Ying CHEN1,Kunyu ZHANG3
),Ying CHEN1,Kunyu ZHANG3
Received:2025-12-23
Revised:2026-01-22
Accepted:2026-01-26
Online:2026-04-10
Published:2026-04-13
Contact:
Yuegu WANG
E-mail:310319735@qq.com
CLC Number:
Ranran DU,Yuegu WANG,Ying CHEN,Kunyu ZHANG. Comparative of the diagnostic efficiency of VAN and NIHSS in emergency recognition of anterior and posterior circulation acute macrovascular occlusive ischemic stroke[J]. The Journal of Practical Medicine, 2026, 42(7): 1257-1264.
Tab.1
Comparison of basic data between LVO group and non-LVO group"
| 项目 | LVO组 (n = 91) | 非LVO组 (n = 98) | Z/t/χ2值 | P值 |
|---|---|---|---|---|
| 性别/[例(%)] | 0.020 | 0.888 | ||
| 男 | 52(57.14) | 55(56.12) | ||
| 女 | 39(42.86) | 43(43.88) | ||
| 年龄/岁 | 67.52 ± 10.26 | 64.13 ± 11.45 | 2.138 | 0.034 |
| 既往病史/[例(%)] | ||||
| 高血压 | 65(71.43) | 67(68.37) | 0.210 | 0.647 |
| 糖尿病 | 34(37.36) | 31(31.63) | 0.687 | 0.407 |
| 心房颤动 | 31(34.07) | 19(19.39) | 5.225 | 0.022 |
| 冠心病 | 20(21.98) | 19(19.39) | 0.193 | 0.660 |
| 发病至就诊时间[M(P25,P75)]/h | 4.1(1.8,8.3) | 4.6(2.1,9.0) | 1.016 | 0.278 |
| 入院时收缩压/mmHg | 155.72 ± 22.07 | 151.46 ± 18.33 | 1.447 | 0.149 |
| 入院时舒张压/mmHg | 87.89 ± 12.09 | 89.31 ± 13.51 | 0.759 | 0.449 |
| 随机血糖/(mmol/L) | 7.75 ± 2.03 | 7.30 ± 1.97 | 1.546 | 0.124 |
Tab.2
Comparison of NIHSS and VAN scores between LVO group and non-LVO group"
| 组别 | 例数 | NIHSS评分/分 | VAN评分阳性/[例(%)] |
|---|---|---|---|
| LVO组 | 91 | 15.42 ± 4.26 | 77(84.62) |
| 非LVO组 | 98 | 5.26 ± 1.67 | 13(13.27) |
| t/χ2值 | 21.873 | 96.303 | |
| P值 | < 0.001 | < 0.001 |
Tab.3
Logistic regression analysis on independent predictors of LVO"
| 因素 | β | SE | Waldχ2 | OR | 95%CI | P值 |
|---|---|---|---|---|---|---|
| 年龄 | 0.040 | 0.019 | 4.432 | 1.041 | 1.003 ~ 1.080 | 0.036 |
| 合并心房颤动 | 0.573 | 0.208 | 7.589 | 1.774 | 1.180 ~ 2.666 | 0.006 |
| NIHSS评分 | 0.277 | 0.086 | 10.374 | 1.319 | 1.115 ~ 1.561 | 0.001 |
| VAN评分 | 2.529 | 0.490 | 26.638 | 12.541 | 4.800 ~ 32.766 | < 0.001 |
Tab.4
Comparison on the diagnostic efficiency of VAN score and NIHSS score for LVO"
