

The Journal of Practical Medicine ›› 2025, Vol. 41 ›› Issue (10): 1445-1452.doi: 10.3969/j.issn.1006-5725.2025.10.003
• Feature Reports:Hepatocellular Carcinoma • Previous Articles
Yanhao SUN1,Yi ZHOU2,Yilong. HU3( )
)
Received:2025-01-21
Online:2025-05-25
Published:2025-05-21
Contact:
Yilong. HU
E-mail:yiminhyl@163.com
CLC Number:
Yanhao SUN,Yi ZHOU,Yilong. HU. The predictive value of rectus abdominis area and visceral fat distribution for the risk of surgical site infection after open radical surgery for hepatocellular carcinoma[J]. The Journal of Practical Medicine, 2025, 41(10): 1445-1452.
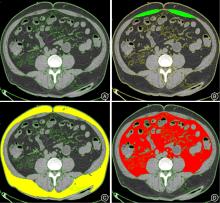
Fig.1
SFA, RAA, and VFA measurements"
Tab.1
Comparison of clinical baseline characteristics between the SSI and non-SSI groups"
| 项目 | 整体队列 (n = 263) | 倾向评分匹配队列 (n = 118) | ||||||
|---|---|---|---|---|---|---|---|---|
| SSI(n = 66) | 非-SSI(n = 197) | t/χ2值 | P值 | SSI(n = 59) | 非-SSI(n = 59) | t/χ2 值 | P值 | |
| 女性 | 30(45.5) | 82(41.6) | 0.29 | 0.59 | 23(40) | 26(44.1) | 0.17 | 0.68 |
| 年龄(x ± s)/岁 | 70.1 ± 4.3 | 58.9 ± 10.5 | 7.89 | 0.033 | 66.4 ± 8.7 | 63.6 ± 5.6 | 1.43 | 0.16 |
| BMI(x ± s)/(kg/m2) | 27.1 ± 4.2 | 22.4 ± 2.6 | 8.12 | 0.024 | 25.5 ± 5.3 | 22.6 ± 5.4 | 1.52 | 0.43 |
| 吸烟 | 24(36.4) | 28(14.2) | 8.73 | 0.003 | 9(15.3) | 7(11.9) | 0.34 | 0.78 |
| 合并症 | 9.45 | 0.026 | 2.53 | 0.47 | ||||
| 肺部炎症 | 16(24.2) | 36(18.3) | 14(23.7) | 16(27.1) | ||||
| 高血压 | 33(50.0) | 79(40.1) | 25(42.4) | 22(37.3) | ||||
| 2型糖尿病 | 11(16.7) | 56(28.4) | 12(20.3) | 15(25.4) | ||||
| 其他 | 6(9.1) | 26(13.2) | 8(13.6) | 6(10.2) | ||||
| ASA评分 | 6.53 | 0.038 | 1.16 | 0.56 | ||||
| Ⅰ | 14(21.2) | 50(25.4) | 14(23.7) | 16(27.1) | ||||
| Ⅱ | 35(53.0) | 128(65.0) | 36(61.0) | 38(64.4) | ||||
| Ⅲ | 17(25.8) | 19(9.6) | 9(15.3) | 5(8.5) | ||||
| Child-Pugh分级 | 10.87 | 0.001 | 1.49 | 0.48 | ||||
| A级 | 39(59.1) | 93(47.2) | 33(55.9) | 32(54.2) | ||||
| B级 | 18(27.3) | 69(35.0) | 19(32.2) | 21(35.6) | ||||
| C级 | 9(13.6) | 35(17.8) | 7(11.9) | 6(10.2) | ||||
