

The Journal of Practical Medicine ›› 2025, Vol. 41 ›› Issue (10): 1575-1583.doi: 10.3969/j.issn.1006-5725.2025.10.021
• Medical Examination and Clinical Diagnosis • Previous Articles
Qiannan JIANG1,Tingting LIU2,Yingying LIU1,Kaijie CUI1,Xiuxiang. LIU1( )
)
Received:2025-01-03
Online:2025-05-25
Published:2025-05-21
Contact:
Xiuxiang. LIU
E-mail:liuxiuxiang99@163.com
CLC Number:
Qiannan JIANG,Tingting LIU,Yingying LIU,Kaijie CUI,Xiuxiang. LIU. Patent ductus arteriosus severity predicts the occurrence and mortality of pulmonary hemorrhage in premature infants with gestational age ≤ 32 weeks[J]. The Journal of Practical Medicine, 2025, 41(10): 1575-1583.
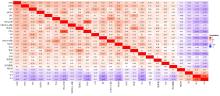
Fig.1
Heatmap of correlation analysis of clinical characteristics between premature infants ≤ 32 weeks of gestational age with NPH and no-NPH"
Tab.1
Analysis of clinical characteristic differences between premature infants ≤32 weeks of gestational age"
| 项目 | NPH组 (n = 92) | no-NPH组 (n = 419) | χ2 /Z值 | P值 | 项目 | NPH组 (n = 92) | no-NPH组 (n = 419) | χ2 /Z值 | P值 |
|---|---|---|---|---|---|---|---|---|---|
| GA[M(P25, P75)]/周 | 27.8(26.5,29.1) | 29(27.5,30.6) | -5.471 | < 0.001 | ROP | 33(36.3) | 140(33.4) | 0.271 | 0.603 |
| W[M(P25, P75)]T/g | 1 070(920,1 215) | 1 180(1 000,1 480) | -4.698 | < 0.001 | NEC(3—4级) | 10(10.9) | 50(11.9) | 0.082 | 0.774 |
| 男 | 56(60.9) | 240(57.3) | 0.399 | 0.528 | MV[M(P25, P75)]/d | 8(3, 16) | 1(1, 4) | -10.009 | < 0.001 |
| 经阴分娩 | 50(54.3) | 200(47.7) | 1.321 | 0.250 | CPAP[M(P25, P75)]/d | 12(0, 24.7) | 9(3, 23) | -0.337 | 0.736 |
| GDM | 18(19.6) | 103(24.6) | 1.051 | 0.305 | IVH | 54(58.7) | 93(22.2) | 49.044 | < 0.001 |
| HDP | 18(19.6) | 79(18.9) | 0.025 | 0.875 | IVH(3—4级) | 24(26.1) | 27(6.4) | 32.398 | < 0.001 |
| PROM | 24(26.1) | 164(39.1) | 5.528 | 0.019 | HFO | 46(50.0) | 42(10.0) | 84.567 | < 0.001 |
| PA | 17(18.5) | 75(17.9) | 0.017 | 0.896 | 低体温 | 11(12.0) | 15(3.6) | 10.961 | 0.001 |
| 宫内感染 | 67(72.8) | 255(60.9) | 4.635 | 0.031 | 低血压 | 39(42.4) | 63(15.0) | 35.334 | < 0.001 |
