

The Journal of Practical Medicine ›› 2026, Vol. 42 ›› Issue (1): 1-11.doi: 10.3969/j.issn.1006-5725.2026.01.001
• Oncology: Diagnosis, Treatment and Prevention •
Bo DENG1,Caoxia PENG1,Qilian XIONG2,Weiqi NIAN1,Ying LIU1( )
)
Received:2025-08-03
Online:2026-01-10
Published:2026-01-14
Contact:
Ying LIU
E-mail:liuying_19_82@163.com
CLC Number:
Bo DENG,Caoxia PENG,Qilian XIONG,Weiqi NIAN,Ying LIU. Predictive model for unplanned 30-day readmission in stage Ⅲ—Ⅳ lung cancer patients receiving immune checkpoint inhibitors[J]. The Journal of Practical Medicine, 2026, 42(1): 1-11.
Tab.1
Comparison of baseline characteristics between training set and validation set"
| 变量 | 验证集(n = 84) | 训练集(n = 200) | t/Z/χ2值 | P值 |
|---|---|---|---|---|
| 年龄(x ± s)/岁 | 65.39 ± 9.78 | 64.75 ± 10.41 | 0.47 | 0.63 |
| 住院天数[M(P25,P75)]/d | 5.00(3.00, 9.00) | 5.00(3.00, 10.00) | 0.03 | 0.98 |
| 性别 | 0.37 | 0.54 | ||
| 女 | 27(32.1) | 57(28.5) | ||
| 男 | 57(67.9) | 143(71.5) | ||
