

The Journal of Practical Medicine ›› 2025, Vol. 41 ›› Issue (24): 3929-3940.doi: 10.3969/j.issn.1006-5725.2025.24.018
• Medical Examination and Clinical Diagnosis • Previous Articles
Tianyuan LI,Ying TIAN,Dingde LONG,Yang DONG,Huan. FU( )
)
Received:2025-10-16
Online:2025-12-25
Published:2025-12-25
Contact:
Huan. FU
E-mail:ndyfy06109@ncu.edu.cn
CLC Number:
Tianyuan LI,Ying TIAN,Dingde LONG,Yang DONG,Huan. FU. An interpretable machine learning model based on bedside lung and diaphragm ultrasound for preoperative prediction of pulmonary dysfunction in gastrointestinal tumor surgery: A clinical study[J]. The Journal of Practical Medicine, 2025, 41(24): 3929-3940.
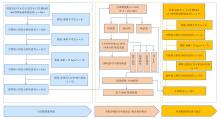
Fig.1
Flowchart of model development and validation"
Tab.1
Comparison of baseline characteristics and clinical variables among patients"
| 变量 | 总数(n = 424) | 肺功能 | χ2 /Z/t值 | P值 | |
|---|---|---|---|---|---|
| 正常(n = 268) | 异常(n = 156) | ||||
| 男性/[例(%)] | 224(52.830) | 135(50.373) | 89(57.051) | 1.765 | 0.184 |
| 吸烟史/[例(%)] | 134(31.604) | 82(30.597) | 52(33.333) | 0.342 | 0.559 |
| 饮酒史/[例(%)] | 114(26.887) | 64(23.881) | 50(32.051) | 3.349 | 0.067 |
| 癌症/[例(%)] | 76(17.925) | 42(15.672) | 34(21.795) | 2.513 | 0.113 |
| 糖尿病/[例(%)] | 42(9.906) | 23(8.582) | 19(12.179) | 1.430 | 0.232 |
| 高血压病/[例(%)] | 132(31.132) | 80(29.851) | 52(33.333) | 0.558 | 0.455 |
| 冠心病/[例(%)] | 20(4.717) | 11(4.104) | 9(5.769) | 0.608 | 0.436 |
| 心律失常/[例(%)] | 49(11.557) | 29(10.821) | 20(12.821) | 0.386 | 0.535 |
| COPD/[例(%)] | 38(8.962) | 19(7.090) | 19(12.179) | 3.131 | 0.077 |
| 中风病史/[例(%)] | 46(10.849) | 26(9.701) | 20(12.821) | 0.992 | 0.319 |
| 年龄/岁 | 65.000(57.000,71.000) | 64.000(55.000,69.000) | 67.000(60.000,73.000) | -4.439 | < 0.001? |
| BMI/(kg/m2) | 22.145(20.761,24.350) | 22.680(21.000,24.920) | 22.000(20.077,23.183) | 3.605 | < 0.001? |
