

The Journal of Practical Medicine ›› 2025, Vol. 41 ›› Issue (13): 2039-2044.doi: 10.3969/j.issn.1006-5725.2025.13.014
• Clinical Research • Previous Articles
Yu LU1,Zhaolian BIAN2( )
)
Received:2025-03-31
Online:2025-07-10
Published:2025-07-18
Contact:
Zhaolian BIAN
E-mail:bianzhaolian1998@163.com
CLC Number:
Yu LU,Zhaolian BIAN. Application of liver⁃to⁃spleen volume ratio combined with fibrinogen in evaluating prognosis of liver cirrhosis patients with esophagogastric variceal bleeding[J]. The Journal of Practical Medicine, 2025, 41(13): 2039-2044.
Tab.1
Comparison of baseline characteristics between non-bleeding and re-bleeding EGVB patients"
| 项目 | 未出血组(n = 71) | 再出血组(n = 59) | χ2/t/Z值 | P值 |
|---|---|---|---|---|
| 年龄(x ± s)/岁 | 58.73 ± 9.92 | 59.80 ± 11.64 | -0.563 | 0.574 |
| 性别/例 | 0.058 | 0.809 | ||
| 男 | 34 | 27 | ||
| 女 | 37 | 32 | ||
| 病因/[例(%)] | 7.76 | 0.051 | ||
| 乙型肝炎 | 45(63.4) | 23(39.0) | ||
| 酒精性肝炎 | 5(7.0) | 6(10.2) | ||
| 自身免疫性肝炎 | 12(16.9) | 17(28.8) | ||
| 其他 | 9(12.7) | 13(22.0) | ||
| ALT/(U/L) | 23(19,37) | 28(22,40) | -1.841 | 0.066 |
| AST/(U/L) | 32(26,44) | 43(32,56) | -3.113 | 0.002 |
| TBIL/(μmol/L) | 20.3(14.3,31.5) | 26.4(16.5,34.0) | -1.700 | 0.089 |
| ALB(x ± s)/(g/L) | 31.91 ± 6.03 | 30.07 ± 4.58 | 1.923 | 0.057 |
| RBC(x ± s)/(× 109/L) | 2.72 ± 0.69 | 2.53 ± 0.65 | 1.566 | 0.120 |
| Hb(x ± s)/(g/L) | 75.37 ± 20.67 | 73.19 ± 19.66 | 0.612 | 0.542 |
| PLT/(109/L) | 54(42,82) | 65(45,95) | -1.464 | 0.143 |
| PT/s | 15.6(13.7,17.5) | 15.3(14.3,17.7) | -0.051 | 0.959 |
| INR | 1.34(1.19,1.50) | 1.33(1.23,1.52) | -0.257 | 0.797 |
| FIB/(g/L) | 1.70(1.23,1.96) | 1.18(0.97,1.52) | -3.587 | 0.000 |
| D-二聚体/(mg/L) | 1.02(0.59,1.95) | 1.42(0.77,3.60) | -2.104 | 0.035 |
| Cr/(μmol/L) | 64.6(54.2,74.0) | 62.0(52.0,83.0) | -0.187 | 0.852 |
| BUN/(mmol/L) | 8.40(6.17,11.17) | 7.81(5.39,11.13) | -0.676 | 0.499 |
| MELD(x ± s) | 7.58 ± 3.64 | 9.32 ± 4.63 | -2.397 | 0.018 |
| CTP | 7.00(7.00,8.00) | 8.00(7.00,9.00) | -1.623 | 0.104 |
| ALBI(x ± s) | -1.84 ± 0.51 | -1.63 ± 0.46 | -2.385 | 0.019 |
| 门静脉血栓/[例(%)] | 21(29.6) | 11(18.6) | 2.076 | 0.150 |
| 门静脉直径(x ± s)/mm | 15.47 ± 1.96 | 14.43 ± 2.02 | 0.218 | 0.004 |
| 脾静脉直径(x ± s)/mm | 11.44 ± 2.43 | 10.40 ± 2.31 | 0.073 | 0.015 |