| IVF | 27(29.3) | 71(16.9) | 7.487 | 0.006 | 休克 | 22(23.9) | 34(8.1) | 19.295 | < 0.001 |
| AS | 53(57.6) | 330(78.8) | 17.974 | < 0.001 | DIC | 20(21.7) | 9(2.1) | 54.088 | < 0.001 |
| NA | 58(63.0) | 164(39.1) | 17.541 | < 0.001 | PDA | 92(100.0) | 298(71.1) | 34.811 | < 0.001 |
| NRDS | 75(81.5) | 208(49.6) | 31.026 | < 0.001 | hsPDA | 46(50.0) | 56(13.4) | 63.371 | < 0.001 |
| NRDS(3—4级) | 37(40.2) | 49(11.7) | 43.845 | < 0.001 | PDA内径[M(P25, P75)]/mm | 2.4(2.0,2.9) | 1.8(0, 2.3) | -6.736 | < 0.001 |
| EOS | 15(16.3) | 22(5.3) | 13.723 | < 0.001 | LA[M(P25, P75)]/AO | 1.33(1.2, 1.5) | 1.30(1.2, 1.4) | -0.180 | 0.857 |
| LOS | 16(17.4) | 46(11.0) | 2.910 | 0.088 | PAH | 28(30.4) | 48(11.5) | 21.462 | < 0.001 |
| BPD | 61(66.3) | 243(58.0) | 2.161 | 0.142 | CD | 15(16.3) | 9(2.1) | 33.774 | < 0.001 |
| NP | 64(69.6) | 304(72.6) | 0.334 | 0.563 |
Tab.2
Multivariate regression logistic analysis of infants ≤ 32 weeks of gestational age with and without NPH"
| 项目 | β | SE | Wald χ2 | P值 | OR | 95%CI |
|---|---|---|---|---|---|---|
| GA | 0.067 | 0.146 | 0.212 | 0.646 | 1.070 | 0.803 ~ 1.425 |
| WT | 0.001 | 0.001 | 1.346 | 0.246 | 1.001 | 0.999 ~ 1.003 |
| PROM | -0.122 | 0.360 | 0.115 | 0.735 | 0.885 | 0.437 ~ 1.793 |
| 宫内感染 | 0.106 | 0.368 | 0.084 | 0.773 | 1.112 | 0.541 ~ 2.286 |
| IVF | -0.226 | 0.401 | 0.319 | 0.572 | 0.797 | 0.364 ~ 1.749 |
| AS | 0.162 | 0.356 | 0.208 | 0.648 | 1.176 | 0.585 ~ 2.364 |
| NA | 0.076 | 0.367 | 0.043 | 0.835 | 1.079 | 0.525 ~ 2.218 |
| NRDS | -0.792 | 0.432 | 3.364 | 0.067 | 0.453 | 0.194 ~ 1.056 |
| NRDS(3—4级) | 0.971 | 0.374 | 6.727 | 0.009 | 2.641 | 1.268 ~ 5.501 |
| EOS | 0.844 | 0.502 | 2.821 | 0.093 | 2.325 | 0.869 ~ 6.222 |
| IVH | 0.74 | 0.372 | 3.963 | 0.047 | 2.097 | 1.012 ~ 4.346 |
| IVH(3—4级) | 0.324 | 0.479 | 0.456 | 0.499 | 1.382 | 0.540 ~ 3.538 |
| MV | 0.063 | 0.016 | 16.047 | 0.000 | 1.065 | 1.033 ~ 1.098 |
| HFO | 0.832 | 0.376 | 4.909 | 0.027 | 2.298 | 1.101 ~ 4.797 |
| 低体温 | 0.419 | 0.573 | 0.533 | 0.465 | 1.520 | 0.494 ~ 4.678 |