| SpO2/% | 97.000(96.000,98.000) | 97.000(96.000,98.000) | 97.000(96.000,97.000) | 4.164 | < 0.001? |
| LUSs/分 | 2.000(1.000,4.000) | 1.000(1.000,3.000) | 4.000(2.000,7.000) | -8.407 | < 0.001? |
| Q-DE/cm | 2.040(1.880,2.230) | 2.130(1.980,2.240) | 1.890(1.750,2.110) | 7.454 | < 0.001? |
| D-DE/cm | 4.930(4.530,5.400) | 5.050(4.850,5.530) | 4.260(3.680,4.870) | 9.855 | < 0.001? |
| Q-DTF/% | 38.889(30.994,45.833) | 41.860(36.842,48.718) | 31.579(26.816,38.095) | 9.419 | < 0.001? |
| D-DTF/% | 62.393(41.667,75.510) | 71.795(60.870,81.081) | 39.831(35.135,51.515) | 12.103 | < 0.001? |
Tab.2
Comparison of baseline characteristics between the training and test sets"
| 变量 | 总数(n = 424) | 训练集(n = 268) | 测试集(n = 156) | χ2/Z/t值 | P值 |
|---|---|---|---|---|---|
| 男性/[例(%)] | 224(52.830) | 177(52.212) | 47(55.294) | 0.259 | 0.611 |
| 吸烟史/[例(%)] | 134(31.604) | 105(30.973) | 29(34.118) | 0.311 | 0.577 |
| 饮酒史/[例(%)] | 114(26.887) | 89(26.254) | 25(29.412) | 0.345 | 0.557 |
| 癌症/[例(%)] | 76(17.925) | 65(19.174) | 11(12.941) | 1.795 | 0.180 |
| 糖尿病/[例(%)] | 42(9.906) | 31(9.145) | 11(12.941) | 1.098 | 0.295 |
| 高血压病/[例(%)] | 132(31.132) | 98(28.909) | 34(40.000) | 3.899 | 0.048 |
| 冠心病/[例(%)] | 20(4.717) | 14(4.130) | 6(7.059) | 1.297 | 0.255 |
| 心律失常/[例(%)] | 49(11.557) | 41(12.094) | 8(9.412) | 0.478 | 0.489 |
| COPD/[例(%)] | 38(8.962) | 27(7.965) | 11(12.941) | 2.063 | 0.151 |
| 中风病史/[例(%)] | 46(10.849) | 36(10.619) | 10(11.765) | 0.092 | 0.761 |
| 年龄/岁 | 65.000(57.000,71.000) | 65.000(57.000,72.000) | 65.000(59.000,70.000) | 0.512 | 0.609 |
| BMI/(kg/m2) | 22.145(20.761,24.350) | 22.491(20.833,24.768) | 21.929(20.324,23.500) | 1.952 | 0.051 |
| SpO2/% | 97.000(96.000,98.000) | 97.000(96.000,98.000) | 97.000(96.000,98.000) | -1.620 | 0.092 |
