

The Journal of Practical Medicine ›› 2025, Vol. 41 ›› Issue (6): 829-837.doi: 10.3969/j.issn.1006-5725.2025.06.009
• Clinical Research • Previous Articles
Xi LI1,Xiaoying REN1,Yongwei JIAO1,Zhipeng SUN1,Shilin YIN1,Zekun ZHANG2,Tianci GAO3,Jingxi WANG4,Yongwang ZHANG1,Lu LIU5,Shuangqing. DU1( )
)
Received:2024-12-26
Online:2025-03-25
Published:2025-03-31
Contact:
Shuangqing. DU
E-mail:szdushuangqing@sina.com
CLC Number:
Xi LI,Xiaoying REN,Yongwei JIAO,Zhipeng SUN,Shilin YIN,Zekun ZHANG,Tianci GAO,Jingxi WANG,Yongwang ZHANG,Lu LIU,Shuangqing. DU. The effect of hip⁃knee⁃ankle active and passive movement therapy on joint function in early and intermediate⁃stage knee osteoarthritis patients[J]. The Journal of Practical Medicine, 2025, 41(6): 829-837.
Tab.1
Comparison of baseline data among the four groups of KOA patients"
| 组别 | 例数 | 性别 (男/女)/例 | 年龄 (x ± s)/岁 | BMI (x ± s)/(kg/m2) | K-L分级 (Ⅱ/Ⅲ)/例 | 病程 M(P25,P75)/年 | 骨密度#(T值) M(P25,P75) |
|---|---|---|---|---|---|---|---|
| 主动组 | 39 | 8/31 | 61.46 ± 8.12 | 25.92 ± 3.56 | 18/21 | 1.00(0.55,4.00) | -1.30(-2.00,-0.95) |
| 被动组 | 42 | 11/31 | 61.29 ± 10.27 | 26.21 ± 2.73 | 12/24 | 2.04(0.50,5.55) | -1.40(-2.08,-0.90) |
| 结合组 | 40 | 8/32 | 62.20 ± 7.51 | 25.63 ± 2.53 | 12/19 | 1.00(0.50,2.00) | -1.10(-2.15,-0.70) |
| 空白对照组 | 39 | 9/30 | 60.51 ± 9.02 | 26.02 ± 2.73 | 14/18 | 1.00(0.50,4.00) | -1.25(-2.02,-0.47) |
| χ2/F/Z值 | 0.567 | 0.244 | 0.672 | 3.349 | 2.182 | 0.272 | |
| P值 | 0.904 | 0.866 | 0.570 | 0.341 | 0.535 | 0.965 |

Fig.1
Active movement therapy"
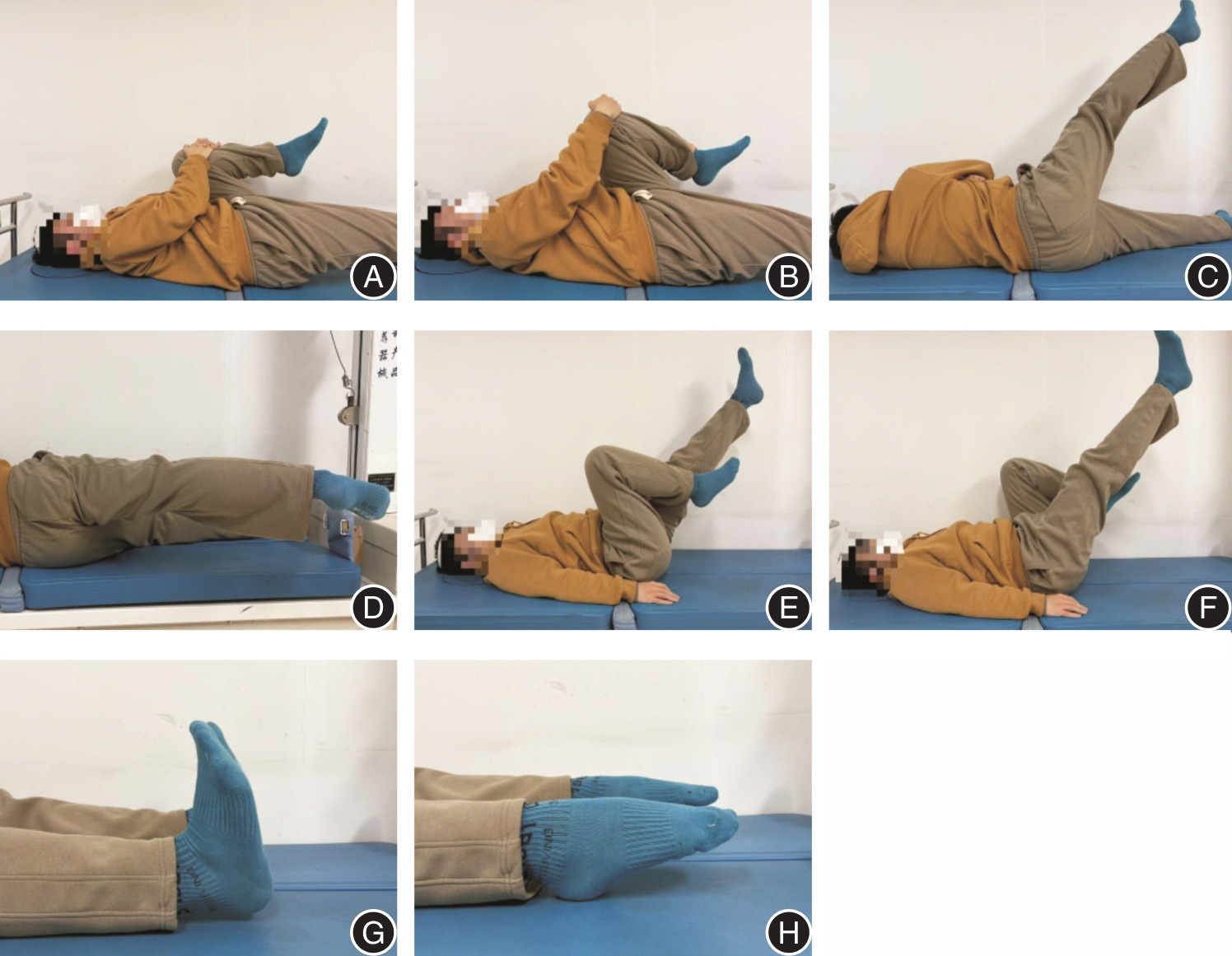

Fig.2
Passive movement therapy"

Tab.2
Comparison of curative effect related indicators after treatment in four groups"
| 结果 | 主动组(n = 39) | 被动组(n = 42) | 结合组(n = 40) | 对照组(n = 39) | 组间Z值 | 组间P值 |
|---|---|---|---|---|---|---|
| WOMAC 功能积分 | ||||||
| 基线时 | 22.0(16.0,34.0) | 24.5(14.0,31.3) | 19.5(13.3,31.8) | 25.0(16.0,32.0) | 0.747 | 0.862 |
| 治疗后2周 | 17.0(14.0,21.0)? | 14.0(8.0,17.0)?△□ | 12.0(9.5,18.0)?△□ | 16.0(10.0,20.5)? | 10.790 | 0.013 |