| 吸烟 | 0.14 | 0.71 | ||
| 无 | 32(38.1) | 81(40.5) | ||
| 有 | 52(61.9) | 119(59.5) | ||
| 饮酒 | 3.21 | 0.07 | ||
| 无 | 42(50.0) | 123(61.5) | ||
| 有 | 42(50.0) | 77(38.5) | ||
| 介入治疗 | 0.005 | 0.95 | ||
| 无 | 70(83.3) | 166(83.0) | ||
| 有 | 14(16.7) | 34(17.0) | ||
| 远端转移 | 0.30 | 0.58 | ||
| 无 | 21(25.0) | 44(22.0) | ||
| 有 | 63(75.0) | 156(78.0) | ||
| TNM | 0.05 | 0.82 | ||
| Ⅲ期 | 22(26.2) | 55(27.5) | ||
| Ⅳ期 | 62(73.8) | 145(72.5) | ||
| KPS | 0.09 | 0.76 | ||
| < 70分 | 20(23.8) | 51(25.5) | ||
| ≥ 70分 | 64(76.2) | 149(74.5) | ||
| NRS 2002 | 0.80 | 0.37 | ||
| < 3分 | 65(77.4) | 164(82.0) | ||
| ≥ 3分 | 19(22.6) | 36(18.0) | ||
| TCMD | 1.79 | 0.18 | ||
| 虚证 | 71(84.5) | 155(77.5) | ||
| 实证 | 13(15.5) | 45(22.5) | ||
| RBC | 0.04 | 0.83 | ||
| 低 | 28(33.3) | 64(32.0) | ||
| 正常 | 56(66.7) | 136(68.0) | ||
| Hb | 0.09 | 0.76 | ||
| 低 | 28(33.3) | 63(31.5) | ||
| 正常 | 56(66.7) | 137(68.5) | ||
| WBC | 0.37 | 0.83 | ||
| < 3.5 × 109/L | 65(77.4) | 148(74.0) | ||