| 指标 | 临界值 | AUC | 95%CI | 敏感度/% | 特异度/% | 阳性预测值/% | 阴性预测值/% |
|---|---|---|---|---|---|---|---|
| NIHSS评分 | > 10分 | 0.863 | 0.805 ~ 0.921 | 82.42 | 87.76 | 86.21 | 84.31 |
| VAN评分 | 阳性 | 0.857 | 0.799 ~ 0.915 | 84.62 | 86.73 | 85.56 | 85.86 |
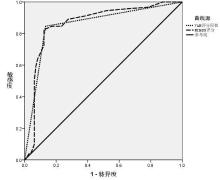
Fig.1
ROC curves analysis of VAN score and NIHSS score in the diagnosis of LVO"
Tab.5
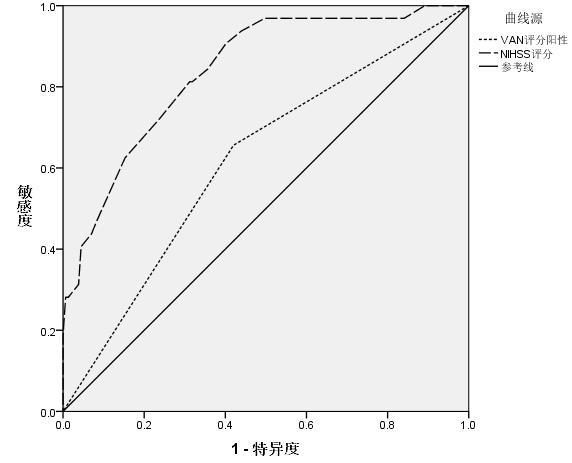
Comparison on the diagnostic efficiency of VAN score and NIHSS score for anterior circulation LVO"
| 指标 | 临界值 | AUC | 95%CI | 敏感度/% | 特异度/% | 阳性预测值/% | 阴性预测值/% |
|---|---|---|---|---|---|---|---|
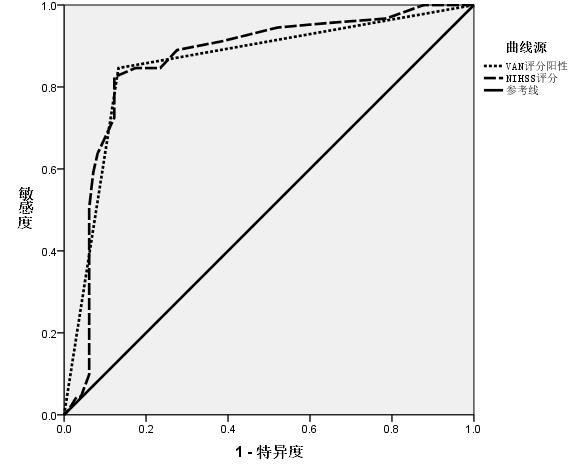
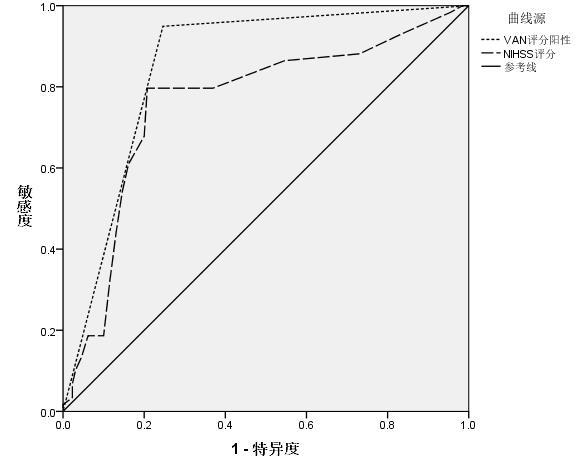
| NIHSS评分 | > 12分 | 0.760 | 0.682 ~ 0.839 | 79.66 | 80.00 | 64.38 | 89.66 |
| VAN评分 | 阳性 | 0.851 | 0.795 ~ 0.908 | 94.92 | 75.38 | 63.64 | 97.03 |
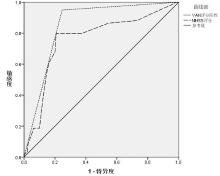
Fig.2
ROC curves analysis of VAN score and NIHSS score in the diagnosis of anterior circulation LVO"
Tab.6
Comparison on the diagnostic efficiency of VAN score and NIHSS score for posterior circulation LVO"
| 指标 | 临界值 | AUC | 95%CI | 敏感度/% | 特异度/% | 阳性预测值/% | 阴性预测值/% |
|---|---|---|---|---|---|---|---|
| NIHSS评分 | > 9分 | 0.839 | 0.766 ~ 0.912 | 90.63 | 63.06 | 33.33 | 97.06 |
| VAN评分 | 阳性 | 0.618 | 0.512 ~ 0.724 | 65.63 | 58.60 | 24.42 | 89.32 |
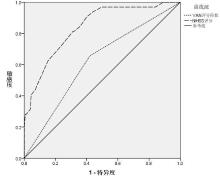
Fig.3
ROC curves analysis of VAN score and NIHSS score in the diagnosis of posterior circulation LVO"
| [1] |
ZHANG H, BAO W, YU M, et al. Neuroimaging marker-CT perfusion of early neurological deterioration in patients with minor stroke and large vessel occlusion after intravenous thrombolysis[J]. Curr Neurovasc Res, 2024, 21(2): 198-204. doi: 10.2174/0115672026306424240319101049 .
doi: 10.2174/0115672026306424240319101049 |
| [2] |
JOINER L, RYAN J, FIESTA M. Including isolated aphasia improves sensitivity and negative predicative value for large vessel occlusion screening[J]. J Stroke Cerebrovasc Dis, 2024, 33(8): 107840. doi: 10.1016/j.jstrokecerebrovasdis.2024.107840 .