| 治疗后14周 | 7.0(4.0,11.0)?#△ | 13.0(11.0,18.0)?△□ | 6.0(4.0,8.5)?△○ | 18.0(15.5,21.0)? | 64.677 | < 0.001 |
| WOMAC 疼痛积分 | ||||||
| 基线时 | 9.0(6.0,10.0) | 7.0(5.8,10.0) | 7.0(4.0,10.0) | 8.0(4.0,10.0) | 1.232 | 0.745 |
| 治疗后2周 | 6.0(4.0,7.5)? | 5.0(3.0,5.0)? | 3.5(2.0,6.0)?△□ | 5.0(3.0,7.0)? | 16.037 | 0.001 |
| 治疗后14周 | 2.0(1.0,3.0)?#△ | 5.0(4.0,7.0)?△□ | 2.0(1.0,3.5)?#△○ | 8.0(6.5,9.0)# | 79.638 | < 0.001 |
| WOMAC 僵硬积分 | ||||||
| 基线时 | 3.0(2.0,4.0) | 3.5(2.0,4.0) | 3.0(2.0,4.0) | 3.0(2.0,4.0) | 3.466 | 0.325 |
| 治疗后2周 | 3.0(2.0,4.0)? | 2.0(1.0,2.0)?□ | 2.0(1.0,2.0)?□ | 2.0(1.5,3.0)? | 11.463 | 0.009 |
| 治疗后14周 | 1.0(0.0,2.0)?#△○ | 2.0(1.0,3.0)?△□ | 1.0(0.0,1.0)?#△○ | 3.0(2.0,4.0) | 49.132 | < 0.001 |
| WOMAC总积分 | ||||||
| 基线时 | 34.0(23.0,45.0) | 36.0(21.8,45.0) | 30.0(22.0,45.8) | 35.0(24.0,45.0) | 1.060 | 0.787 |
| 治疗后2周 | 27.0(21.5,30.5)?△ | 21.0(14.0,24.0)?□ | 17.0(13.5,25.0)?△□ | 23.0(14.5,31.0)? | 15.564 | 0.001 |
| 治疗后14周 | 11.0(6.0,16.0)?#△○ | 22.0(16.0,24.0)?△□ | 10.0(6.0,15.5)?#△○ | 29.0(26.0,33.0)?# | 76.889 | < 0.001 |
| SF-12积分 | ||||||
| 基线时 | 35.8(27.3,45.0) | 37.3(27.1,57.2) | 39.2(27.1,47.7) | 42.9(33.5,56.7) | 2.291 | 0.514 |
| 治疗后14周 | 81.3(71.0,89.5)?△○ | 63.7(51.7,72.9)?△□ | 83.3(71.9,89.6)?△○ | 70.8(64.6,77.9)? | 33.311 | < 0.001 |
| HKA角(x ± s) | ||||||
| 基线时 | 175.4 ± 4.9 | 177.3 ± 4.5 | 176.5 ± 3.7 | 176.0 ± 4.9 | 1.256 | 0.292 |
| 治疗后14周 | 175.4 ± 4.7 | 177.2 ± 4.7 | 176.1 ± 3.9 | 176.0 ± 5.1 | 1.067 | 0.365 |
| 1 | 中华医学会骨科学分会关节外科学组,中国医师协会骨科医师分会骨关节炎学组,国家老年疾病临床医学研究中心(湘雅医院),等. 中国骨关节炎诊疗指南(2021年版)[J]. 中华骨科杂志,2021,41(18):1291-1314. |
| 2 | 中华医学会物理医学与康复学分会,四川大学华西医院. 中国膝骨关节炎康复治疗指南(2023版)[J]. 中国循证医学杂志,2024,24(1):1-14. |
| 3 | 肖剑伟. 骨关节炎中西医结合诊疗指南[J]. 风湿病与关节炎,2023,12(6):70-80. |
| 4 |
MOSENG T, VLIET VLIELAND T P M, BATTISTA S, et al. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis:2023 update[J]. Ann Rheum Dis, 2024,83(6):730-740. doi:10.1136/ard-2023-225041
doi: 10.1136/ard-2023-225041 |
| 5 |