| LUSs/分 | 2.000(1.000,4.000) | 2.000(1.000,5.000) | 2.000(1.000,3.000) | 1.723 | 0.081 |
| Q-DE/cm | 2.040(1.880,2.230) | 2.030(1.880,2.220) | 2.110(1.910,2.240) | -1.002 | 0.317 |
| D-DE/cm | 4.930(4.530,5.400) | 4.900(4.490,5.400) | 5.010(4.670,5.450) | -1.502 | 0.133 |
| Q-DTF(x ± s)/% | 38.715 ± 10.870 | 38.354 ± 10.932 | 40.156 ± 10.500 | -1.367 | 0.172 |
| D-DTF/% | 62.393(41.667,75.510) | 61.194(40.426,75.610) | 64.815(43.478,75.000) | -0.622 | 0.534 |

Fig.2
Results of predictor selection"


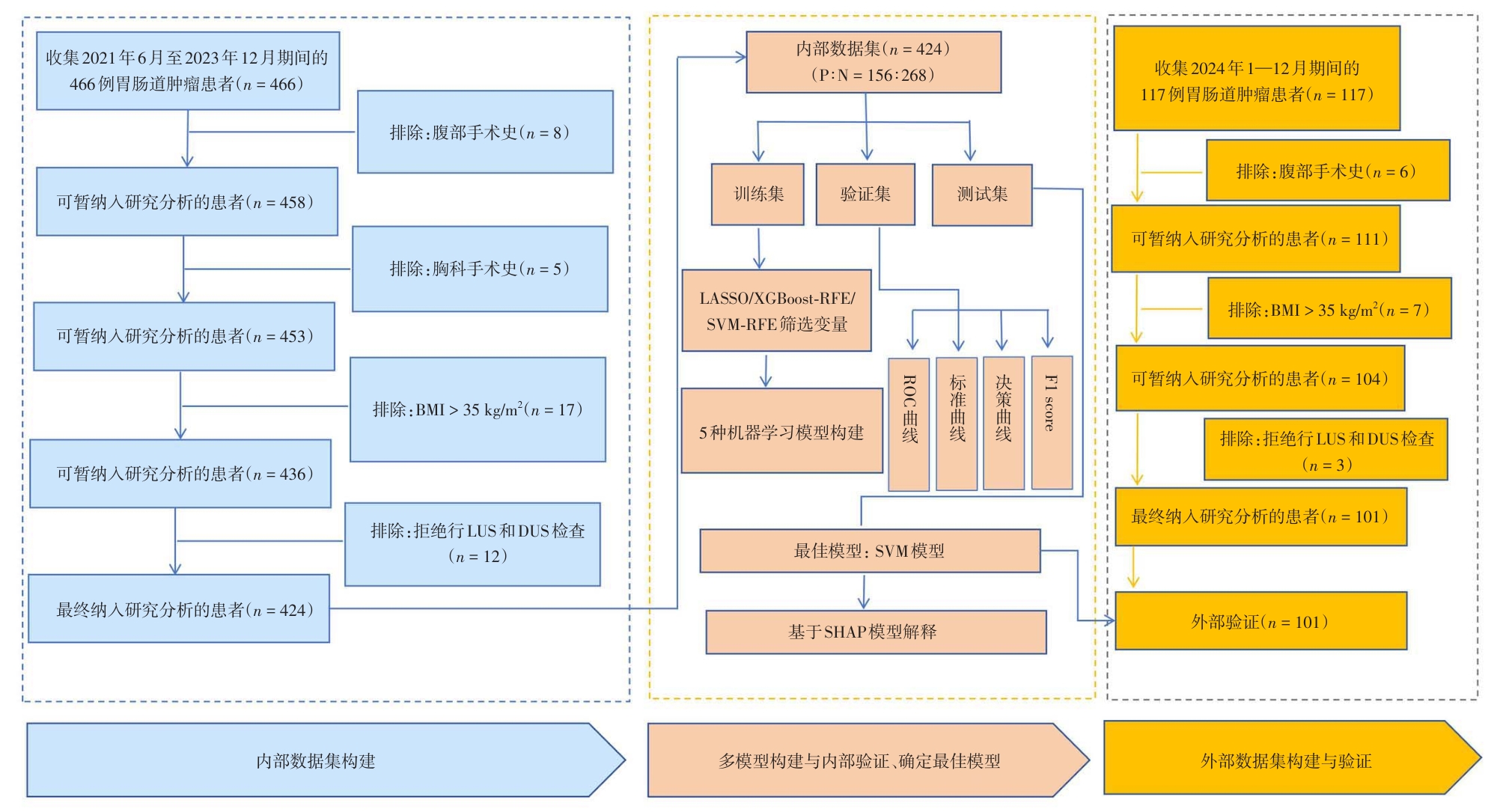
Fig.3
Comprehensive analysis of machine learning models"
Tab.3
Performance metrics of five machine learning models in the training set"
| 模型 | AUC(95%CI) | 敏感 | 特异 | PPV | NPV | F1 | |
|---|---|---|---|---|---|---|---|
| XGBoost | 0.999(0.997 ~ 1.000) | 0.974 | 0.998 | 0.959 | 0.94 | 0.999 | 0.968 |
| logistic | 0.857(0.809 ~ 0.906) | 0.827 | 0.780 | 0.859 | 0.783 | 0.856 | 0.781 |
| RandomForest | 0.997(0.994 ~ 1.000) | 0.967 | 0.981 | 0.957 | 0.938 | 0.988 | 0.959 |
| SVM | 0.878(0.833 ~ 0.923) | 0.840 | 0.785 | 0.876 | 0.806 | 0.862 | 0.795 |
| KNN | 0.922(0.892 ~ 0.951) | 0.831 | 0.866 | 0.809 | 0.750 | 0.904 | 0.802 |
Tab.4
Performance metrics of five machine learning models in the validation set"
| 模型 | AUC(95%CI) | 敏感 | 特异 | PPV | NPV | F1 | |
|---|---|---|---|---|---|---|---|
| XGBoost | 0.838(0.738 ~ 0.938) | 0.767 | 0.732 | 0.790 | 0.695 | 0.820 | 0.712 |
| logistic | 0.851(0.752 ~ 0.951) | 0.820 | 0.761 | 0.859 | 0.778 | 0.847 | 0.769 |
| RandomForest | 0.849(0.753 ~ 0.944) | 0.776 | 0.724 | 0.810 | 0.718 | 0.819 | 0.719 |
| SVM | 0.853(0.756 ~ 0.951) | 0.814 | 0.746 | 0.859 | 0.780 | 0.839 | 0.761 |
| KNN | 0.846(0.748 ~ 0.945) | 0.767 | 0.806 | 0.741 | 0.683 | 0.856 | 0.734 |
Fig.4
Training, validation, and testing of the SVM model"