doi: 10.1016/j.jstrokecerebrovasdis.2024.107840 |
| [3] |
QIU K, HANG Y, LV P, et al. Thrombectomy in Stroke Patients with Large Vessel Occlusion and Mild Symptoms: Insights from a Multicenter Observational Study[J]. Transl Stroke Res, 2025, 16(5): 1644-1654. doi: 10.1007/s12975-025-01337-1 .
doi: 10.1007/s12975-025-01337-1 |
| [4] |
OZTURAN I U, EMIR D F, KARADAŞ A, et al. External Validation of Vision, Aphasia and Neglect, Ventura Emergent Large Vessel Occlusion and Large Artery Intracranial Occlusion Screening Tools for Emergent Large Vessel Occlusion Stroke: A Multicenter, Prospective, Cross-Sectional Study[J]. J Emerg Med, 2025, 68(6): 15-24. doi: 10.1016/j.jemermed.2024.07.004 .
doi: 10.1016/j.jemermed.2024.07.004 |
| [5] |
CROWE R P, MYERS J B, FERNANDEZ A R, et al. The cincinnati prehospital stroke scale compared to stroke severity tools for large vessel occlusion stroke prediction[J]. Prehosp Emerg Care, 2021, 25(1): 67-75. doi: 10.1080/10903127.2020.1725198 .
doi: 10.1080/10903127.2020.1725198 |
| [6] |
中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国各类主要脑血管病诊断要点2019[J]. 中华神经科杂志, 2019, 52(9): 710-722. doi: 10.3760/cma.j.issn.1006-7876.2019.09.003 .
doi: 10.3760/cma.j.issn.1006-7876.2019.09.003 |
| [7] |
DUKE K, HARTMAN R, ROTH J.Standardization of large vessel occlusion assessment with designated stroke zone decreases door in door out times[J].Stroke, 2020, 51(1): 2-7. doi: 10.1161/STROKEAHA.119.027373 .
doi: 10.1161/STROKEAHA.119.027373 |
| [8] |
BASAGNI B, HAKIKI B, CAMPAGNINI S, et al. Critical issue on the extinction and inattention subtest of NIHSS scale: An analysis on post-acute stroke patients attending inpatient rehabilitation[J]. BMC Neurol, 2021, 21(1): 475. doi: 10.1186/s12883-021-02499-9 .
doi: 10.1186/s12883-021-02499-9 |
| [9] |
CROWE R P, MYERS J B, FERNANDEZ A R, et al. The Cincinnati Prehospital Stroke Scale Compared to Stroke Severity Tools for Large Vessel Occlusion Stroke Prediction[J]. Prehosp Emerg Care, 2021, 25(1): 67-75. doi: 10.1080/10903127.2020.1725198 .
doi: 10.1080/10903127.2020.1725198 |
| [10] |
SUN D, HUO X, JIA B, et al. Delayed neurological improvement after endovascular treatment for acute large vessel occlusion: Data from ANGEL-ACT registry[J]. J Thromb Thrombolysis, 2023, 55(1): 1-8. doi: 10.1007/s11239-022-02712-7 .
doi: 10.1007/s11239-022-02712-7 |
| [11] |
CLAUS J J, BERGHOUT B B P, BOX C V J, et al. Characterizing TIA and stroke symptomatology in a population-based study: Implications for and diagnostic value of FAST-based public education[J]. BMC Public Health, 2024, 24(1): 3512. doi: 10.1186/s12889-024-20960-5 .
doi: 10.1186/s12889-024-20960-5 |
| [12] |
OSPEL J M, BROWN S, BOSSHART S, et al. Modified Rankin Scale at 90 Days Versus National Institutes of Health Stroke Scale at 24 Hours as Primary Outcome in Acute Stroke Trials[J]. J Am Heart Assoc, 2025, 14(5): e037752. doi: 10.1161/JAHA.124.037752 .
doi: 10.1161/JAHA.124.037752 |
| [13] |
JOHANSEN T, MATRE M, LØVSTAD M, et al. Virtual reality as a method of cognitive training of processing speed, working memory, and sustained attention in persons with acquired brain injury: A protocol for a randomized controlled trial[J]. Trials, 2024, 25(1): 340. doi: 10.1186/s13063-024-08178-7 .
doi: 10.1186/s13063-024-08178-7 |
| [14] |
MOZUMDER A S, BANDELA S, BIRNBAUM L.Inclusion of Asymmetric Bilateral Weakness Optimizes VAN Pre-hospital LVO Triage (P17-10.006)[J]. Neurology, 2022, 98(18): 105-107. doi: 10.1212/WNL.0000000000200110 .
doi: 10.1212/WNL.0000000000200110 |
| [15] |
ROWLING H, ITALIANO D, CHURILOV L, et al. Large vessel occlusive stroke with milder baseline severity shows better collaterals and reduced harm from thrombectomy transfer delays[J]. Int J Stroke, 2024, 19(7): 772-778. doi: 10.1177/17474930241242954 .