HENRIKSEN M. Limitations of the updated EULAR recommendations for osteoarthritis[J]. Nat Rev Rheumatol. 2024,20(6):321-322. doi:10.1038/s41584-024-01103-x
doi: 10.1038/s41584-024-01103-x |
| 6 | 魏光成,秦伟凯,赵勇,等.“筋束骨”理论探源[J].北京中医药大学学报,2024,47(6):765-772. |
| 7 |
KELLGREN J H, LAWRENCE J S. Radiological assessment of osteo-arthrosis[J]. Ann Rheum Dis, 1957,16(4):494-502. doi:10.1136/ard.16.4.494
doi: 10.1136/ard.16.4.494 |
| 8 | 中华医学会骨质疏松和骨矿盐疾病分会. 原发性骨质疏松症诊疗指南(2022)[J]. 中国全科医学,2023,26(14):1671-1691. |
| 9 | CLEGG D O, REDA D J, HARRIS C L, et al. Glucosamine, chondroitin sulfate, and the two in combination for painful knee osteoarthritis[J]. N Engl J Med, 2006, 354(8):795-808. |
| 10 | 史周华. 医学统计学[M]. 北京:人民卫生出版社,2021:38-40. |
| 11 | 中华医学会骨科学分会关节外科学组. 骨关节炎诊疗指南(2018年版)[J]. 中华骨科杂志,2018,38(12):705-715. |
| 12 | 李锡,张健,刘郭辉,等. 脊柱-骨盆-下肢力线正骨手法治疗膝骨关节炎的疗效评价[J]. 实用医学杂志,2024,40(17):2495-2502. |
| 13 | 李锡,杨立英,张永旺,等. 三种中医理筋正骨手法治疗膝骨关节炎随机对照研究[J]. 中国中西医结合杂志,2024,44(11):1307-1313. |
| 14 | 赵文龙. 摇拔戳手法治疗外踝关节扭伤的临床疗效和步态分析研究[D]. 北京:北京中医药大学,2023. |
| 15 | BELLAMY N, BUCHANAN W W, GOLDSMITH C H, et al. Validation study of WOMAC:A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee[J]. J Rheumatol,1988,15(12):1833-1840. |
| 16 |
BELLAMY N. Pain assessment in osteoarthritis: Experience with the WOMAC osteoarthritis index[J]. Semin Arthritis Rheum,1989,18(42):14-17. doi:10.1016/0049-0172(89)90010-3
doi: 10.1016/0049-0172(89)90010-3 |
| 17 |
WARE J JR, KOSINSKI M, KELLER S D. A 12-Item Short-Form Health Survey:Construction of scales and preliminary tests of reliability and validity[J]. Med Care,1996,34:220-233. doi:10.1097/00005650-199603000-00003
doi: 10.1097/00005650-199603000-00003 |
| 18 | 冯华.膝关节运动损伤与下肢力线不良[M]. 北京:人民卫生出版社,2023:1-2. |
| 19 |
MENG X, WANG Z, MA X, et al. Fully automated measurement on coronal alignment of lower limbs using deep convolutional neural networks on radiographic images[J]. BMC Musculoskeletal Disorders, 2022, 23(1):1-11. doi:10.1186/s12891-022-05818-4
doi: 10.1186/s12891-022-05818-4 |
| 20 |