| 3.5 ~ 9.5 × 109/L | 12(14.3) | 32(16.0) | ||
| ≥ 9.5 × 109/L | 7(8.3) | 20(10.0) | ||
| NEUT | 2.88 | 0.24 | ||
| < 1.8 × 109/L | 60(71.4) | 149(74.5) | ||
| 1.8 ~ 6.3 × 109/L | 11(13.1) | 14(7.0) | ||
| ≥ 6.3 × 109/L | 13(15.5) | 37(18.5) | ||
| PLT | 0.48 | 0.79 | ||
| < 125 × 109/L | 54(64.3) | 136(68.0) | ||
| 125 ~ 350 × 109/L | 24(28.6) | 53(26.5) | ||
| ≥ 350 × 109/L | 6(7.1) | 11(5.5) | ||
| CRP | 2.57 | 0.11 | ||
| ≤ 10 mg/L | 44(52.4) | 84(42.0) | ||
| > 10 mg/L | 40(47.6) | 116(58.0) | ||
| ALB | 0.40 | 0.53 | ||
| < 40 g/L | 31(36.9) | 66(33.0) | ||
| 40 ~ 55 g/L | 53(63.1) | 134(67.0) | ||
| AFP | 2.11 | 0.15 | ||
| 0 ~ 7 mg/L | 71(84.5) | 181(90.5) | ||
| > 7 mg/L | 13(15.5) | 19(9.5) | ||
| CEA | 0.58 | 0.44 | ||
| 0 ~ 5 mg/L | 51(60.7) | 131(65.5) | ||
| > 5 mg/L | 33(39.3) | 69(34.5) | ||
| CA19-9 | 0.03 | 0.86 | ||
| 0 ~ 37 U/mL | 63(75.0) | 148(74.0) | ||
| > 37 U/mL | 21(25.0) | 52(26.0) | ||
| CA50 | 0.26 | 0.61 | ||