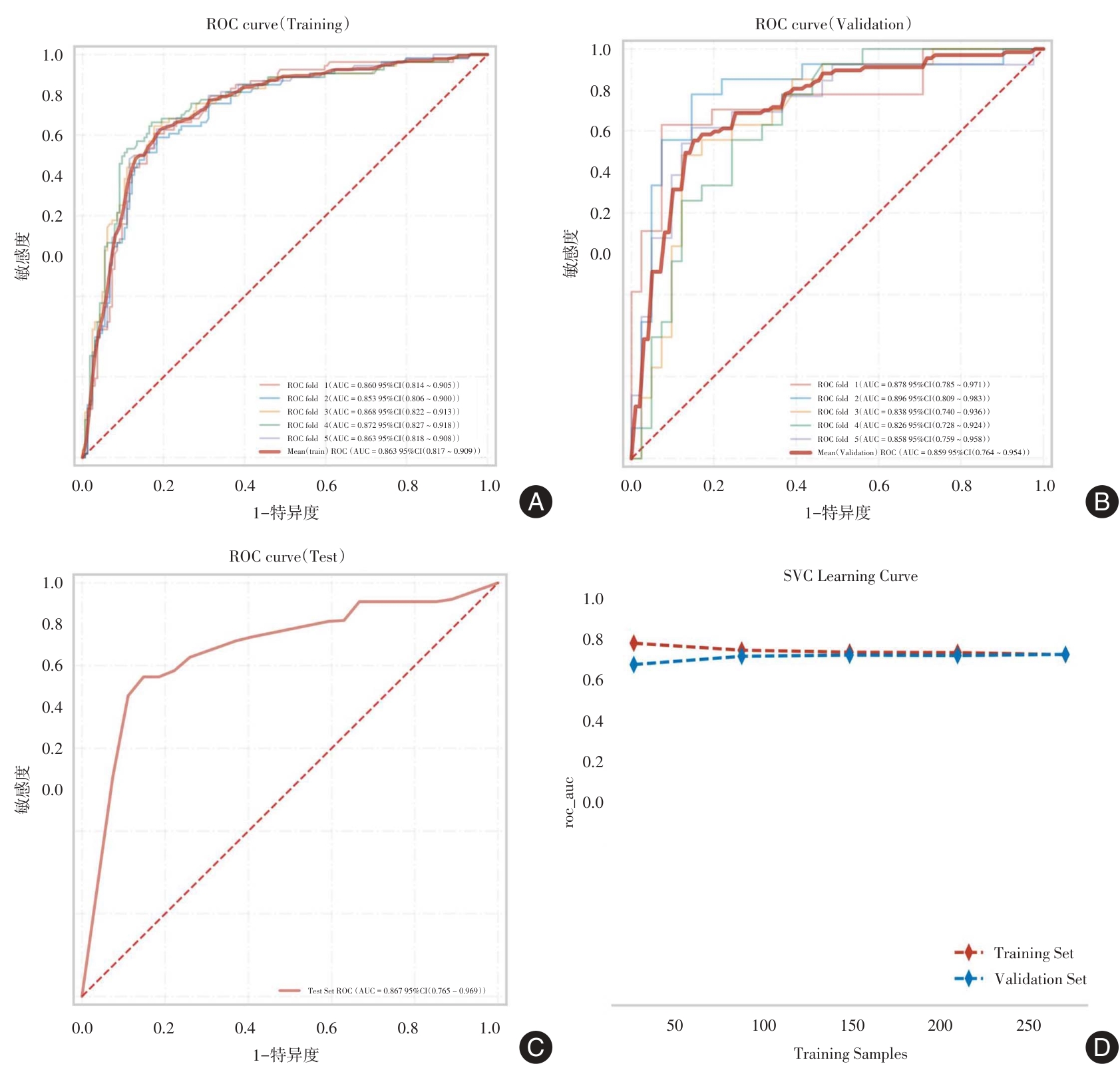
Fig.5
External validation of the final model"
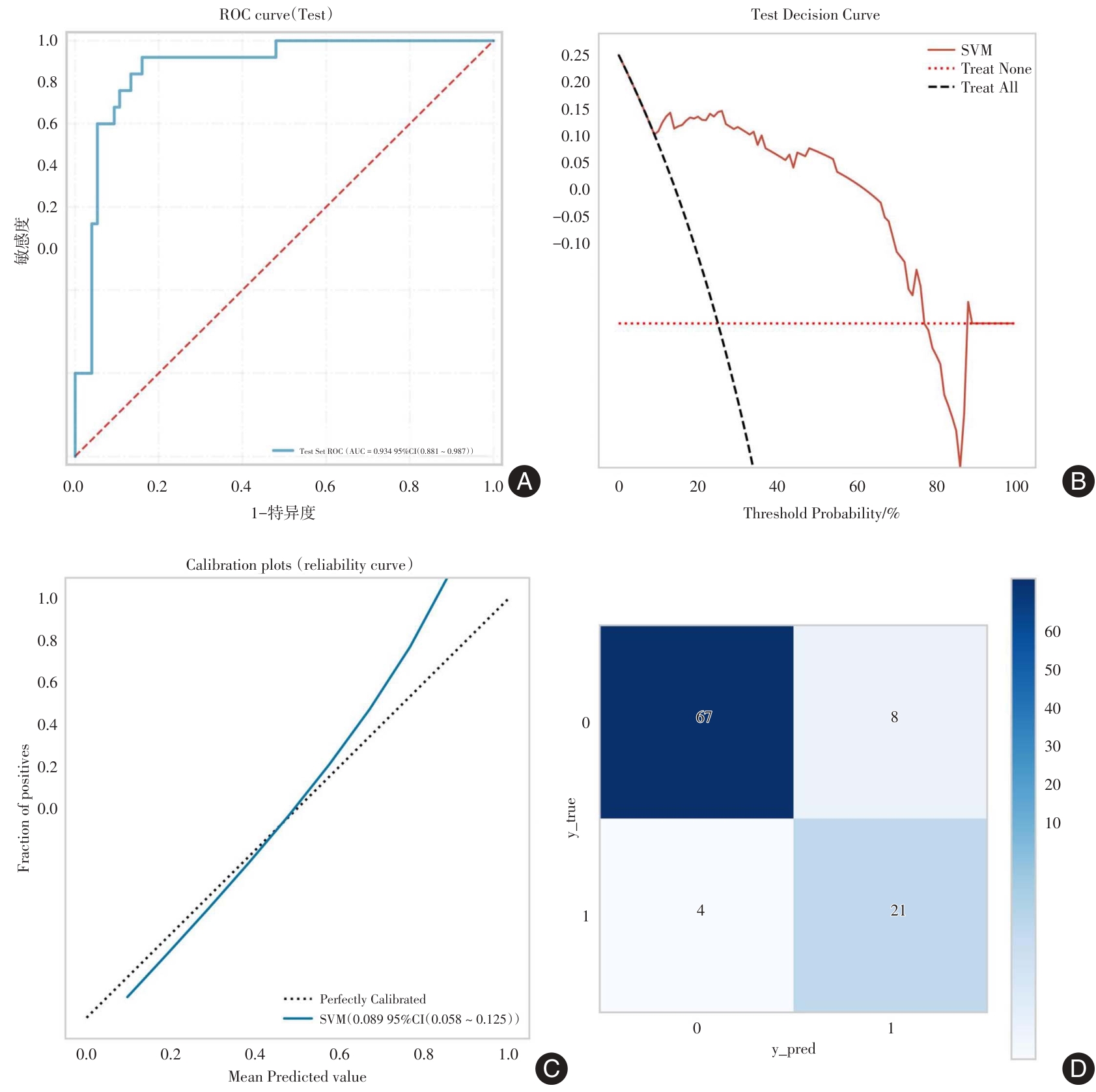

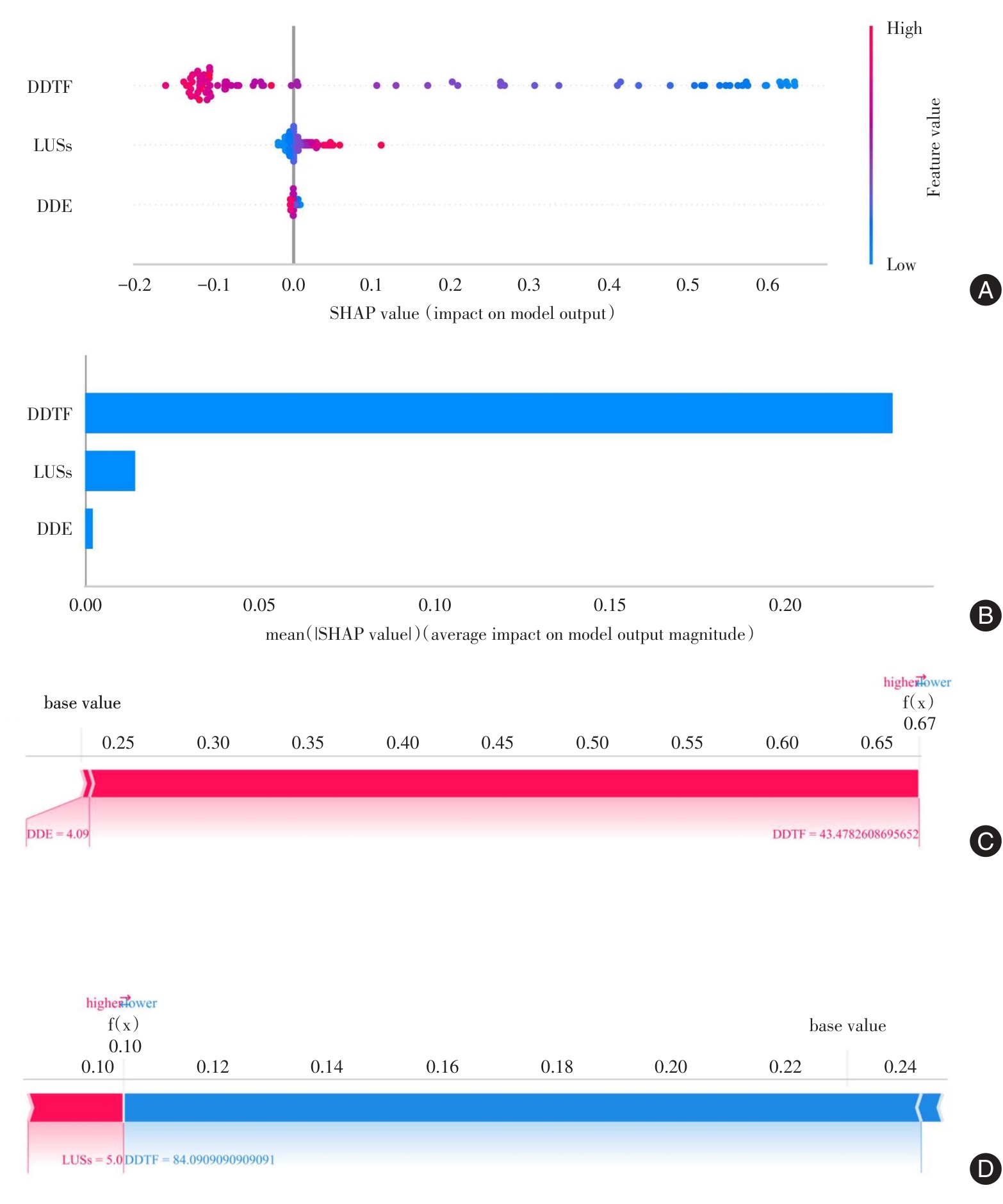
Fig.6
Model interpretability analysis based on SHAP"
| [1] |
MAO X, ZHANG W, NI Y Q, et al. A Prediction Model for Postoperative Pulmonary Complication in Pulmonary Function-Impaired Patients Following Lung Resection[J]. J Multidiscip Healthc, 2021, 14: 3187-3194. doi:10.2147/jmdh.s327285
doi: 10.2147/jmdh.s327285 |
| [2] | 郭高锋, 阮孝国, 王洋洋, 等. 床旁膈肌超声在预测胸腔镜肺叶切除术后肺部并发症中的应用价值[J]. 实用医学杂志, 2024, 40(2): 207-212. |
| [3] |
FERNANDEZ-BUSTAMANTE A, FRENDL G, SPRUNG J, et al. Postoperative Pulmonary Complications, Early Mortality, and Hospital Stay Following Noncardiothoracic Surgery: A Multicenter Study by the Perioperative Research Network Investigators[J]. JAMA Surg, 2017, 152(2): 157-166. doi:10.1001/jamasurg.2016.4065
doi: 10.1001/jamasurg.2016.4065 |
| [4] | 胡荣贵, 傅剑华, 罗孔嘉, 等. 术前放化疗对食管癌患者肺功能和术后肺部并发症的影响[J]. 中华胃肠外科杂志, 2013, 16(9): 827-830. |
| [5] |
SUNG H, FERLAY J, SIEGEL R L, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries[J]. CA Cancer J Clin, 2021, 71(3): 209-249. doi:10.3322/caac.21660
doi: 10.3322/caac.21660 |
| [6] |
DOHERTY C, KUBASKI F, TOMATSU S, et al. Non-invasive pulmonary function test on Morquio patients[J]. J Rare Dis Res Treat, 2017, 2(2): 55-62. doi:10.29245/2572-9411/2017/2.1097
doi: 10.29245/2572-9411/2017/2.1097 |
| [7] | KAWAMOTO H, KAMBE M. [Pulmonary function tests][J]. Rinsho Byori, 2003, 51(6): 568-573. |
| [8] |
BRUCK O, NAOFAL A, SENUSSI M H. Lung, Pleura, and Diaphragm Point-of-Care Ultrasound[J]. Semin Ultrasound CT MR, 2024, 45(1): 120-131. doi:10.1053/j.sult.2024.01.001
doi: 10.1053/j.sult.2024.01.001 |
| [9] |