Tab.2
Comparison of preoperative and intraoperative indicators between the SSI and non-SSI groups"
| 项目 | SSI (n = 59) | 非SSI (n = 59) | t/χ2 值 | P值 |
|---|---|---|---|---|
| 白细胞计数/(×109/L) | 7.3 ± 1.3 | 6.9 ± 1.2 | 0.98 | 0.33 |
| C 反应蛋白/(mg/L) | 14.6 ± 2.4 | 12.4 ± 1.5 | 1.85 | 0.07 |
| 降钙素原/(ng/mL) | 0.28 ± 0.01 | 0.22 ± 0.2 | 1.45 | 0.15 |
| 白蛋白/(g/L) | 30.6 ± 2.6 | 36.4 ± 3.4 | 3.12 | 0.003 |
| 血红蛋白/(g/L) | 124 ± 13.2 | 126 ± 14.2 | 1.15 | 0.25 |
| 失血量/mL | 157 ± 25.2 | 136 ± 16.3 | 0.65 | 0.52 |
| 手术时长/min | 195 ± 23.1 | 204 ± 18.3 | 1.25 | 0.21 |
| 手术方式/[例(%)] | 7.18 | 0.06 | ||
| 左外叶切除 | 6(10.2) | 9(15.3) | ||
| 左半肝切除 | 36(61.0) | 31(52.5) | ||
| 右半肝切除 | 13(22.0) | 16(27.1) | ||
| 其他术式 | 4(6.8) | 3(5.1) | ||
| 淋巴结清扫数量 | 22.4 ± 2.5 | 29.2 ± 3.2 | 1.02 | 0.32 |
Tab.3
Comparison of abdominal anatomical characteristics between the SSI and non-SSI groups"
| 参数 | SSI(n = 59) | 非SSI(n = 59) | t值 | P值 |
|---|---|---|---|---|
| SFA/cm2 | 606.52 ± 25.43 | 583.42 ± 43.23 | 1.18 | 0.241 |
| RAA/cm2 | 52.34 ± 5.31 | 34.33 ± 9.33 | 2.18 | 0.032 |
| VFA/cm2 | 952.41 ± 74.48 | 724.76 ± 67.72 | 2.47 | 0.015 |
| V/S 比值 | 1.57 ± 1.31 | 1.04 ± 0.83 | 3.14 | 0.002 |
Tab.4
Univariate and multivariate logistic regression analysis of surgical site infection risk factors"
| 参数 | 单因素logistic回归 | 多因素logistic回归 | ||
|---|---|---|---|---|
| OR(95%CI) | P值 | OR(95%CI) | P值 | |
| 性别 | ||||
| 年龄 | 1.12(0.98 ~ 1.28) | 0.089 | ||
| BMI | 1.34(0.92 ~ 1.95) | 0.124 | ||
| 吸烟(是) | 1.67(1.02 ~ 2.73) | 0.041 | 1.21(0.87 ~ 1.69) | 0.253 |
| Child-Pugh分级 | 1.53(1.11 ~ 2.11) | 0.009 | 1.18(0.94 ~ 1.48) | 0.157 |
| ASA评分 | 2.01(0.92 ~ 3.06) | 0.217 | ||
| 术前白细胞计数 | ||||
| 术前白蛋白 | 2.14(1.45 ~ 3.16) | 0.003 | 1.103(0.903 ~ 1.302) | 0.063 |
| 术前血红蛋白 | 1.78(1.20 ~ 2.64) | 0.107 | ||
| 手术时长 | 2.53(0.91 ~ 3.63) | 0.083 | ||
| 失血量 | 2.312(0.34 ~ 3.54) | 0.265 | ||
| 皮下脂肪面积 | 1.64(0.88 ~ 2.45) | 0.531 | ||
| RAA | 1.32(1.01 ~ 1.72) | 0.033 | 1.285(1.043 ~ 1.472) | 0.013 |
| VFA | 1.54(1.14 ~ 1.83) | 0.009 | 1.041(1.001 ~ 1.232) | 0.029 |