doi: 10.1177/17474930241242954 |
| [16] |
SILVA A H, ALVES P N, FONSECA A C, et al. Neglect scoring modifications in the National Institutes of Health Stroke Scale improve right hemisphere stroke lesion volume prediction[J]. Eur J Neurol, 2024, 31(2): e16133. doi: 10.1111/ene.16133 .
doi: 10.1111/ene.16133 |
| [17] |
HAVENON A, AYODELE I, ALHANTI B, et al. Prediction of large vessel occlusion stroke using clinical registries for research[J]. Neurology, 2024, 102(11): e209424. doi: 10.1212/WNL.0000000000209424 .
doi: 10.1212/WNL.0000000000209424 |
| [18] |
PATEL M D, THOMPSON J, CABAÑAS J G, et al. Performance of the vision, aphasia, neglect (VAN) assessment within a single large EMS system[J]. J Neurointerv Surg, 2022, 14(4): 341-345. doi: 10.1136/neurintsurg-2020-017217 .
doi: 10.1136/neurintsurg-2020-017217 |
| [19] |
MARTO J P, QURESHI M, NAGEL S, et al. Endovascular therapy for patients with low NIHSS scores and large vessel occlusion in the 6- to 24-Hour window: Analysis of the CLEAR study[J]. Neurology, 2025, 104(7): e213442. doi: 10.1212/WNL.0000000000213442 .
doi: 10.1212/WNL.0000000000213442 |
| [20] |
杨成双, 刘圣, 梁堃, 等. 后循环颅内动脉粥样硬化性急性大血管闭塞的早期识别[J]. 介入放射学杂志, 2025, 34(1): 18-23. doi: 10.3969/j.issn.1008-794X.2025.01.003 .
doi: 10.3969/j.issn.1008-794X.2025.01.003 |
| [21] |
KURIBARA T, IIHOSHI S, TSUKAGOSHI E, et al. Thrombectomy for acute large vessel occlusion in posterior and anterior circulation: A single institutional retrospective observational study[J]. Neuroradiology, 2022, 64(3): 565-574. doi: 10.1007/s00234-021-02799-4 .
doi: 10.1007/s00234-021-02799-4 |
| [22] |
林子君, 李玮. 后循环急性大血管闭塞性卒中的诊疗进展[J]. 中国脑血管病杂志, 2023, 20(2): 119-125. doi: 10.3969/j.issn.1672-5921.2023.02.008 .
doi: 10.3969/j.issn.1672-5921.2023.02.008 |
| [23] |
BIRNBAUM L, WAMPLER D, SHADMAN A, et al. Paramedic utilization of Vision, Aphasia, Neglect (VAN) stroke severity scale in the prehospital setting predicts emergent large vessel occlusion stroke[J]. J Neurointerv Surg, 2021, 13(6): 505-508. doi: 10.1136/neurintsurg-2020-016054 .
doi: 10.1136/neurintsurg-2020-016054 |
| [24] |
HENDRIX P, KILLER-OBERPFALZER M, BROUSSALIS E, et al. Mechanical thrombectomy for anterior versus posterior circulation large vessel occlusion stroke with emphasis on posterior circulation outcomes[J]. World Neurosurg, 2022, 158(6): e416-e422. doi: 10.1016/j.wneu.2021.10.187 .
doi: 10.1016/j.wneu.2021.10.187 |
| [25] |
ZHANG L, BU X, LIAO J, et al. Prospective evaluation of modified Cincinnati Prehospital Stroke Severity Scale for identifying large vessel occlusion[J]. J Clin Neurosci, 2025, 134(6): 111077. doi: 10.1016/j.jocn.2025.111077 .
doi: 10.1016/j.jocn.2025.111077 |
| [26] |
KOTHARI S A, MORSI R Z, KOZEL O A, et al. Comparing validated stroke screening scales for identifying large and medium vessel occlusions: A prospective observational cohort study[J]. J Neurointerv Surg, 2025, 17(12): 1320-1324. doi: 10.1136/jnis-2024-022309 .
doi: 10.1136/jnis-2024-022309 |
| [27] |
FEIL K, MATUSEVICIUS M, HERZBERG M, et al. Minor stroke in large vessel occlusion: A matched analysis of patients from the German Stroke Registry-Endovascular Treatment (GSR-ET) and patients from the Safe Implementation of Treatments in Stroke-International Stroke Thrombolysis Register (SITS-ISTR)[J]. Eur J Neurol, 2022, 29(6): 1619-1629. doi: 10.1111/ene.15272 .
doi: 10.1111/ene.15272 |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||