| 0 ~ 25 U/mL | 65(77.4) | 149(74.5) | ||
| > 25 U/mL | 19(22.6) | 51(25.5) |

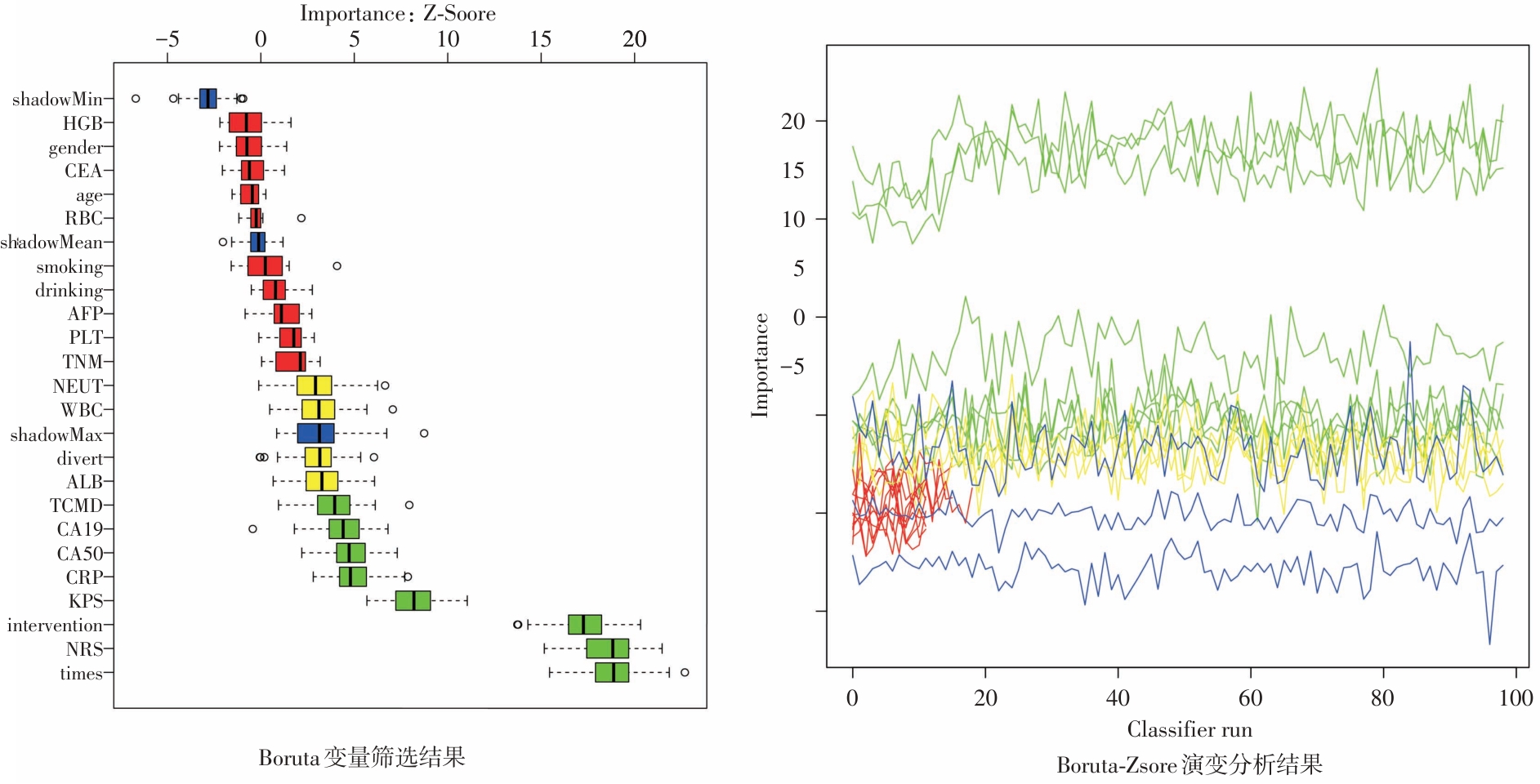
Fig.1
Feature selection results for unplanned readmission using the Boruta algorithm"
Tab.2
Results of univariate and multivariate logistic regression analysis after Boruta screening"
| 变量 | 单因素分析 | 多因素分析 | |||
|---|---|---|---|---|---|
| OR(95%CI) | P值 | OR(95%CI) | P值 | ||
| 住院天数 | 1.115(1.06 ~ 1.169) | < 0.01 | 1.11(1.03 ~ 1.19) | < 0.01 | |
| 介入治疗 | |||||
| 否 | Ref | Ref | |||
| 是 | 5.26(2.41 ~ 11.47) | < 0.01 | 11.34(3.51 ~ 36.63) | < 0.01 | |
| CRP | |||||
| ≤ 10 mg/L | Ref | Ref | |||
| > 10 mg/L | 2.91(1.48 ~ 5.71) | < 0.01 | 1.46(0.60 ~ 3.56) | 0.4 | |
| CA19-9 | |||||
| 0 ~ 37 U/mL | Ref | Ref | |||
| > 37 U/mL | 2.379(1.23 ~ 4.61) | 0.01 | 0.65(0.17 ~ 2.49) | 0.53 | |
| CA50 | |||||
| 0 ~ 25 U/mL | Ref | Ref | |||
| > 25 U/mL | 2.79(1.43 ~ 5.43) | 0.003 | 1.61(0.43 ~ 5.96) | 0.47 | |
| KPS | |||||
| < 70分 | Ref | Ref | |||