| 低血压 | 0.762 | 0.418 | 3.319 | 0.068 | 2.144 | 0.944 ~ 4.868 |
| 休克 | -0.799 | 0.530 | 2.272 | 0.132 | 0.450 | 0.159 ~ 1.271 |
| DIC | 1.714 | 0.613 | 7.823 | 0.005 | 5.550 | 1.670 ~ 18.446 |
| PDA | 19.673 | 3 229.065 | 0.000 | 0.995 | 3.497 | 0.000 |
| hsPDA | 1.340 | 0.362 | 13.689 | 0.000 | 3.820 | 1.878 ~ 7.768 |
| PDA内径 | -0.334 | 0.241 | 1.923 | 0.166 | 0.716 | 0.447 ~ 1.148 |
| PAH | -0.011 | 0.401 | 0.001 | 0.979 | 0.990 | 0.451 ~ 2.173 |
| CD | 0.288 | 0.615 | 0.219 | 0.639 | 1.334 | 0.400 ~ 4.448 |
| 常量 | -43.379 | 4 634.193 | 0.000 | 0.993 | 0.000 |
Tab.3
Analysis of clinical characteristic differences of NPH Patients ≤32 weeks of gestational age with and without hsPDA"
| 项目 | hsPDA组 (n = 46) | no-hsPDA组 (n = 46) | χ2 /Z值 | P值 | 项目 | NPH组 (n = 46) | no-NPH组 (n = 46) | χ2 /Z值 | P值 |
|---|---|---|---|---|---|---|---|---|---|
| GA/周 | 28.2(27.0,29.7) | 27.3(26.1,28.5) | -2.367 | 0.018 | AS/[例(%)] | 27(58.7) | 26(56.5) | 0.045 | 0.833 |
| WT/kg | 1.1(0.9,1.2) | 1(0.8,1.2) | -2.691 | 0.007 | NA/[例(%)] | 24(52.2) | 34(73.9) | 4.665 | 0.031 |
| PDAsc | 7.0(5.2,9.5) | 3.8(1.7,5.4) | -5.060 | < 0.001 | NRDS/[例(%)] | 35(76.1) | 40(87.0) | 1.804 | 0.179 |
| PDA内径/mm | 2.8(2.1,3.2) | 2.0(1.5,2.5) | -4.268 | < 0.001 | NRDS(3—4级)/[例(%)] | 20(43.5) | 17(37.0) | 0.407 | 0.524 |
| PDA血流速度/(m/s) | 1.8(1.6,2.3) | 2.9(2.9,3.4) | -8.022 | < 0.001 | EOS/[例(%)] | 10(21.7) | 5(10.9) | 1.991 | 0.158 |
| LVO/[mL/(kg·min)] | 565.0(475.9,626.1) | 285.7(274.3,291.6) | -8.262 | < 0.001 | IVH/[例(%)] | 26(56.5) | 28(60.9) | 0.179 | 0.672 |
| VTI/cm | 14.6(14.0,15.1) | 12.4(12.0,12.8) | -7.776 | < 0.001 | IVH(3—4级)/[例(%)] | 12(26.1) | 12(26.1) | < 0.001 | 1.000 |
| 心率/(次/min) | 168.0(160.0,171.7) | 115(111,122) | -8.274 | < 0.001 | MV/d | 7(2,14) | 10(4.7,23) | -1.817 | 0.069 |
| AO/cm2 | 0.26(0.24,0.27) | 0.20(0.18,0.21) | -7.063 | < 0.001 | HFO/[例(%)] | 22(47.8) | 24(52.2) | 0.174 | 0.677 |
| LV a'/(cm/s) | 3(3,4) | 6(5,6) | -7.261 | < 0.001 | 低体温/[例(%)] | 8(17.4) | 3(6.5) | 2.581 | 0.108 |