| LV/cm3 | 960.4(794.6,1 163.8) | 1 021.8(860.5,1 220.6) | -1.34 | 0.180 |
| SV/cm3 | 873.1(659.90,1 146.4) | 578.5(451.4,895.2) | -4.150 | 0.000 |
| LSVR | 1.08(0.90,1.45) | 1.61(1.33,2.62) | -4.524 | 0.000 |
Tab.2
Multivariate logistic analysis of prognostic factors for 1-year outcomes in EGVB patients"
| 变量 | β | SE | P值 | OR | 95% CI |
|---|---|---|---|---|---|
| LSVR | 1.208 | 0.369 | 0.001 | 3.347 | 1.624~6.899 |
| AST | 0.015 | 0.010 | 0.119 | 1.015 | 0.996~1.034 |
| D-二聚体 | 0.147 | 0.117 | 0.209 | 1.158 | 0.921~1.456 |
| FIB | -1.578 | 0.495 | 0.001 | 0.206 | 0.078~0.544 |
| MELD | 0.065 | 0.061 | 0.287 | 1.067 | 0.947~1.203 |
| ALBI | -0.662 | 0.549 | 0.228 | 0.516 | 0.176~1.512 |
| 门静脉直径 | -0.246 | 0.162 | 0.129 | 0.782 | 0.569~1.074 |
| 脾静脉直径 | -0.035 | 0.138 | 0.802 | 0.966 | 0.738~1.265 |
Tab.3
Prognostic value of LSVR, FIB and their combination in EGVB patients"
| 变量 | AUC | 敏感度 | 特异度 | 约登指数 | 截断值 | P值 | 95% CI |
|---|---|---|---|---|---|---|---|
| LSVR联合FIB | 0.825 | 0.746 | 0.817 | 0.563 | -2.741 | 0.000 | 0.751 ~ 0.899 |
| LSVR | 0.731 | 0.763 | 0.718 | 0.481 | 1.320 | 0.000 | 0.639 ~ 0.822 |
| FIB | 0.683 | 0.577 | 0.797 | 0.374 | 1.575 | 0.000 | 0.589 ~ 0.777 |
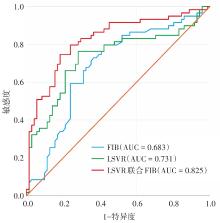
Fig.1
ROC analysis of LSVR, FIB and their combination for EGVB prognosis"
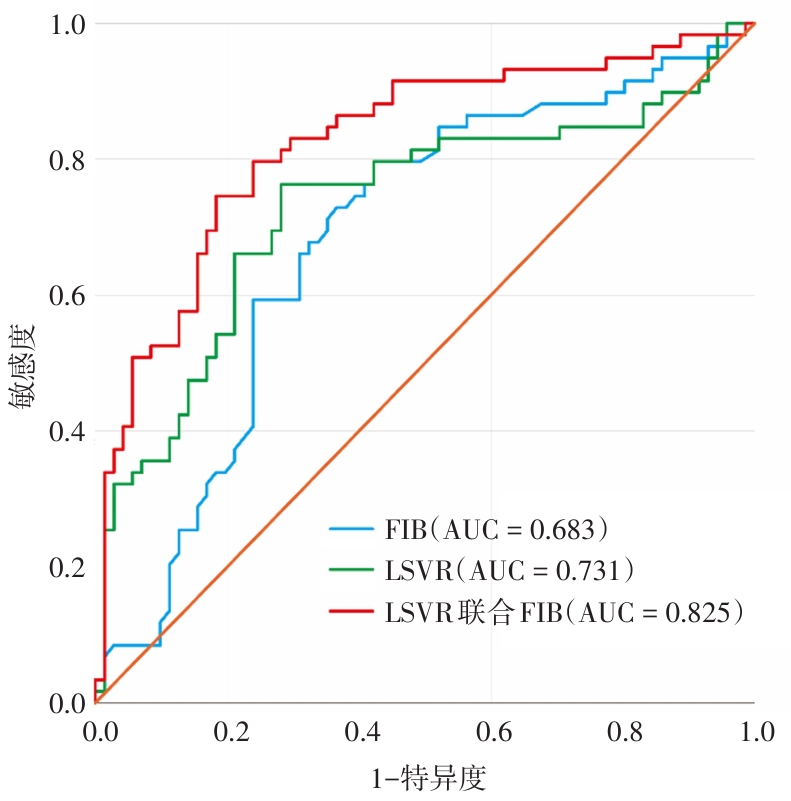
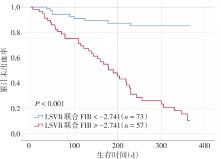
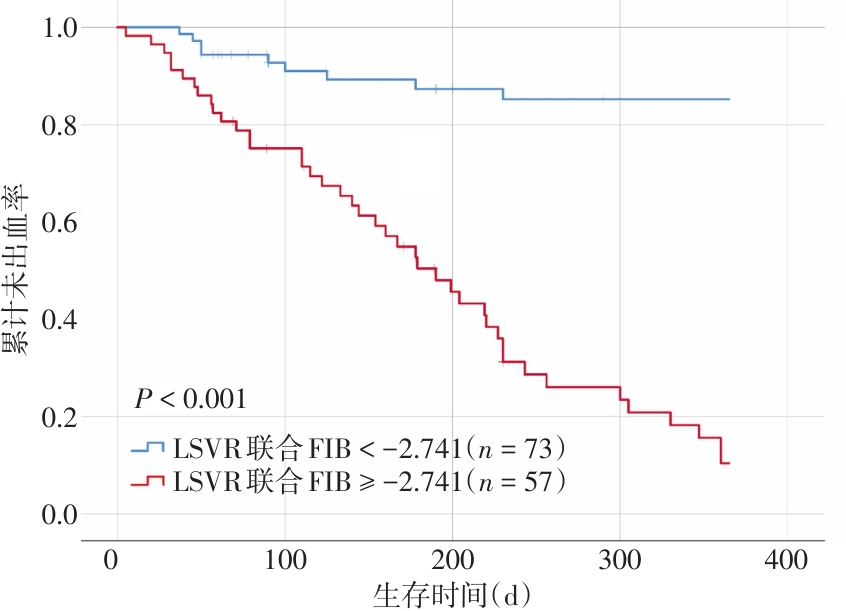
Fig.2
Survival analysis of EGVB patients stratified by LSVR combined with FIB"
| [1] | DE FRANCHIS R, BOSCH J, GARCIA-TSAO G, et al. Baveno VII - Renewing consensus in portal hypertension [J]. J Hepatol, 2022, 76(4): 959-974. |
| [2] |
YOKOYAMA S, HONDA T, ISHIZU Y, et al. Predicting early rebleeding and mortality after endoscopic hemostasis of esophagogastric varices: Diagnostic performance of aspartate aminotransferase-to-platelet ratio index and model for end-stage liver disease-Na score [J]. J Hepatobiliary Pancreat Sci, 2024, 31(11): 830-839. doi:10.1002/jhbp.12057
doi: 10.1002/jhbp.12057 |
| [3] |
ZENG A, LI Y, LYU L, et al. Risk factors and predictive nomograms for bedside emergency endoscopic treatment following endotracheal intubation in cirrhotic patients with esophagogastric variceal bleeding [J]. Sci Rep, 2024, 14(1): 9467. doi:10.1038/s41598-024-59802-0