KOLASINSKI S L, NEOGI T, HOCHBERG M C, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee[J]. Arthritis Rheumatol, 2020, 72(2):220-233. doi:10.1002/art.41142
doi: 10.1002/art.41142 |
| 21 |
VAN DOORMAAL M C M, MEERHOFF G A, VLIET VLIELAND T P M, et al. A clinical practice guideline for physical therapy in patients with hip or knee osteoarthritis[J]. Musculoskeletal Care, 2020, 18(4):575-595. doi:10.1002/msc.1492
doi: 10.1002/msc.1492 |
| 22 |
PESARE E, VICENTI G, KON E, et al. Italian Orthopaedic and Traumatology Society (SIOT) position statement on the non-surgical management of knee osteoarthritis[J]. J Orthop Traumatol, 2023, 24(1):47. doi:10.1186/s10195-023-00729-z
doi: 10.1186/s10195-023-00729-z |
| 23 |
WEBER F, KLOEK C, STUHRMANN S, et al. Usability and preliminary effectiveness of an app-based physical activity and education program for people with hip or knee osteoarthritis-a pilot randomized controlled trial[J]. Arthritis Res Ther, 2024, 26(1):83. doi:10.1186/s13075-024-03291-z
doi: 10.1186/s13075-024-03291-z |
| 24 |
BENNELL K L, NELLIGAN R K, KIMP A J, et al. What type of exercise is most effective for people with knee osteoarthritis and co-morbid obesity?: The TARGET randomized controlled trial[J]. Osteoarthritis Cartilage, 2020, 28(6):755-765. doi:10.1016/j.joca.2020.02.838
doi: 10.1016/j.joca.2020.02.838 |
| 25 |
NELLIGAN R K, HINMAN R S, KASZA J, et al. Effects of a Self-directed Web-Based Strengthening Exercise and Physical Activity Program Supported by Automated Text Messages for People With Knee Osteoarthritis: A Randomized Clinical Trial[J]. JAMA Intern Med, 2021, 181(6):776-785. doi:10.1001/jamainternmed.2021.0991
doi: 10.1001/jamainternmed.2021.0991 |
| 26 |
DRUMMEN S J J, RUNHAAR J, BIERMA-ZEINSTRA S M, et al. Early-stage vs established knee osteoarthritis: A comparative observational study on prevalence and changes in pain, function and quality of life after supervised exercise and education among 10,365 patients[J]. Osteoarthritis Cartilage, 2024. doi: 10.1016/j.joca.2024.11.007 . Epub ahead of print.