| EDV/(m/s) | -0.053(-0.07,-0.04) | 0.02(0.01,0.03) | -8.256 | < 0.001 | 低血压/[例(%)] | 15(32.6) | 24(52.2) | 3.605 | 0.058 |
| LA/AO | 1.5(1.3,1.6) | 1.2(1.2,1.3) | -6.308 | < 0.001 | 休克/[例(%)] | 12(26.1) | 10(21.7) | 0.239 | 0.625 |
| PAH/[例(%)] | 17(37.0) | 11(23.9) | 1.848 | 0.174 | DIC/[例(%)] | 11(23.9) | 9(19.6) | 0.256 | 0.613 |
| CD/[例(%)] | 9(19.6) | 6(13.0) | 0.717 | 0.397 | |||||
| PROM/[例(%)] | 11(23.9) | 13(28.3) | 0.225 | 0.635 | |||||
| PA/[例(%)] | 5(10.9) | 12(26.1) | 3.536 | 0.060 | |||||
| 宫内感染/[例(%)] | 31(67.4) | 36(78.3) | 1.373 | 0.241 | |||||
| IVF/[例(%)] | 14(30.4) | 13(28.3) | 0.052 | 0.919 |

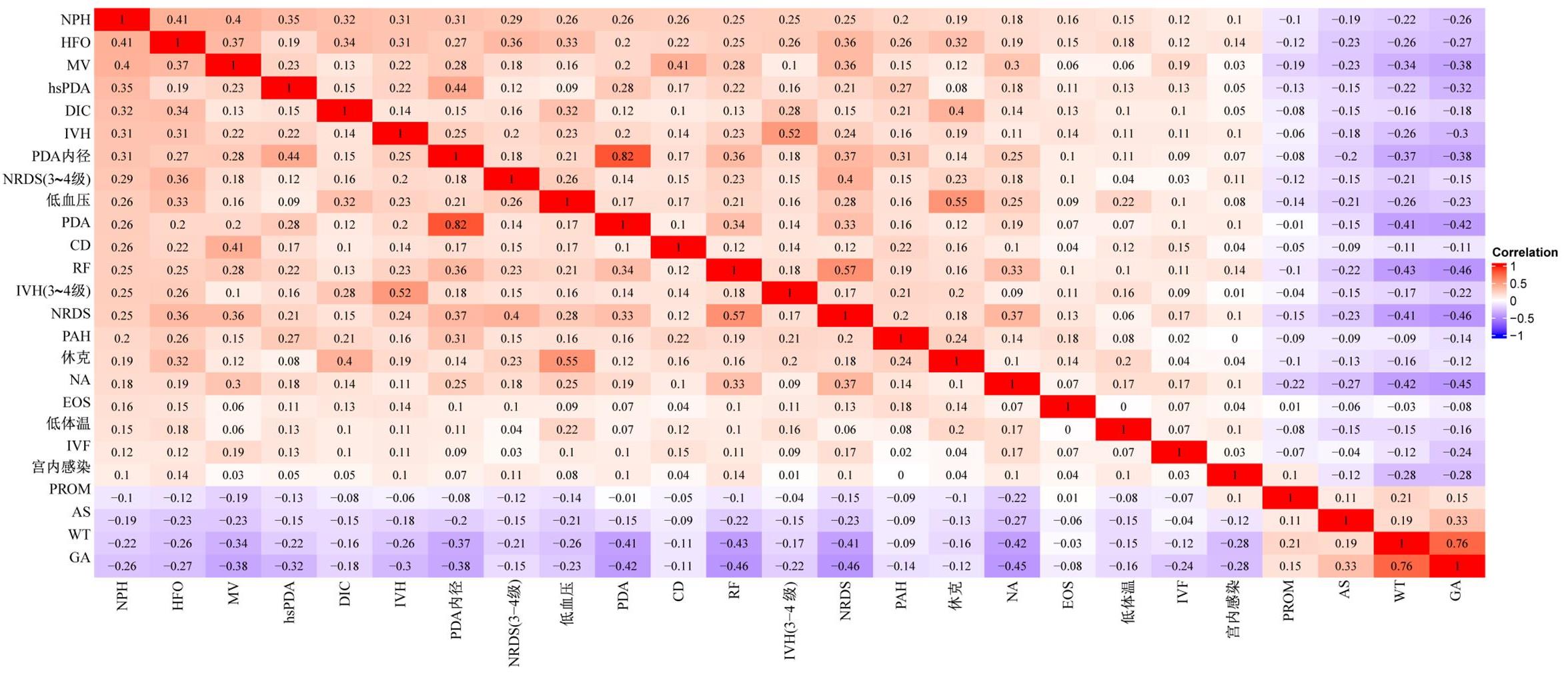
Fig.2
Comparative analysis of PDAsc between the survival group and the non-survival group in infants with NPH and coexisting PDA"
Tab.4
Analysis of differences in PDA related clinical characteristics between non-survivor group and survivor group of infants ≤ 32 weeks of gestational age with NPH and coexisting PDA M(P25, P75)"
| 项目 | 死亡组(n = 38) | 存活组(n = 54) | χ2 /Z值 | P值 |
|---|---|---|---|---|
| PDAsc/分 | 6.5(3.8, 10.2) | 4.3(2.0, 6.2) | -3.037 | 0.002 |
| PDA内径/mm | 2.0(2.0, 3.1) | 2.5(2.0, 2.8) | -0.232 | 0.817 |
| PDA血流速度/(m/s) | 2.45(1.8, 2.92) | 2.5(1.95, 2.9) | -0.690 | 0.490 |
| LVO/[mL/(kg·min)] | 480.9(288.3, 610.1) | 295.7(282.6, 511.4) | -2.296 | 0.022 |
| VTI/cm | 13.8(12.4, 15.0) | 13.0(12.3, 14.3) | -1.222 | 0.222 |
| 心率/(次/min) | 157.5(112.0, 171.7) | 125(116.0, 166.2) | -0.814 | 0.416 |
| AO/cm2 | 0.21(0.19, 0.27) | 0.22(0.20, 0.26) | -0.492 | 0.623 |
| LV a′/(cm/s) | 4(3, 5) | 5(4, 6) | -2.741 | 0.006 |
| EDV/(m/s) | -0.02(-0.05, 0.02) | 0.00(-0.05, 0.02) | -0.377 | 0.706 |
| LA/AO | 1.4(1.2, 1.5) | 1.33(1.2, 1.4) | -1.127 | 0.260 |
| PAH/[例(%)] | 15(39.5) | 13(24.1) | 2.498 | 0.114 |
| CD[例(%)] | 9(23.7) | 6(11.1) | 2.584 | 0.108 |
Tab.5
Multivariate regression logistic analysis of factors associated with mortality in infants ≤32 weeks of gestational age with NPH and coexisting PDA"
| 项目 | β | SE | Wald χ2 | P值 | OR | 95%CI |
|---|---|---|---|---|---|---|
| PDAsc | 0.235 | 23 647.730 | 5.086 | 0.024 | 1.265 | 1.031 ~ 1.553 |