doi: 10.1038/s41598-024-59802-0 |
| [4] |
KUTAIBA N, CHUNG W, GOODWIN M, et al. The impact of hepatic and splenic volumetric assessment in imaging for chronic liver disease: A narrative review [J]. Insights Imaging, 2024, 15(1): 146. doi:10.1186/s13244-024-01727-3
doi: 10.1186/s13244-024-01727-3 |
| [5] |
SON J H, LEE S S, LEE Y, et al. Assessment of liver fibrosis severity using computed tomography-Based liver and spleen volumetric indices in patients with chronic liver disease [J]. Eur Radiol, 2020, 30(6): 3486-3496. doi:10.1007/s00330-020-06665-4
doi: 10.1007/s00330-020-06665-4 |
| [6] |
KWON J H, LEE S S, YOON J S, et al. Liver-to-Spleen Volume Ratio Automatically Measured on CT Predicts Decompensation in Patients with B Viral Compensated Cirrhosis [J]. Korean J Radiol, 2021, 22(12): 1985-1995. doi:10.3348/kjr.2021.0348
doi: 10.3348/kjr.2021.0348 |
| [7] |
SINGH T, HASAN M, GAULE T G, et al. Exploiting the Molecular Properties of Fibrinogen to Control Bleeding Following Vascular Injury [J]. Int J Mol Sci, 2025, 26(3):1336. doi:10.3390/ijms26031336
doi: 10.3390/ijms26031336 |
| [8] |
BROWN R S, JR., BROWN K A, FLAMM S, et al. Screening and management of portal hypertension and varices in cirrhosis: Expert perspectives [J]. Hepatol Commun, 2025, 9(4):e0682. doi:10.1097/hc9.0000000000000682
doi: 10.1097/hc9.0000000000000682 |
| [9] |
XU X, DING H, JIA J, et al. Chinese guidelines on the management of ascites in cirrhosis : Chinese Society of Hepatology, Chinese Medical Association [J]. Hepatol Int, 2024, 18(4): 1071-1089. doi:10.1007/s12072-024-10697-z
doi: 10.1007/s12072-024-10697-z |
| [10] |
JOBE K, HENRY Z. Endoscopic Treatment of Acute Esophageal and Gastric Variceal Bleeding [J]. Gastrointest Endosc Clin N Am, 2024, 34(2): 249-261. doi:10.1016/j.giec.2023.09.004
doi: 10.1016/j.giec.2023.09.004 |
| [11] |
LI X, CUI Y, GAO S, et al. Development and validation of a score model for predicting the risk of first esophagogastric variceal hemorrhage and mortality in patients with hepatocellular carcinoma [J]. Ann Med, 2025, 57(1): 2490210. doi:10.1080/07853890.2025.2490210
doi: 10.1080/07853890.2025.2490210 |
| [12] | 王慧群, 叶超, 许朝, 等. 肝硬化食管胃底静脉曲张破裂出血内镜治疗后再出血的5年随访研究 [J]. 实用医学杂志, 2024, 40(22): 3155-3159. |
| [13] |