doi: 10.1016/j.joca.2024.11.007 |
| 27 |
WOLF D F, CARVALHO C, MOREIRA PADOVEZ R F C, et al. Effects of physical exercise on muscle function of the knee, pain and quality of life in postmenopausal women with knee osteoarthritis: A systematic review with meta-analysis[J]. Musculoskelet Sci Pract, 2024, 71:102929. doi:10.1016/j.msksp.2024.102929
doi: 10.1016/j.msksp.2024.102929 |
| 28 |
KNOOP J, ESSER J, DEKKER J, et al. No evidence for stratified exercise therapy being cost-effective compared to usual exercise therapy in patients with knee osteoarthritis: Economic evaluation alongside cluster randomized controlled trial[J]. Braz J Phys Ther, 2023, 27(1):100469. doi:10.1016/j.bjpt.2022.100469
doi: 10.1016/j.bjpt.2022.100469 |
| 29 | 李锡,颜运涛,刘路,等. 运用髋关节推摇拔伸手法治疗初、早期膝骨关节炎:随机对照研究[J]. 北京中医药大学学报,2023,46(12):1756-1762. |
| 30 |
UHLRICH S D, KOLESAR J A, KIDZINSKI L, et al. Personalization improves the biomechanical efficacy of foot progression angle modifications in individuals with medial knee osteoarthritis[J]. J Biomech, 2022,144:111312. doi:10.1016/j.jbiomech.2022.111312
doi: 10.1016/j.jbiomech.2022.111312 |
| 31 |
YANG L, SINSURIN K, SHEN F, et al. Biomechanical changes in lower extremity in individuals with knee osteoarthritis in the past decade: A scoping review[J]. Heliyon, 2024,10(11):e32642. doi:10.1016/j.heliyon.2024.e32642
doi: 10.1016/j.heliyon.2024.e32642 |
| 32 |
DU P, YAN Y, YIN S, LI X, et al. Correlation Between Coronal Position Sequence of Lumbar and WOMAC Score in Knee Osteoarthritis (KOA) in Standard Standing Position[J]. Adv Ther, 2024,41(7):2924-2935. doi:10.1007/s12325-024-02898-7
doi: 10.1007/s12325-024-02898-7 |
| 33 |
LIU S, AMIRI P, MCGREGOR A H, et al. Bilateral Asymmetry in Knee and Hip Musculoskeletal Loading During Stair Ascending/Descending in Individuals with Unilateral Mild-to-Moderate Medial Knee Osteoarthritis[J]. Ann Biomed Eng, 2023,51(11):2490-2503. doi:10.1007/s10439-023-03289-9
doi: 10.1007/s10439-023-03289-9 |
| 34 |
DOCKING S, ADEMI Z, BARTON C, et al. Lifetime Cost-Effectiveness of Structured Education and Exercise Therapy for Knee Osteoarthritis in Australia[J]. JAMA Netw Open, 2024,7(10):e2436715. doi:10.1001/jamanetworkopen.2024.36715
doi: 10.1001/jamanetworkopen.2024.36715 |
| 35 |
WEI G, SHANG Z, LI Y, et al. Effects of lower-limb active resistance exercise on mobility, physical function, knee strength and pain intensity in patients with total knee arthroplasty: A systematic review and meta-analysis[J]. BMC Musculoskelet Disord, 2024,25(1):730. doi:10.1186/s12891-024-07845-9
doi: 10.1186/s12891-024-07845-9 |
| 36 |
LIU H, CONG H, CHEN L, et al. Efficacy and Safety of Lower Limb Progressive Resistance Exercise for Patients With Total Knee Arthroplasty: A Meta-analysis of Randomized Controlled Trials[J]. Arch Phys Med Rehabil, 2021,102(3):488-501. doi:10.1016/j.apmr.2020.05.021
doi: 10.1016/j.apmr.2020.05.021 |
| [1] | Shangzeng WANG,Bei ZHANG,Zhen WANG,Shang MA,Deyang RUANGZHANG,Zhiying YIN,Yunqi ZHU,Kunpeng HU,Shao CHENG. Comparison of the effects of CR and PS prostheses in the treatment of knee osteoarthritis [J]. The Journal of Practical Medicine, 2024, 40(9): 1251-1256. |
| [2] | Yuke SONG,Jinfan XU,Xiaoming HE,Tianye LIN,Mincong HE,Qiushi. WEI. Correlation of high signal intensity of infrapatellar fat pad on symptoms and structure of knee osteoarthritis [J]. The Journal of Practical Medicine, 2024, 40(23): 3373-3378. |
| [3] | Lingling ZHU,Yanchun CHEN,Liang FANG,Chengyan CAI,Ting. LIU. Clinical effectiveness of dynamic joint mobilization combined with core stability training for nonspecific low back pain treatment [J]. The Journal of Practical Medicine, 2024, 40(18): 2602-2606. |
| [4] | Binbin ZHANG,Yongrui WU,Chao LI,Kai FAN,Jingtang ZHANG. Clinical application of personalized osteotomy guide based on rapid 3D printing in knee arthroplasty [J]. The Journal of Practical Medicine, 2024, 40(17): 2448-2453. |
| [5] | Xi LI,Jian ZHANG,Guohui LIU,Yunhao LIU,Zekun ZHANG,Tianci GAO,Jingxi WANG,Yongwang ZHANG,Shilin YIN,Lu LIU,Liqing QI,Shuangqing. DU. Evaluation of the curative effect of traditional Chinese medicine bone-setting technique in the treatment of knee osteoarthritis [J]. The Journal of Practical Medicine, 2024, 40(17): 2495-2502. |
| [6] |
LI Liang, ZHOU Zhengxin, LI Wenhua, LIU Tao, ZHU Lei, KANG Jinping..