| LVO/[mL/(kg·min)] | -0.003 | 101 876.520 | 1.061 | 0.303 | 0.997 | 0.992 ~ 1.003 |
| LV a′/(cm/s) | -0.430 | 17 103.142 | 2.531 | 0.112 | 0.651 | 0.383 ~ 1.105 |
| 常量 | 1.403 | 16 519.471 | 0.496 | 0.481 | 4.066 |
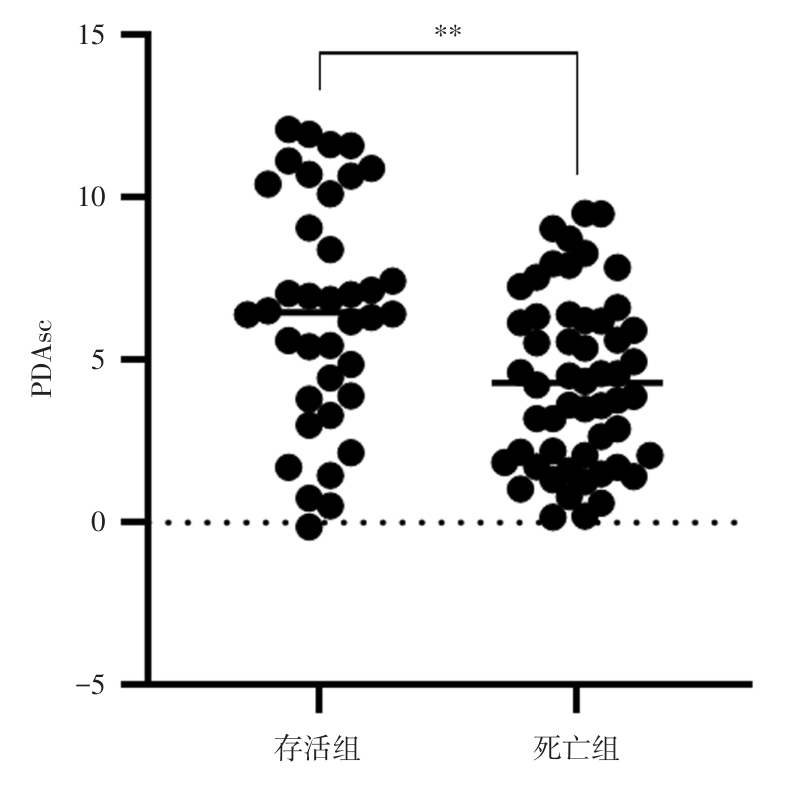
Fig.3
Relationship between PDAsc and the predicted probability of death in infants with NPH and coexisting PDA"
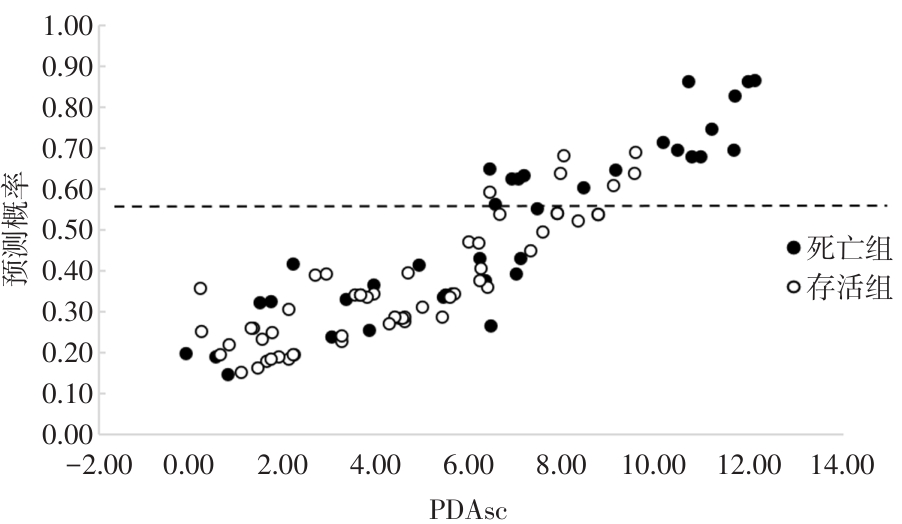
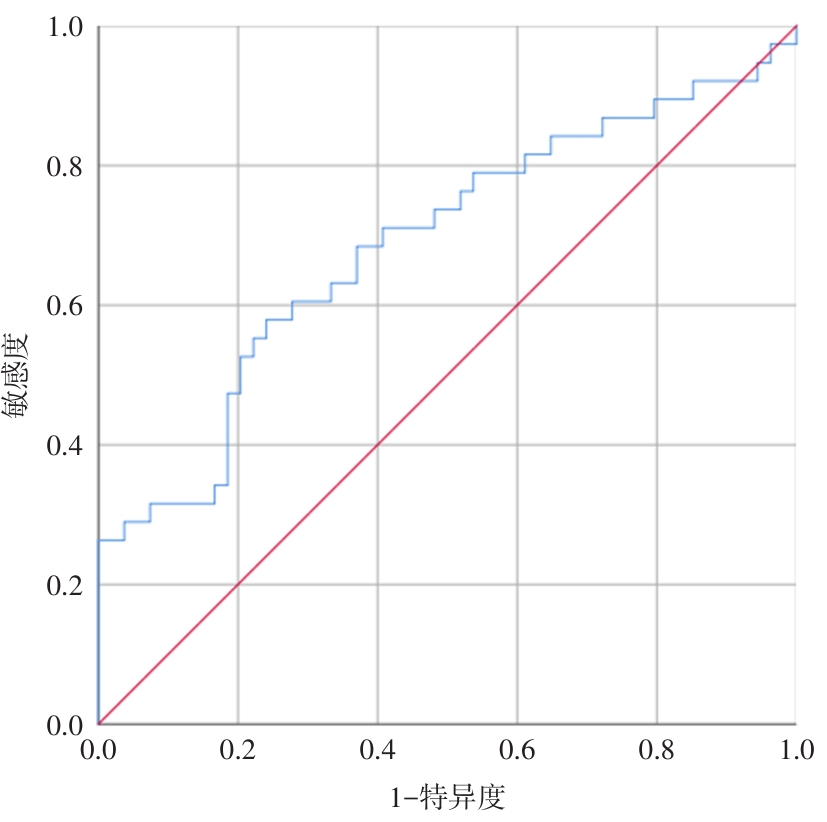
Fig.4
ROC curve for PDAsc in infants with NPH and coexisting PDA resulting in death"
| 1 |
FERREIRA C H, CARMONA F, MARTINEZ F E. Prevalence, risk factors and outcomes associated with pulmonary hemorrhage in newborns[J]. J Pediatr (Rio J), 2014, 90(3):316-322. doi:10.1016/j.jped.2013.12.008
doi: 10.1016/j.jped.2013.12.008 |
| 2 | 多中心极低和超低出生体质量儿的预后评估协作组. 超早产儿和超低出生体质量儿的死亡原因:多中心前瞻性队列研究[J]. 中华围产医学杂志,2020,23(8):530-538. |
| 3 | 张二清,郑明琼,徐小静. 143例新生儿肺出血不良预后原因分析[J]. 中国研究型医院,2022,9(4):64-67. |
| 4 |
AHMAD K A, BENNETT M M, AHMAD S F, et al. Morbidity and mortality with early pulmonary haemorrhage in preterm neonates[J]. Arch Dis Child Fetal Neonatal Ed, 2019, 104(1):F63-F68. doi:10.1136/archdischild-2017-314172
doi: 10.1136/archdischild-2017-314172 |
| 5 | 齐敏,张烨,杨世炳,等. 超早产儿肺出血临床特点及高危因素研究[J]. 中华新生儿科杂志(中英文),2023,38(4):200-204. |
| 6 | 刘莹莹,江倩男,刘秀香. 极低及超低出生体质量儿肺出血的危险因素分析[J]. 国际儿科学杂志,2023,50(1):61-65. |
| 7 | 郭玮,李清峰,吴明赴,等. 新生儿肺出血危险因素的临床分析[J]. 国际医药卫生导报,2020,26(2):162-165. |
| 8 | 蒋更盼,李杨方. 早产儿呼吸窘迫综合征并发肺出血的危险因素分析[J]. 中国基层医药,2023,30(11):1662-1666. |
| 9 |
KAPPICO J M, CAYABYAB R, EBRAHIMI M, et al. Pulmonary hemorrhage in extremely low birth weight infants: Significance of the size of left to right shunting through a valve incompetent patent foramen ovale[J]. J Perinatol, 2022, 42(9):1233-1237. doi:10.1038/s41372-022-01464-9
doi: 10.1038/s41372-022-01464-9 |
| 10 | 中华医学会儿科学分会新生儿学组. 新生儿肺出血的诊断与治疗方案[J]. 中国实用儿科杂志,2001,16(10):631. |
| 11 |
SWEET D G, CARNIELLI V P, GREISEN G, et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome: 2022 Update[J]. Neonatology, 2023, 120(1):3-23. doi:10.1159/000528914