| ≥ 70分 | 0.18(0.089 ~ 0.35) | < 0.01 | 0.22(0.08 ~ 0.58) | < 0.01 | |
| NRS 2002 | |||||
| < 3分 | Ref | Ref | |||
| ≥ 3分 | 11.90(5.11 ~ 27.74) | < 0.01 | 8.86(3.06 ~ 25.62) | < 0.01 | |
| TCMD | |||||
| 虚证 | Ref | Ref | |||
| 实证 | 0.81(0.39 ~ 1.71) | 0.58 | 0.92(0.43 ~ 1.81) | 0.62 | |

Fig.2
Comprehensive evaluation of the logistic regression model for predicting unplanned readmission"
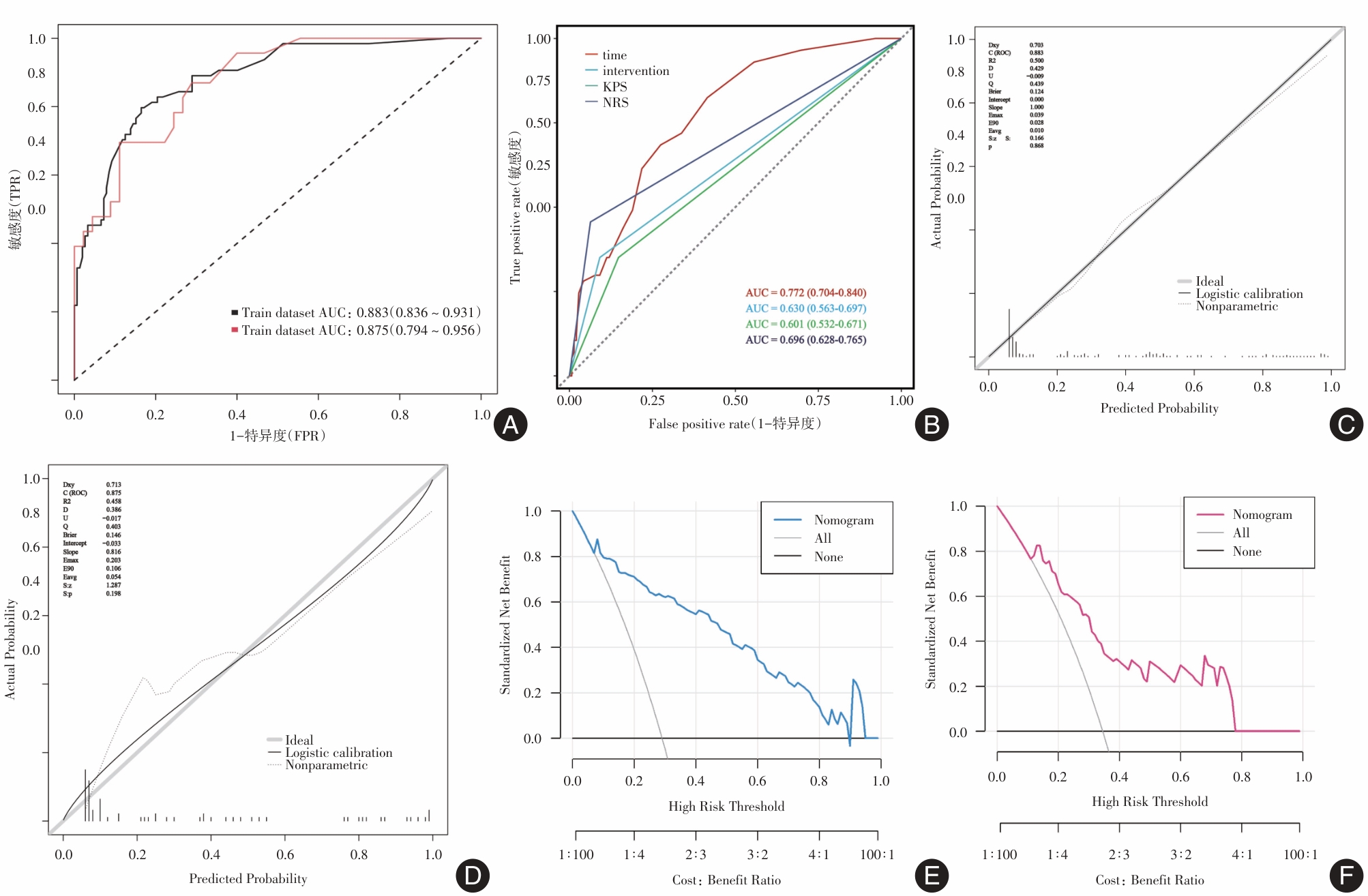

Fig.3
Nomogram for unplanned readmission in patients with stage Ⅲ—Ⅳ lung cancer treated with immune checkpoint inhibitors"
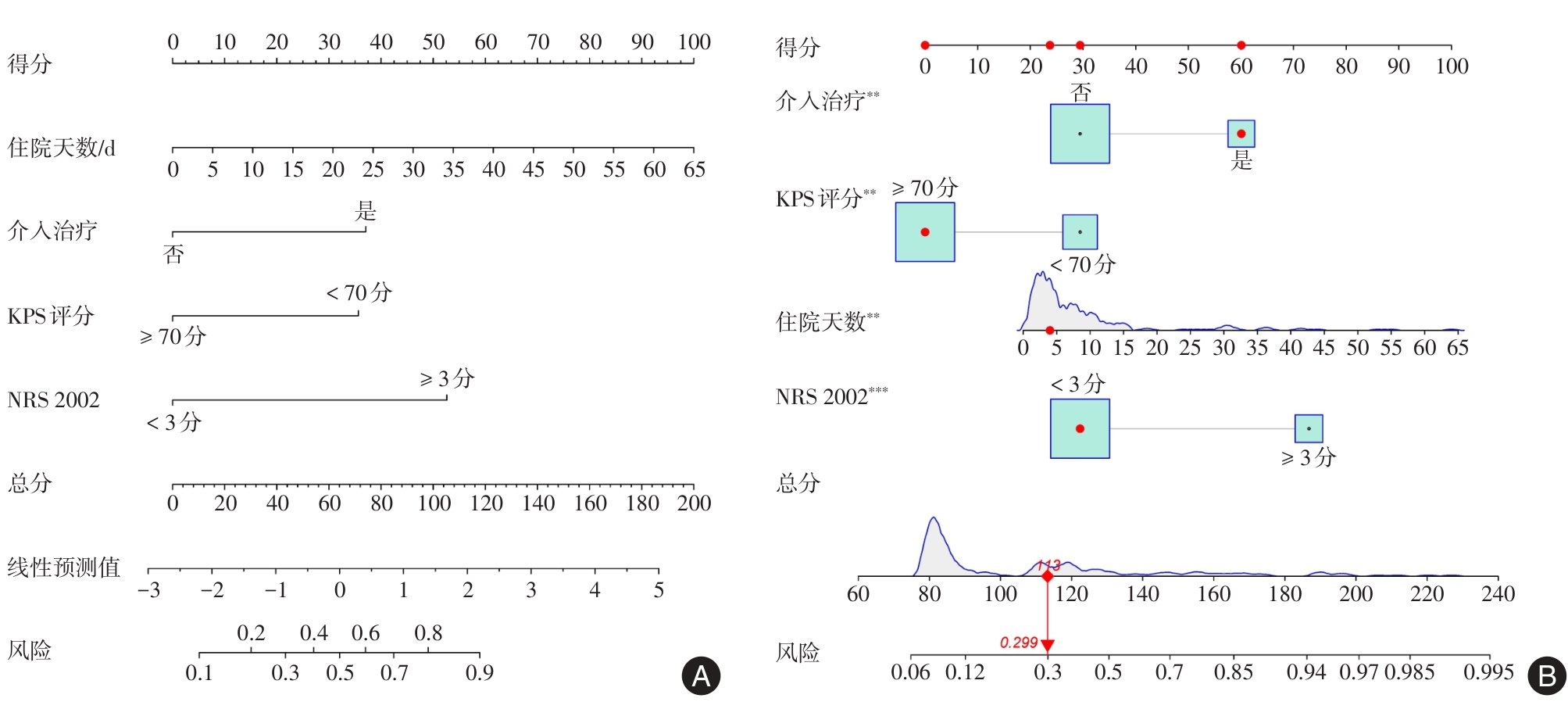

Fig.4
SHAP-based interpretability analysis of the nomogram model"
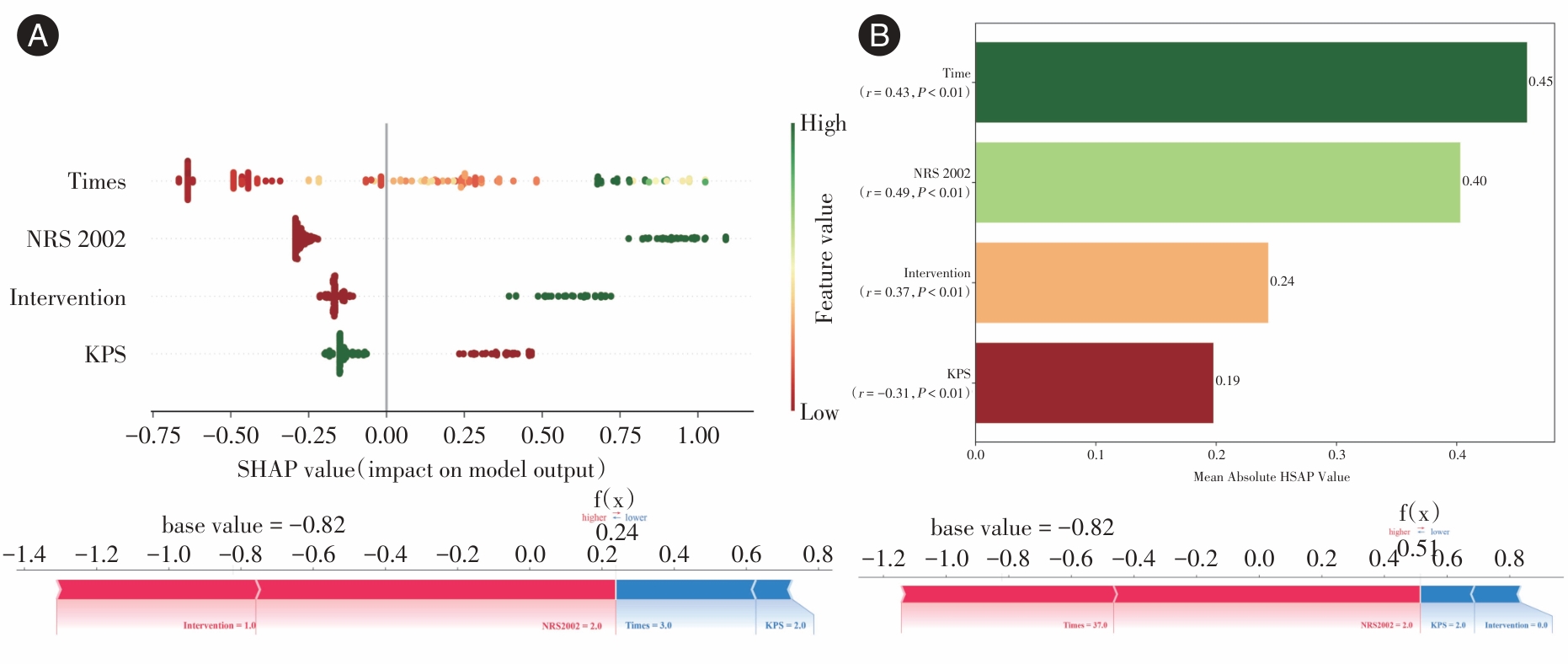
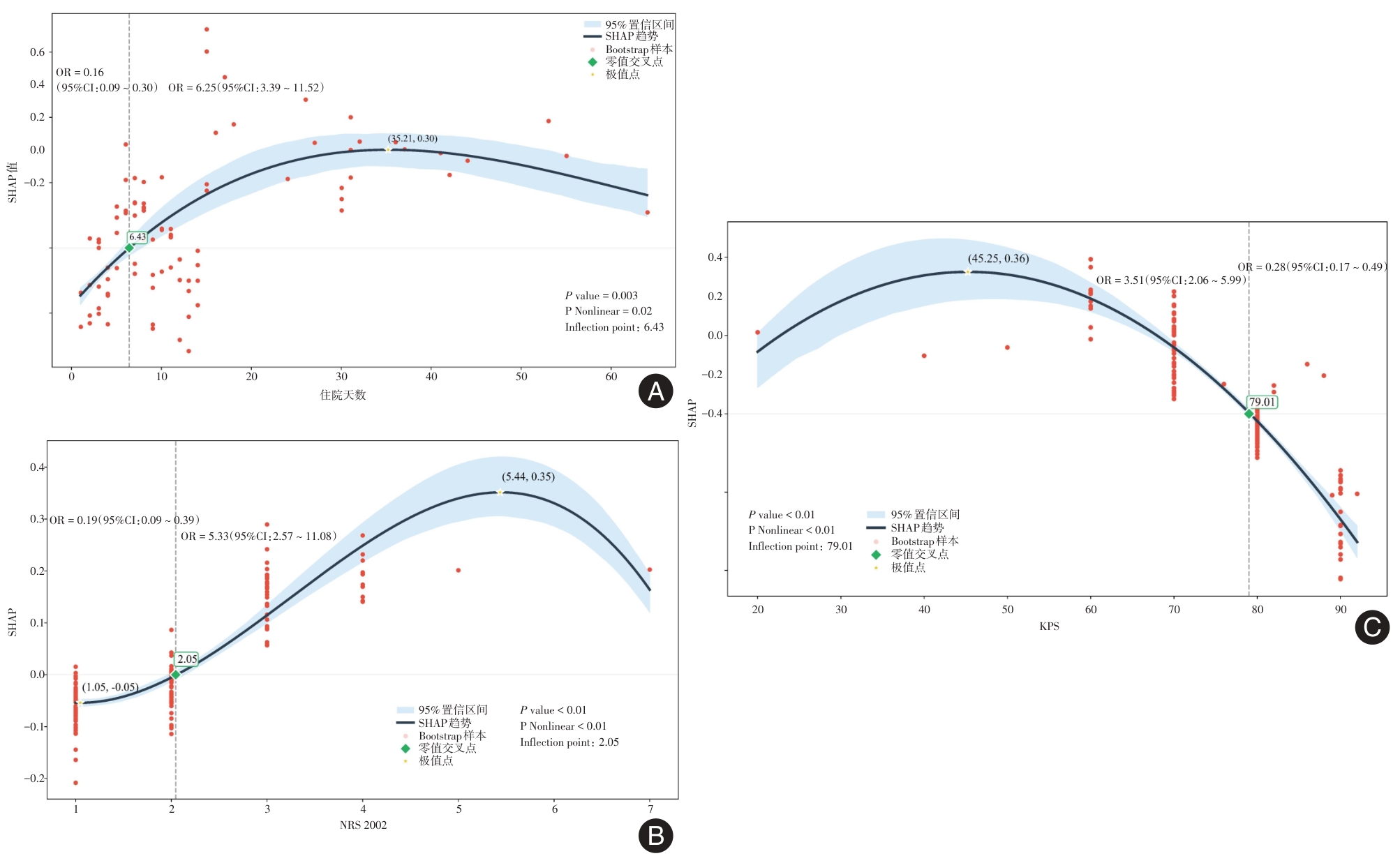
Fig.5
SHAP-RCS trend analysis of KPS, NRS 2002, and length of hospital stay"
| [1] |
BRAY F, LAVERSANNE M, SUNG H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA-Cancer J Clin, 2024,74(3):229-263. doi: 10.3322/caac.21834 .