TENZA-LOZANO E, LLAMAS-ALVAREZ A, JAIMEZ-NAVARRO E, et al. Lung and diaphragm ultrasound as predictors of success in weaning from mechanical ventilation[J]. Crit Ultrasound J, 2018, 10(1): 12. doi:10.1186/s13089-018-0094-3
doi: 10.1186/s13089-018-0094-3 |
| [10] |
LLAMAS-ÁLVAREZ A M, TENZA-LOZANO E M, LATOUR-PÉREZ J. Diaphragm and Lung Ultrasound to Predict Weaning Outcome: Systematic Review and Meta-Analysis[J]. Chest, 2017, 152(6): 1140-1150. doi:10.1016/j.chest.2017.08.028
doi: 10.1016/j.chest.2017.08.028 |
| [11] |
LI T, WU X Z, LONG D, et al. Ultrasonographic modeling of lung and diaphragm mechanics: Clinical trial of a novel non-invasive method to evaluate pre-operative pulmonary function[J]. PeerJ, 2024, 12: e18677. doi:10.7717/peerj.18677
doi: 10.7717/peerj.18677 |
| [12] | 中华医学会超声医学分会. 肺部超声临床应用专家共识[J]. 中华超声影像学杂志, 2022, 31(9): 757-768. |
| [13] |
DANISH M, AGARWAL A, GOYAL P, et al. Diagnostic Performance of 6-Point Lung Ultrasound in ICU Patients: A Comparison with Chest X-Ray and CT Thorax[J]. Turk J Anaesthesiol Reanim, 2019, 47(4): 307-319. doi:10.5152/tjar.2019.73603
doi: 10.5152/tjar.2019.73603 |
| [14] |
KONG S, WANG J, LI Y, et al. Value of Bedside Lung Ultrasound in Severe and Critical COVID-19 Pneumonia[J]. Respir Care, 2021, 66(6): 920-927. doi:10.4187/respcare.08382
doi: 10.4187/respcare.08382 |
| [15] |
ZAMBON M, GRECO M, BOCCHINO S, et al. Assessment of diaphragmatic dysfunction in the critically ill patient with ultrasound: A systematic review[J]. Intensive Care Med, 2017, 43(1): 29-38. doi:10.1007/s00134-016-4524-z
doi: 10.1007/s00134-016-4524-z |
| [16] |
MOINGEON P, KUENEMANN M, GUEDJ M. Artificial intelligence-enhanced drug design and development: Toward a computational precision medicine[J]. Drug Discov Today, 2022, 27(1): 215-222. doi:10.1016/j.drudis.2021.09.006
doi: 10.1016/j.drudis.2021.09.006 |
| [17] |