doi: 10.1159/000528914 |
| 12 | 高翔羽. 极/超早产儿有血流动力学意义的动脉导管未闭的管理策略[J]. 中华新生儿科杂志(中英文),2024,39(2):65-69. |
| 13 |
ROBERTS A G, YOUNGE N, GREENBERG R G. Neonatal Necrotizing Enterocolitis: An Update on Pathophysiology, Treatment, and Prevention[J]. Paediatr Drugs, 2024, 26(3):259-275. doi:10.1007/s40272-024-00626-w
doi: 10.1007/s40272-024-00626-w |
| 14 |
HIGGINS R D, JOBE A H, KOSO-THOMAS M, et al. Bronchopulmonary Dysplasia: Executive Summary of a Workshop[J]. J Pediatr, 2018, 197:300-308. doi:10.1016/j.jpeds.2018.01.043
doi: 10.1016/j.jpeds.2018.01.043 |
| 15 | 邵肖梅,叶鸿瑁,丘小汕. 实用新生儿学[M]. 5版. 北京:人民卫生出版社,2019. |
| 16 |
EL-KHUFFASH A, JAMES A T, CORCORAN JD, et al. A Patent Ductus Arteriosus Severity Score Predicts Chronic Lung Disease or Death before Discharge[J]. J Pediatr, 2015, 167(6):1354-1361.e2. doi:10.1016/j.jpeds.2015.09.028
doi: 10.1016/j.jpeds.2015.09.028 |
| 17 |
WANG T T, ZHOU M, HU X F, et al. Perinatal risk factors for pulmonary hemorrhage in extremely low-birth-weight infants[J]. World J Pediatr, 2020, 16(3):299-304. doi:10.1007/s12519-019-00322-7
doi: 10.1007/s12519-019-00322-7 |
| 18 |
KAPPICO J M, CAYABYAB R, EBRAHIMI M, et al. Pulmonary hemorrhage in extremely low birth weight infants: Significance of the size of left to right shunting through a valve incompetent patent foramen ovale[J]. J Perinatol, 2022, 42(9):1233-1237. doi:10.1038/s41372-022-01464-9
doi: 10.1038/s41372-022-01464-9 |
| 19 | 蒋丽军,于倩,王伏东,等. 血压变异性联合脑血流参数在预测极低出生体质量早产儿脑室内出血的作用[J]. 实用医学杂志,2023,39(16):2116-2121. |
| 20 | 张素娥,陈春,陈思齐,等. 胎膜早破时间对< 34周早产儿早期结局的影响[J]. 实用医学杂志,2021,37 (15): 1976-1981. |
| 21 |
KLUCKOW M, JEFFERY M, GILL A, et al. A randomised placebo-controlled trial of early treatment of the patent ductus arteriosus[J]. Arch Dis Child Fetal Neonatal Ed, 2014, 99(2):F99-F104. doi:10.1136/archdischild-2013-304695
doi: 10.1136/archdischild-2013-304695 |
| 22 |
HAMRICK S E G, SALLMON H, ROSE A T, et al. Patent Ductus Arteriosus of the Preterm Infant[J]. Pediatrics, 2020, 146(5):e20201209. doi:10.1542/peds.2020-1209