doi: 10.3322/caac.21834 |
| [2] |
SÁNCHEZ J C, NUÑEZ-GARCÍA B, RUANO-RAVINA A, et al. Patterns and outcome of unplanned care in lung cancer patients: An observational study in a medical oncology department[J]. Transl Lung Cancer Res, 2023, 12(8):1752-1765. doi: 10.21037/tlcr-23-48 .
doi: 10.21037/tlcr-23-48 |
| [3] |
MEDBERY R L, GILLESPIE T W, LIU Y, et al. Socioeconomic factors are associated with readmission after lobectomy for early stage lung cancer[J]. Ann Thorac Surg, 2016, 102(5): 1660-1667. doi: 10.1016/j.athoracsur.2016.05.060 .
doi: 10.1016/j.athoracsur.2016.05.060 |
| [4] |
PURI V, PATEL A P, CRABTREE T D, et al. Unexpected readmission after lung cancer surgery: A benign event? [J]. J Thorac Cardiovasc Surg, 2015, 150(6): 1496-504, 505.e1-5; discussion 504-505. doi: 10.1016/j.jtcvs.2015.08.067 .
doi: 10.1016/j.jtcvs.2015.08.067 |
| [5] |
CHUETZ P, SULO S, WALZER S, et al. Gomes F. Cost savings associated with nutritional support in medical inpatients: An economic model based on data from a systematic review of randomised trials[J]. BMJ Open, 2021, 11(7): e046402. doi: 10.1136/bmjopen-2020-046402 .
doi: 10.1136/bmjopen-2020-046402 |
| [6] |
NAIMI A, MOHAMMED R N, RAJI A, et al. Tumor immunotherapies by immune checkpoint inhibitors (ICIs); the pros and cons[J]. J Cell Commun Signal, 2022,20(1):44. doi: 10.1186/s12964-022-00854-y .
doi: 10.1186/s12964-022-00854-y |
| [7] |
WANG S J, DOUGAN S K, DOUGAN M. Immune mechanisms of toxicity from checkpoint inhibitors[J]. Trends in Cancer, 2023,9(7):543-553. doi: 10.1016/j.trecan.2023.04.002 .
doi: 10.1016/j.trecan.2023.04.002 |
| [8] |
CHHABRA N, KENNEDY J. A review of cancer immunotherapy toxicity: Immune checkpoint inhibitors[J]. J Med Toxicol, 2021, 17(4):411-424. doi: 10.1007/s13181-021-00833-8 .
doi: 10.1007/s13181-021-00833-8 |
| [9] |
THOMPSON J A, SCHNEIDER B J, BRAHMER J, et al. Management of immunotherapy-related toxicities, version 1.2022, nccn clinical practice guidelines in oncology[J]. J Natl Compr Canc Netw, 2022, 20(4):387-405. doi: 10.6004/jnccn. 2022. 0020 .
doi: 10.6004/jnccn. 2022. 0020 |
| [10] |
COUSSENS L M, WERB Z. Inflammation and cancer[J]. Nature, 2002, 420(6917): 860-867. doi: 10.1038/nature01322 .
doi: 10.1038/nature01322 |
| [11] |
GRETEN F R, GRIVENNIKOV S I. Inflammation and cancer: Triggers, mechanisms, and consequences[J]. Immunity, 2019, 51(1): 27-41. doi: 10.1016/j.immuni.2019.06.025 .
doi: 10.1016/j.immuni.2019.06.025 |
| [12] |
MANTOVANI A. The inflammation-cancer connection[J]. FEBS J, 2018, 285(4): 638-640. doi: 10.1111/febs.14395 .
doi: 10.1111/febs.14395 |
| [13] |
ECCLESTON D, DUONG M N, CHOWDHURY E, et al. Early vs. Late readmission following percutaneous coronary intervention: Predictors and impact on long-term outcomes[J]. J Clin Med, 2023, 12(4):1684. doi: 10.3390/jcm12041684 .
doi: 10.3390/jcm12041684 |
| [14] |
HUANG D, HARRISON R, CURTIS E, et al. Beyond post-operative readmissions: Analysis of the impact of unplanned readmissions during primary treatment of advanced-stage epithelial ovarian cancer on long-term oncology outcome[J]. Int J Gynecol Cancer, 2023, 33(5):741-748. doi: 10.1136/ijgc-2022-003765 .
doi: 10.1136/ijgc-2022-003765 |
| [15] |
KASPER J, WACH J, VYCHOPEN M, et al. Unplanned 30-day readmission in glioblastoma patients: Implications for the extent of resection and adjuvant therapy[J]. Cancers (Basel), 2023, 15(15):390. doi: 10.3390/cancers15153907 .
doi: 10.3390/cancers15153907 |
| [16] |
VAN SMEDEN M, MOONS K G, DE GROOT J A, et al. Sample size for binary logistic prediction models: Beyond events per variable criteria[J]. Stat Methods Med Res, 2019, 28(8): 2455-2474. doi: 10.1177/0962280218784726 .