BIFARIN O O. Interpretable machine learning with tree-based shapley additive explanations: Application to metabolomics datasets for binary classification[J]. PLoS One, 2023, 18(5): e0284315. doi:10.1371/journal.pone.0284315
doi: 10.1371/journal.pone.0284315 |
| [18] |
GUO Z, WANG P, YE S, et al. Interpretable Machine Learning Models Based on Shapley Additive Explanations for Predicting the Risk of Cerebrospinal Fluid Leakage in Lumbar Fusion Surgery[J]. Spine (Phila Pa 1976), 2024, 49(18): 1281-1293. doi:10.1097/brs.0000000000005087
doi: 10.1097/brs.0000000000005087 |
| [19] |
ZARGARI MARANDI R. ExplaineR: An R package to explain machine learning models[J]. Bioinform Adv, 2024, 4(1): vbae049. doi:10.1093/bioadv/vbae049
doi: 10.1093/bioadv/vbae049 |
| [20] |
BRUSASCO V, CRAPO R, VIEGI G, et al. Coming together: The ATS/ERS consensus on clinical pulmonary function testing[J]. Eur Respir J, 2005, 26(1): 1-2. doi:10.1183/09031936.05.00034205
doi: 10.1183/09031936.05.00034205 |
| [21] |
BALL L, ROCCO P R M, PELOSI P. Editorial: Lung Imaging in Respiratory Failure[J]. Front Physiol, 2022, 13: 862647. doi:10.3389/fphys.2022.862647
doi: 10.3389/fphys.2022.862647 |
| [22] |
DESANTI R L, GILL K G, SWANSON J O, et al. Comparison of chest radiograph and lung ultrasound in children with acute respiratory failure[J]. J Ultrasound, 2023, 26(4): 861-870. doi:10.1007/s40477-023-00827-y
doi: 10.1007/s40477-023-00827-y |
| [23] | 路子蕴, 孙行, 徐璐, 等. 日间胸腔镜手术患者术后肺部并发症危险因素分析[J]. 实用医学杂志, 2023, 39(24): 3205-3209. |
| [24] |
QIAN Z, YANG M, LI L, et al. Ultrasound assessment of diaphragmatic dysfunction as a predictor of weaning outcome from mechanical ventilation: A systematic review and meta-analysis[J]. BMJ Open, 2018, 8(9): e021189. doi:10.1136/bmjopen-2017-021189
doi: 10.1136/bmjopen-2017-021189 |
| [25] |