| V/S比值 | 1.38(1.17 ~ 1.93) | 0.024 | 1.304(1.065 ~ 1.503) | 0.002 |
Tab.5
Prediction of surgical site infection"
| 参数 | 灵敏度/% | 特异度/% | 截断值 | AUC | P值 |
|---|---|---|---|---|---|
| RAA | 88 | 93.76 | 46.54 cm2 | 0.77 | 0.042 |
| VFA | 79 | 79.75 | 856.42 cm2 | 0.64 | 0.035 |
| V/S 比值 | 90 | 100.00 | 1.25 | 0.88 | 0.021 |
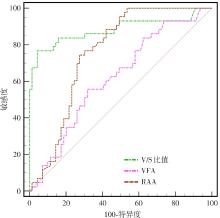
Fig.2
ROC analysis of risk factors for SSI prediction"

Fig.3
Nomogram for surgical incision infection in open radical surgery for liver cancer"
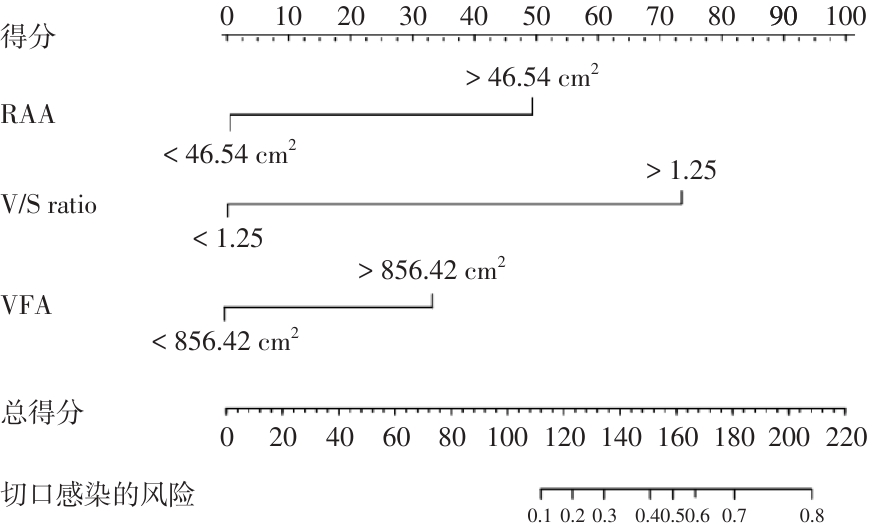
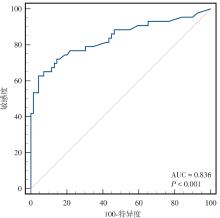
Fig.4
ROC analysis of the nomogram for surgical incision infection"
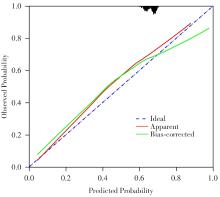
Fig.5
Calibration curve of the nomogram for surgical incision infection"
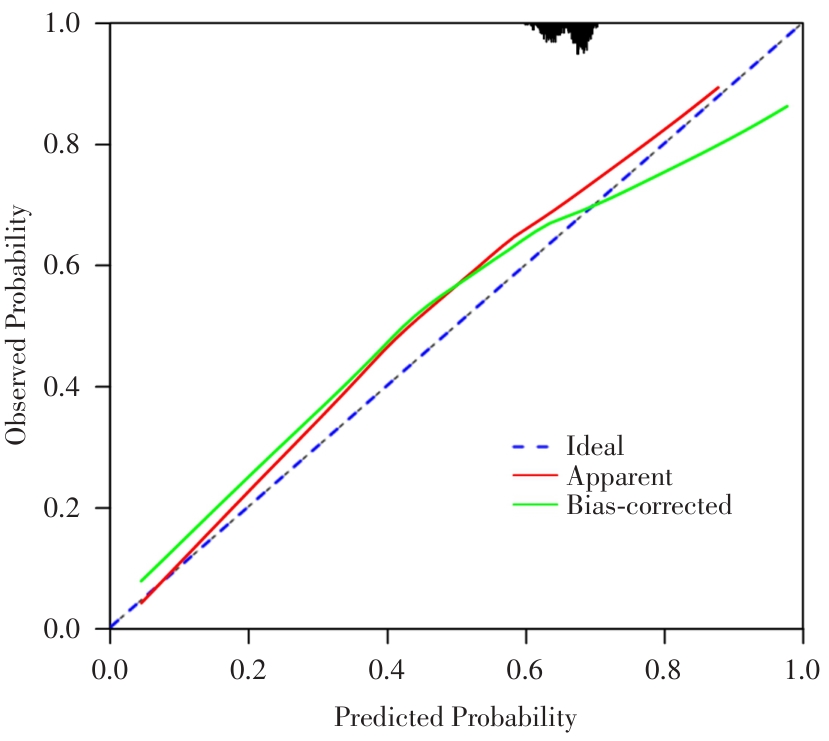
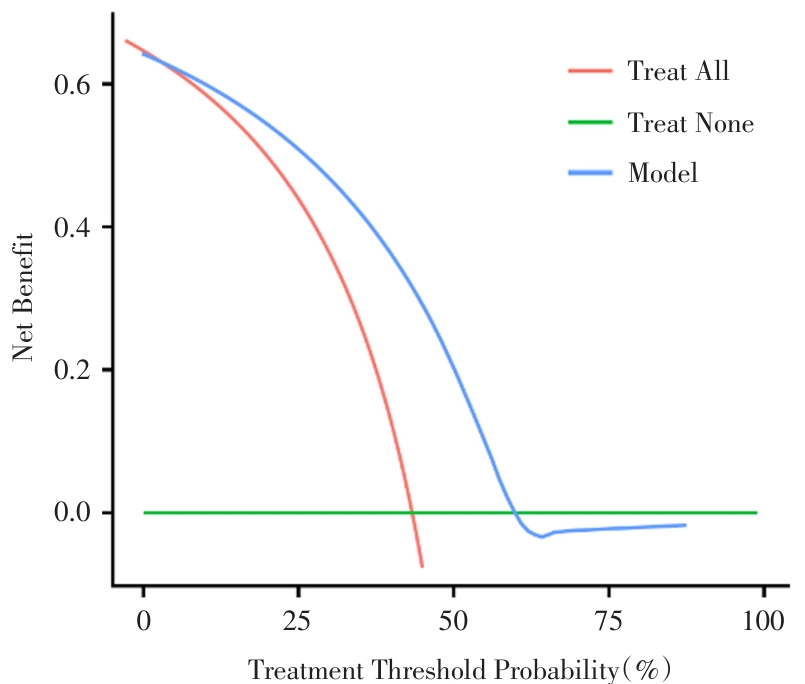
Fig.6
Decision curve of the nomogram for surgical incision infection"
| 1 |
SEIDELMAN J L, MANTYH C R, ANDERSON D J. Surgical Site Infection Prevention: A Review[J]. JAMA,2023,329 (3):244-252. doi:10.1001/jama.2022.24075
doi: 10.1001/jama.2022.24075 |
| 2 | 林鹏,蔡敏清,房俊伟,等. 肝癌术后复发的外科治疗研究现状及进展[J]. 器官移植,2022,13(1):111-119. |
| 3 |
MCFARLAND A M, MANOUKIAN S, MASON H, et al. Impact of surgical-site infection on health utility values: A meta-analysis[J]. Br J Surg, 2023,110 (8):942-949. doi:10.1093/bjs/znad144
doi: 10.1093/bjs/znad144 |
| 4 |
KAIBORI M, ICHIHARA N, MIYATA H, et al. Surgical outcomes of laparoscopic versus open repeat liver resection for liver cancers: A report from a nationwide surgical database in Japan[J]. J Hepatobiliary Pancreat Sci, 2022,29 (8):833-842. doi:10.1002/jhbp.1156
doi: 10.1002/jhbp.1156 |
| 5 | 刘为军, 陈昌贤, 张丽菊,等. 结直肠癌患者体质量指数及临床特征与远期预后的相关性[J]. 实用医学杂志, 2021, 37(13): 1701-1705. |
| 6 | 陈会文,马兴越,刘锦裕,等. 内脏脂肪面积对结直肠癌患者围手术期相关指标及短期预后的影响[J]. 重庆医学,2024,53(9):1312-1316,1322. |
| 7 | 中华人民共和国国家卫生健康委员会. 原发性肝癌诊疗指南(2024年版)[J]. 临床肝胆病杂志,2024,40(5):893-918. |
| 8 |