doi: 10.1177/0962280218784726 |
| [17] |
VITTINGHOFF E, MCCULLOCH C E. Relaxing the rule of ten events per variable in logistic and Cox regression[J]. Am J Epidemiol, 2007, 165(6): 710-718. doi: 10.1093/aje/kwk052 .
doi: 10.1093/aje/kwk052 |
| [18] |
SOHIL F, SOHALI M U, SHABBIR J. An introduction to statistical learning with applications in R, eISBN: 978-1-4614-7137-7[J]. Statist Theor Relat Field, 2022, 6(1): 87. doi: 10.1080/24754269.2021.1980261 .
doi: 10.1080/24754269.2021.1980261 |
| [19] |
KURSA M B, RUDNICKI W R. Feature selection with the boruta package[J]. J Statist Soft, 2010, 36(11): 1-13. doi: 10.18637/jss.v036.i11 .
doi: 10.18637/jss.v036.i11 |
| [20] |
LUNDBERG S, LEE S I. A Unified Approach to Interpreting Model Predictions[J]. arXiv, 2017. doi:10.48550/arXiv. 1705. 07874 .
doi: 10.48550/arXiv. 1705. 07874 |
| [21] |
ZHU R, ZHANG Y, ZHANG J, et al. Development and validation of an explainable machine learning model for predicting occult lymph node metastasis in early-stage oral tongue squamous cell carcinoma a multi-center study[J]. Int J Surg, 2025,111(8):5022-5035. doi: 10.1097/JS9.0000000000002641 .
doi: 10.1097/JS9.0000000000002641 |
| [22] |
DONG W, JIANG H, LI Y, et al. Interpretable machine learning analysis of immunoinflammatory biomarkers for predicting CHD among NAFLD patients[J]. Cardiovasc Diabetol, 2025, 24(1):263. doi: 10.1186/s12933-025-02818-1 .
doi: 10.1186/s12933-025-02818-1 |
| [23] |
李文锋, 李建华, 王正昕. 肝癌肝移植术前应用免疫检查点抑制剂治疗的进展[J]. 器官移植, 2025, 16(3): 329-337. doi: 10.12464/j.issn.1674-7445.2025094 .
doi: 10.12464/j.issn.1674-7445.2025094 |
| [24] |
陈静文, 徐林霞, 吴秀丽, 等. 基于Logistic回归与决策树模型的结直肠癌术后患者非计划性再入院影响因素分析[J]. 护理学报, 2022,29(2):1-6. doi: 10.16460/j.issn1008-9969. 2022. 02.001 .
doi: 10.16460/j.issn1008-9969. 2022. 02.001 |
| [25] |
李静, 侯云霞, 强万敏. 癌症患者非计划性再入院风险预测模型的范围综述[J]. 中华护理杂志, 2022,57(9):1079-1087. doi: 10.3761/j.issn.0254-1769.2022.09.008 .
doi: 10.3761/j.issn.0254-1769.2022.09.008 |
| [26] |
SHAH M P, NEAL J W. Relative impact of anticancer therapy on unplanned hospital care in patients with non–small-cell lung cancer[J]. JCO Oncol Pract, 2021, 17(8): e1131-e1138. doi: 10.1200/OP.20.00612 .
doi: 10.1200/OP.20.00612 |
| [27] |
HARRON K, GILBERT R, CROMWELL D, et al. Newborn length of stay and risk of readmission[J]. Paediatr Perinat Epidemiol, 2017, 31(3):221-232. doi: 10.1111/ppe.12359 .
doi: 10.1111/ppe.12359 |
| [28] |
LENNES I T, EUSEBIO J, BOHLEN N, et al. Characterization of unplanned 30-day medical oncology readmissions after discharge at an academic medical center with a comprehensive cancer center[J]. J Clin Oncol, 2016, 34(7) suppl: 269. doi: 10.1200/jco.2016.34.7_suppl.269 .
doi: 10.1200/jco.2016.34.7_suppl.269 |
| [29] |
BISWAS S, DINH D, LUCAS M, et al. Incidence and predictors of unplanned hospital readmission after percutaneous coronary intervention[J]. J Clin Med, 2020, 9(10):3242. doi: 10.3390/jcm9103242 .
doi: 10.3390/jcm9103242 |
| [30] |
刘剑, 李敏菁. 全身免疫炎症指数对非小细胞肺癌免疫检查点抑制剂疗效的预测价值[J].实用医学杂志, 2022,38(7):904-908. doi: 10.3969/j.issn.1006-5725.2022.07.024 .
doi: 10.3969/j.issn.1006-5725.2022.07.024 |
| [31] |
TANG Q, CHEN Y, LI X, et al. The role of PD-1/PD-L1 and application of immune-checkpoint inhibitors in human cancers[J]. Front Immunol, 2022,13(1):964442. doi: 10.3389/fimmu. 2022.964442 .
doi: 10.3389/fimmu. 2022.964442 |
| [32] |
CATA J P, CORRALES G, SPEER B, et al. Postoperative acute pain challenges in patients with cancer[J]. Best Pract Res Clin Anaesthesiol, 2019,33(3):361-371. doi: 10.1016/j.bpa. 2019. 07.018 .