XU Q, YANG X, QIAN Y, et al. Speckle tracking quantification parasternal intercostal muscle longitudinal strain to predict weaning outcomes: A multicentric observational study[J]. Shock, 2023, 59(1): 66-73. doi:10.1097/shk.0000000000002044
doi: 10.1097/shk.0000000000002044 |
| [26] |
PODDIGHE D, VAN HOLLEBEKE M, CHOUDHARY Y Q, et al. Accuracy of respiratory muscle assessments to predict weaning outcomes: A systematic review and comparative meta-analysis[J]. Crit Care, 2024, 28(1): 70. doi:10.1186/s13054-024-04823-4
doi: 10.1186/s13054-024-04823-4 |
| [27] |
STAHR C S, SAMARAGE C R, DONNELLEY M, et al. Quantification of heterogeneity in lung disease with image-based pulmonary function testing[J]. Sci Rep, 2016, 6: 29438. doi:10.1038/srep29438
doi: 10.1038/srep29438 |
| [28] |
STENWIG E, SALVI G, ROSSI P S, et al. Comparative analysis of explainable machine learning prediction models for hospital mortality[J]. BMC Med Res Methodol, 2022, 22(1): 53. doi:10.1186/s12874-022-01540-w
doi: 10.1186/s12874-022-01540-w |
| [29] |
ABBAS S, QAISAR A, FAROOQ M S, et al. Smart Vision Transparency: Efficient Ocular Disease Prediction Model Using Explainable Artificial Intelligence[J]. Sensors (Basel), 2024, 24(20): 6618. doi:10.3390/s24206618
doi: 10.3390/s24206618 |
| [30] |
BRANKOVIC A, HUANG W, COOK D, et al. Elucidating Discrepancy in Explanations of Predictive Models Developed Using EMR[J]. Stud Health Technol Inform, 2023, 310: 865-869. doi:10.3233/shti231088
doi: 10.3233/shti231088 |
| [1] | Xiudong YANG,Xing LIU,Xin LIU,Yan JIANG,Wei WANG,Zongbin HE,Sha HUANG,Meihong WEN,Yazhen. LIU. Construction and clinical validation of a machine learning⁃based nomogram model for predicting lymphatic leakage following radical prostatectomy [J]. The Journal of Practical Medicine, 2025, 41(21): 3378-3384. |