ALLEGRANZI B, BISCHOFF P, DE JONGE S, et al. New WHO recommendations on preoperative measures for surgical site infection prevention: An evidence-based global perspective[J]. Lancet Infect Dis, 2016,16(12):e276-e287. doi:10.1016/s1473-3099(16)30398-x
doi: 10.1016/s1473-3099(16)30398-x |
| 9 | YOSHIZUMI T, NAKAMURA T, YAMANE M, et al. Abdominal fat: Standardized technique for measurement at CT[J]. Radiology,1991,211(1):283-286. |
| 10 |
SHUSTER A, PATLAS M N, PINTHUS J H, et al. The clinical importance of visceral adiposity: A critical review of methods for visceral adipose tissue analysis[J]. Br J Radiol,2012,85(1009):1-10. doi:10.1259/bjr/38447238
doi: 10.1259/bjr/38447238 |
| 11 |
SOUZA N C, GONZALEZ M C, MARTUCCI R B, et al. Comparative Analysis Between Computed Tomography and Surrogate Methods to Detect Low Muscle Mass Among Colorectal Cancer Patients[J]. JPEN J Parenter Enteral Nutr, 2020,44(7):1328-1337. doi:10.1002/jpen.1741
doi: 10.1002/jpen.1741 |
| 12 | 吕进,吕成余,徐牧,等. 腹腔镜直肠癌手术后发生腹直肌萎缩的影响因素分析及预测模型构建[J]. 腹腔镜外科杂志,2024,29(2):103-107. |
| 13 |
YUKSEL O, GEZER N S, CANDA A E, et al. Cross-sectional areas of rectus abdominis and psoas muscles reduces following surgery in rectal cancer patients[J]. Support Care Cancer, 2020,28(5):2397-2405. doi:10.1007/s00520-019-05062-y
doi: 10.1007/s00520-019-05062-y |
| 14 | SIMPSON E, HAHNE A. Effectiveness of Early Postpartum Rectus Abdominis versus Transversus Abdominis Training in Patients with Diastasis of the Rectus Abdominis Muscles: A Pilot Randomized Controlled Trial[J]. Physiother Can,2023,75(4):368-376. |
| 15 |
LIU S, WANG M, LU X, et al. Abdomen Depth and Rectus Abdominis Thickness Predict Surgical Site Infection in Patients Receiving Elective Radical Resections of Colon Cancer[J]. Front Oncol,2019,9:637. doi:10.3389/fonc.2019.00637
doi: 10.3389/fonc.2019.00637 |
| 16 | 李岳航,王愿,李义帅,等. 内脏脂肪在肺癌中的研究进展[J]. 实用医学杂志, 2022, 38(10): 1292-1297. |
| 17 | 马于祺,万浩浩,毕心然,等. CT定量测定内脏脂肪对胃癌根治术后并发症和预后的影响[J]. 中国现代普通外科进展,2024,27(11):882-886. |
| 18 |