doi: 10.1542/peds.2020-1209 |
| 23 |
NOORI S, MCCOY M, FRIEDLICH P, et al. Failure of Ductus Arteriosus Closure Is Associated With Increased Mortality in Preterm Infants[J]. Pediatrics, 2009, 123(1):e138-e144. doi:10.1542/peds.2008-2418
doi: 10.1542/peds.2008-2418 |
| [1] | Tong DUAN,Qi WU,Hui. LIU. Correlation between iron death⁃related gene expression level and myocardial dysfunction and prognosis in sepsis [J]. The Journal of Practical Medicine, 2025, 41(6): 846-851. |
| [2] | Runfang WANG,Ya DUAN,Liyan DU,Xiaodan LIU,Wenning LIAN,Yan HUO,Dandan. YANG. Epidemiological status and risk factors associated with placental abruption among pregnant women in Hebei Province [J]. The Journal of Practical Medicine, 2025, 41(6): 904-910. |
| [3] | Dongli LIU,Zilin QUAN,Lingxiu ZHONG,Qiqi CHEN,Wenqiao CAI,Senpei ZHUANG,Ying WEI,Huiyi PAN,Yawen. LIN. Construction and validation of a predictive model for antibiotic-associated diarrhea after surgery in children with congenital heart disease [J]. The Journal of Practical Medicine, 2025, 41(5): 683-690. |
| [4] | Qiaoying MO,Fangyi ZHU,Cunkui ZHU,Shenglong. MA. Nomogram model of malnutrition risk in patients suffering from chronic heart failure grounded on GNRI score [J]. The Journal of Practical Medicine, 2025, 41(5): 691-698. |
| [5] | Qingqing WANG,Jie DING,Haiwen LI,Zhijian DONG,Yiying WANG,Siqi LIU,Guoji CHANG,Lijuan HUA,Huayi CHEN,Shenghao LI,Yongrui. YANG. Analysis of factors influencing short⁃term adverse clinical outcome in cirrhotic patients with grade 2/3 ascites [J]. The Journal of Practical Medicine, 2024, 40(8): 1114-1120. |
| [6] | Xiaotong LIU,Xianhua SU,Zhijun XIN,Fengqiong GAO,Jiayi FENG,Tongxia. XIA. Risk factors of postoperative complications in patients with spinal tuberculosis and the predictive value of prognostic nutritional index [J]. The Journal of Practical Medicine, 2024, 40(7): 972-978. |
| [7] | Changzhi GUO,Tao SUN,Shuman HAN,Lingxiang WANG,Mengjing. NIU. Risk factors of peripheral infections of knee joint tumor prosthesis and predictive value of serum D⁃dimer and TLR2 [J]. The Journal of Practical Medicine, 2024, 40(6): 814-819. |