| [2] | Cuicui WANG,Wantong QIAO,Junying YAO,Qian LI,Weige GAO,Min FAN. Clinical application value of nutritional control status score combined with prognostic nutritional index in evaluating the risk of anemia in elderly colorectal cancer patients [J]. The Journal of Practical Medicine, 2025, 41(17): 2696-2704. |
| [3] | Jianliang YAN,Zeyu XIE,Rongrong JING,Ming. CUI. Research on establishing gastric cancer lymph node metastasis prediction model based on machine learning and routine laboratory indicators [J]. The Journal of Practical Medicine, 2024, 40(6): 844-849. |
| [4] | Liangjiang HUANG,Dewen MAO,Jinghui ZHENG,Minggang WANG,Chun YAO. Application of artificial intelligence in HE risk prediction modelling and research advances [J]. The Journal of Practical Medicine, 2024, 40(3): 289-294. |
| [5] |
YAN Jianliang, JING Rongrong, XIE Zeyu, CUI Ming..
Applicationprogress of machine learning in mining of gastric cancer biomarker [J]. The Journal of Practical Medicine, 2023, 39(6): 783-787. |
| [6] |
SUN Fang, XU Yongbo, CUI Guanghe, LI Xinyan, DONG Jingyun, JIAO Yuting, TANG Liwei. .
Predict the Luminal type of invasive breast cancer using machine learning models based on ultrasono⁃ graphic features [J]. The Journal of Practical Medicine, 2022, 38(18): 2279-2283. |
| [7] |
YAN Junhong, DUAN Shuhui, HUAN Mei⁃ yu, PAN Lei..
Recent advances of lung ultrasound in coronavirus disease 2019 [J]. The Journal of Practical Medicine, 2021, 37(17): 2171-2175. |
| [8] |
HUANG Zhongjiang, JIANG Zengyu, LI Jianding, ZHANG Zhixing, CHEN Wenqing.
Application of enhanced CT radiomics in differentiation of renal angiomyolipoma without visible fat from homogeneous clear cell renal cell carcinoma [J]. The Journal of Practical Medicine, 2021, 37(17): 2266-2270. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||