TANIGUCHI Y, KUROKAWA Y, TAKAHASHI T, et al. Impacts of Preoperative Psoas Muscle Mass and Visceral Fat Area on Postoperative Short- and Long-Term Outcomes in Patients with Gastric Cancer[J]. World J Surg, 2021,45(3):815-821. doi:10.1007/s00268-020-05857-9
doi: 10.1007/s00268-020-05857-9 |
| 19 |
HOU T Y, GAN H Q, ZHOU J F, et al. Incidence of and risk factors for surgical site infection after colorectal surgery: A multiple-center prospective study of 3,663 consecutive patients in China[J]. Int J Infect Dis, 2020,96:676-681. doi:10.1016/j.ijid.2020.05.124
doi: 10.1016/j.ijid.2020.05.124 |
| 20 |
WATANABE J, TATSUMI K, OTA M, et al. The impact of visceral obesity on surgical outcomes of laparoscopic surgery for colon cancer[J]. Int J Colorectal Dis, 2014,29(3):343-351. doi:10.1007/s00384-013-1803-9
doi: 10.1007/s00384-013-1803-9 |
| 21 |
TAKEUCHI M, ISHII K, SEKI H, et al. Excessive visceral fat area as a risk factor for early postoperative complications of total gastrectomy for gastric cancer: A retrospective cohort study[J]. BMC Surg, 2016,16(1):54. doi:10.1186/s12893-016-0168-8
doi: 10.1186/s12893-016-0168-8 |
| 22 |
BOCCA G, MASTORIDIS S, YEUNG T M, et al. Visceral-to-subcutaneous fat ratio exhibits strongest association with early post-operative outcomes in patients undergoing surgery for advanced rectal cancer[J]. Int J Colorectal Dis, 2022,37(8):1893-1900. doi:10.1007/s00384-022-04221-8
doi: 10.1007/s00384-022-04221-8 |
| 23 | TIAN W L, XU X, ZHAO R S, et al. High visceral fat-to-muscle ratio predicated a recurrent fistula after definitive surgery for a small intestinal fistula with diffuse extensive abdominal adhesions: A cohort study[J]. Int J Surg, 2023,109(11):3490-3496. |
| 24 |
BUCKLEY E, MULLEN M M, NIZAMUDDIN R, et al. High visceral fat to subcutaneous fat ratios portend a poor prognosis in patients with advanced endometrial cancer[J]. Gynecol Oncol, 2022,167(3):496-501. doi:10.1016/j.ygyno.2022.09.011
doi: 10.1016/j.ygyno.2022.09.011 |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||