The study of effect of YiqiYangying Decoction used in perioperation for cases of severe knee osteoarthritis treated by artificial knee resurfacing surgery [J]. The Journal of Practical Medicine, 2023, 39(7): 904-909. |
| [7] |
YAN Zhenjie, SUN Honglin, ZHAO Lingfeng, WANG Huanxin. .
Effects of injection needle scalpel,small needle scalpel and sodium hyaluronate intraarticular injectionon knee osteoarthritis:a comparative study [J]. The Journal of Practical Medicine, 2023, 39(5): 591-596. |
| [8] | Haitao TU,Xun ZHUANG,Lixing ZHUANG,Zhengpeng FAN,Yu. PAN. Clinical observation of the effect and efficacy of fire on serum IL⁃1β and TNF⁃α in knee osteoarthritis [J]. The Journal of Practical Medicine, 2023, 39(22): 3000-3004. |
| [9] | Shanshan HU,Xiao LIU,Hancai LUO,Yayun WU,Xiaoman WU,Lili NIU,Min PAN. Clinical study of low intensity pulsed ultrasound in the treatment of painful knee osteoarthritis [J]. The Journal of Practical Medicine, 2023, 39(21): 2783-2789. |
| [10] | YAO Fang⁃ ming, HE Mincong, HE Xiaoming, WEI Qiushi, HE Wei. . Advances in the characterization of lipid metabolism in synovial fluid with knee osteoarthritis [J]. The Journal of Practical Medicine, 2023, 39(15): 1992-1997. |
| [11] |
CHEN Fuyan, ZHOU Xin, WU Bangqi. .
Clinical efficacy of radiofrequency acupotomy combined with ozone injection for the treatment of knee osteoarthritis [J]. The Journal of Practical Medicine, 2022, 38(3): 335-339. |
| [12] |
WU Di, SI Lina, WU Lizhu, WANG Jianhua, LUO Jinwei, CHANG Qiankun, LÜ Yongming, YANG Yang..
Application of 3D printing osteotomy guide plate for multi ⁃radius prosthesis total knee arthroplasty in patients with severe knee osteoarthritis and its effect on surgical trauma and joint function [J]. The Journal of Practical Medicine, 2022, 38(2): 190-195. |
| [13] |
HONG Kunhao, WU Huai, LIU Wengang, YANG Wenbin, YE Guozhu, LIU Xin..
Correlation between serum PTX3 and CTRP3 levels and osteoporosis in patients with knee osteoarthritis [J]. The Journal of Practical Medicine, 2022, 38(16): 2046-2050. |
| [14] |
XU Xuemeng, LIU Wen′gang, XU Shuchai, LI Yikai, ZHANG Qingwen, HUANG Hongxing, GUAN Honggang, LU Chao, JIANG Tao..
Clinical practice guidelines for knee osteoarthritis in integrated traditional chinese and western medicine [J]. The Journal of Practical Medicine, 2021, 37(22): 2827-2833. |
| [15] |
LIU Zhichao, FU Lixin, CUI Yanjiang, YANG Keqiang, MIAO Wei, ZHANG Shuqin, LI Xin, MA Zilong, JIA Yusong, LI Jinyu, ZHENG Chenying, ZHANG Fan, LIU Chuyin, YUAN Qiaomei, DI Xueshi, KANG Shengqian, CHEN Jiang..
A double center comparative study of Oxford unicompartment knee replacement and total knee arthroplas⁃ ty in treatment of medial knee osteoarthritis [J]. The Journal of Practical Medicine, 2021, 37(19): 2487-2491. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||