CATUCCI D, HRYCYK J, LANGE N F, et al. Liver segmental volumes and their relationship with 5-year prognostication [J]. Abdom Radiol (NY), 2025, 50(3): 1133-1142. doi:10.1007/s00261-024-04552-w
doi: 10.1007/s00261-024-04552-w |
| [14] | 薛红, 张莉, 陈伟杰, 等. 肝体积联合血小板在评估慢加急性肝衰竭预后中的应用 [J]. 实用医学杂志, 2023, 39(10): 1247-1252. |
| [15] | 漆丹. 彩超对于酒精性肝硬化与肝炎肝硬化的鉴别诊断价值研究 [J]. 中国实用医药, 2020, 15(34): 35-37. |
| [16] | 符玉环, 贺文, 王克扬. 64排螺旋CT对原发性胆汁性肝硬化患者肝脏体积变化的研究——与乙肝肝硬化和正常人对比研究 [J]. 临床放射学杂志, 2016, 35(10): 1517-1520. |
| [17] |
YU S, CHEN W, JIANG Z. Platelet count/spleen volume ratio has a good predictive value for esophageal varices in patients with hepatitis B liver cirrhosis [J]. PLoS One, 2021, 16(12): e0260774. doi:10.1371/journal.pone.0260774
doi: 10.1371/journal.pone.0260774 |
| [18] |
TAN B-G, TANG Z, OU J, et al. A novel model based on liver/spleen volumes and portal vein diameter on MRI to predict variceal bleeding in HBV cirrhosis [J]. Eur Radiol, 2022, 33(2): 1378-1387. doi:10.1007/s00330-022-09107-5
doi: 10.1007/s00330-022-09107-5 |
| [19] |
MURATA Y, ABE M, HIASA Y, et al. Liver/spleen volume ratio as a predictor of prognosis in primary biliary cirrhosis [J]. J Gastroenterol, 2008, 43(8): 632-636. doi:10.1007/s00535-008-2202-9
doi: 10.1007/s00535-008-2202-9 |
| [20] |
TIDWELL J, THAKKAR B, WU G Y. Etiologies of Splenic Venous Hypertension: A Review [J]. J Clin Transl Hepatol, 2024, 12(6): 594-606. doi:10.14218/jcth.2024.00054
doi: 10.14218/jcth.2024.00054 |
| [21] | RIZZO K, VELLA K, ZAMMIT D, et al. Fibrinogen measurement in liver disease: Validation of the functional fibrinogen thromboelastography assay and a novel mathematical predictive model [J]. Blood Transfus, 2019, 17(3): 237-246. |
| [22] |
DESBOROUGH M J, KAHAN B C, STANWORTH S J, et al. Fibrinogen as an independent predictor of mortality in decompensated cirrhosis and bleeding [J]. Hepatology, 2017, 65(3): 1079-1080. doi:10.1002/hep.28915
doi: 10.1002/hep.28915 |
| [1] | Li ZHOU,Yong HAN,Ting PANG,Jingheng LEI,Shan ZENG,Jingjing WANG,Yuejie ZHOU,Shuya LI,Zhe DENG. Predictive value of plasma fibrinogen for in⁃hospital mortality in patients with septic shock [J]. The Journal of Practical Medicine, 2025, 41(12): 1840-1845. |
| [2] |
XIE Yongzheng, SUN Xinfang, SUN Juncong, WANG Zhaoyang, ZHENG Li, SHI Zhaohui..