| [8] | Xilin WANG,Chanjuan YANG,Daomeng. CHENG. Construction of a nomogram prediction model for aggressive behavior in patients with bipolar disorder [J]. The Journal of Practical Medicine, 2024, 40(5): 677-681. |
| [9] | Huiqun WANG,Chao YE,Chao XU,Si CHEN,Kaiguang ZHANG,Mei. XIAO. A 5⁃year follow⁃up study of rebleeding after endoscopic treatment of esophageal gastric varices rebleeding associated with liver cirrhosis [J]. The Journal of Practical Medicine, 2024, 40(22): 3155-3159. |
| [10] | Shijun LUO,Lizi ZHANG,Dunjin. CHEN. Diagnosis, prevention and treatment of placenta accreta spectrum with non⁃traumatic factors [J]. The Journal of Practical Medicine, 2024, 40(21): 2971-2975. |
| [11] | Lili TANG,Xueming LI,Liming LEI,Xiaodong ZENG,Yun LING,Qiongyu LIN,Sumin. ZHU. Risk factors for prolonged ICU stay after surgery in patients with infective endocarditis [J]. The Journal of Practical Medicine, 2024, 40(20): 2854-2859. |
| [12] | Xiaoqin LI,Lexin WANG,Xiaojun MA,Na LI,Guanjun LU,Zhihan ZHANG,Pengcheng. ZHANG. Mechanism of iron death induced by high homocysteine via TRPC6/NF⁃κb in glomerular podiatocytes [J]. The Journal of Practical Medicine, 2024, 40(2): 174-181. |
| [13] | Xianghong CHEN,Xiumin CHEN,Yingyan ZHOU,Li LI,Zhenxiong. XU. Advancements in the investigation of cardiovascular risk associated with idiopathic inflammatory myopathy [J]. The Journal of Practical Medicine, 2024, 40(19): 2801-2805. |
| [14] | Boyang YANG,Qian FANG,Yi ZHENG,Hongying. WANG. Quantitative diagnosis of annular pancreas in neonates with saline⁃contrast ultrasound [J]. The Journal of Practical Medicine, 2024, 40(18): 2618-2622. |
| [15] | Jun ZHENG,Qiye WU,Xia ZENG,Zhixian LEI,Dufei. ZHANG. Clinical characteristics and risk factors of the occurrence of hypoxic hepatitis in children with shock [J]. The Journal of Practical Medicine, 2024, 40(15): 2126-2132. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||