doi: 10.1016/j.bpa. 2019. 07.018 |
| [33] | WU D T Y, VITHALA T M, VU H, et al. Development of a clinical decision support system to predict unplanned cancer readmissions[J]. AMIA Annu Symp Proc, 2022,2022:1173-1180. |
| [34] |
THIAGARAJAN S, KANTAMANI T, SATHE P, et al. Impact of surgical site infection on unplanned hospital readmissions, initiation of adjuvant treatment following surgery, and disease-free survival on patients with upper aerodigestive tract squamous cell carcinoma[J]. J Surg Oncol, 2023,128(4):692-700. doi: 10.1002/jso.27356 .
doi: 10.1002/jso.27356 |
| [35] |
GUVEN D C, CEYLAN F, CAKIR I Y, et al. Evaluation of early unplanned readmissions and predisposing factors in an oncology clinic[J]. Support Care Cancer, 2021,29(7):4159-4164. doi: 10.1007/s00520-020-05927-7 .
doi: 10.1007/s00520-020-05927-7 |
| [36] |
YUAN Q, YAO H J, XI C H, et al. Perioperative risk factors associated with unplanned neurological intensive care unit readmission following elective supratentorial brain tumor resection[J]. J Neurosurg, 2022, 139(2):315-323. doi: 10.3171/2022.10.JNS221318 .
doi: 10.3171/2022.10.JNS221318 |
| [37] |
ZHOU J, YE D, ZHANG S, et al. The impact of karnofsky performance status on prognosis of patients with hepatocellular carcinoma in liver transplantation[J]. BMC Gastroenterol, 2024,24(1):85. doi: 10.1186/s12876-024-03161-7 .
doi: 10.1186/s12876-024-03161-7 |
| [38] |
郭科迪, 武岩, 汤夕慧, 等.术前衰弱对老年肺癌患者术后并发症的影响[J]. 实用医学杂志, 2023,39(15):1956-1960. doi: 10.3969/j.issn.1006-5725.2023.15.017 .
doi: 10.3969/j.issn.1006-5725.2023.15.017 |
| [39] |
MANZANO J M, LIN H, ZHAO H, et al. Derivation and validation of the cancer readmit score: a readmission risk scoring system for patients with solid tumor malignancies[J]. JCO Oncol Pract, 2022,18(1): e117-e128. doi: 10.1200/OP.20.01077 .
doi: 10.1200/OP.20.01077 |
| [40] |
PRADO C M, PURCELL S A, LAVIANO A. Nutrition interventions to treat low muscle mass in cancer[J]. J Cachexia Sarcopenia Muscle, 2020,11(2):366-380. doi: 10.1002/jcsm.12525 .
doi: 10.1002/jcsm.12525 |
| [41] |
匡荣康, 顾熙. 南京某三级医院2015至2019年间胃肠道恶性肿瘤病人营养风险和营养治疗现状调查分析[J]. 肠外与肠内营养, 2020,27(6):350-354. doi: 10.16151/j.1007-810x.2020.06.007 .
doi: 10.16151/j.1007-810x.2020.06.007 |
| [42] |
CHANG L, CHENG Q, MA Y, et al. Prognostic effect of the controlling nutritional status score in patients with esophageal cancer treated with immune checkpoint inhibitor[J]. J Immunother, 2022, 45(9):415-422. doi: 10.1097/CJI.0000000000000438 .
doi: 10.1097/CJI.0000000000000438 |
| [43] |
HERSBERGER L, BARGETZI L, TRIBOLET P, et al. Nutritional risk screening (NRS 2002) is a strong and modifiable predictor risk score for short-term and long-term clinical outcomes: Secondary analysis of a prospective randomised trial[J]. Clin Nutr, 2020,39(9):2720-2729. doi: 10.1016/j.clnu.2019.11.041 .
doi: 10.1016/j.clnu.2019.11.041 |
| [44] |
WANG F, DONG Q, YU K, et al. Nutrition risk screening and related factors analysis of non-hospitalized cancer survivors: A nationwide online survey in China[J]. Front Nutr, 2022,9:920714. doi: 10.3389/fnut.2022.920714 .
doi: 10.3389/fnut.2022.920714 |
| [45] |
王娜, 秦卓, 刘慧珍, 等. 营养风险评分对脓毒症相关性急性肾损伤患者预后的临床价值[J]. 中华危重病急救医学, 2022,34(3):245-249. doi: 10.3760/cma.j.cn121430-20211019-01525 .
doi: 10.3760/cma.j.cn121430-20211019-01525 |
| [46] |
GREENLEE H, SANTIAGO-TORRES M, MCMILLEN K K, et al. Helping patients eat better during and beyond cancer treatment: Continued nutrition management throughout care to address diet, malnutrition, and obesity in cancer[J]. Cancer J, 2019,25(5):320-328. doi: 10.1097/PPO.0000000000000405 .
doi: 10.1097/PPO.0000000000000405 |
| [47] |
PRADO C M, LANDI F, CHEW S T H, et al. Advances in muscle health and nutrition: A toolkit for healthcare professionals[J]. Clin Nutr, 2022, 41(10):2244-2263. doi: 10.1016/j.clnu. 2022.07.041 .
doi: 10.1016/j.clnu. 2022.07.041 |
| [48] |
LI Y F, NIE R C, WU T, et al. Prognostic value of the nutritional risk screening 2002 scale in metastatic gastric cancer: A large-scale cohort study[J]. J Cancer, 2019,10(1):112-119. doi: 10.7150/jca.27729 .
doi: 10.7150/jca.27729 |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||