Therapeutic efficacy of different surgical methods on esophageal and gastric variceal hemorrhage in liver cirrhosis [J]. The Journal of Practical Medicine, 2023, 39(7): 860-865. |
| [3] | Jie ZHANG,Fanliang. MENG. Diagnostic and Prognostic Value of HDAC4 and Fibrinogen/Albumin Ratio in Non⁃small Cell Lung Cancer [J]. The Journal of Practical Medicine, 2023, 39(19): 2495-2500. |
| [4] | bater Hurile,Hongli WU,Xueting LIU,Zhipeng LI,Zhipeng YANG,Hongjun WANG,Qi XIN,Hongwei. CHEN. Predictors of early left ventricular thrombus in elderly patients with anterior acute ST segment elevation myocardial infarction receiving emergency percutaneous coronary intervention [J]. The Journal of Practical Medicine, 2023, 39(17): 2230-2235. |
| [5] | ZHANG Xiaodan, LIANG Ping, LIANG Jing, WANG Hongbo, SU Jiangwei. . Effects of Bacillus Subtilis and Enterococcus Faecium Enteric ⁃coated Capsules on intestinal barrier func⁃ tion and expression of Th9 cells in liver cirrhosis patients with different hepatic reserve function [J]. The Journal of Practical Medicine, 2023, 39(14): 1820-1824. |
| [6] | XUE Hong, ZHANG Li, CHEN Weijie, CHEN Ying, SHAO Jianguo, BIAN Zhaolian. . Study on the prognosis of chronic acute hepatic failure patients based on the prediction model of liver vol⁃ ume and platelet [J]. The Journal of Practical Medicine, 2023, 39(10): 1247-1252. |
| [7] | LI Xiaoling, ZHOU Wenjie, DENG Wei, MA Xigang.. Prognostic value of coagulation function index combined with serum cystatin C in patients with septic acute kidney injury [J]. The Journal of Practical Medicine, 2023, 39(1): 81-85. |
| [8] |
QIN Xiang, ZHANG Jiandong, KONG Dan, GUO Lili..
The value of residual liver volume in evaluation of liver reserve function on liver mass CT virtual imaging [J]. The Journal of Practical Medicine, 2022, 38(22): 2845-2849. |
| [9] |
Guixin, GUAN Shuhong, ZHOU Jun..
Value of endocan and fibrinogen in the diagnosis and disease course assessment of AECOPD PENG [J]. The Journal of Practical Medicine, 2022, 38(17): 2198-2202. |
| [10] |
HAO Xingliang, WANG Yingying, ZHANG Jian, LI Shuang, WANG Naizhi, JI Yanrong..
Establishment and study of risk model for predicting prognosis of COPD patients in acute exacerbation stage by combining clinical characteristics,MMP⁃12,FIB and CC⁃16 [J]. The Journal of Practical Medicine, 2021, 37(4): 458-462. |
| [11] |
BUY REMUGU· Abu Dureyimu, FANG Fa , MU Qingshuang , SUN Jun..
The effect of regulation of intestinal microflora on the peritonitis therapeutic effect nd prognosis of elderly patients with liver cirrhosis
[J]. The Journal of Practical Medicine, 2021, 37(3): 343-347.
|
| [12] |
ZHANG Meng, LIU Jiao, CHEN Yi, LI Yesheng, HUANG Yangqing.
A randomized controlled trial of tolvaptan in the treatment of cirrhotic ascites during the perioperative pe⁃ riod [J]. The Journal of Practical Medicine, 2021, 37(16): 2137-2141. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||