实用医学杂志 ›› 2025, Vol. 41 ›› Issue (9): 1361-1367.doi: 10.3969/j.issn.1006-5725.2025.09.013
• 临床研究 • 上一篇
韦晨龙,王昆( )
)
Chenlong WEI,Kun WANG()
摘要:
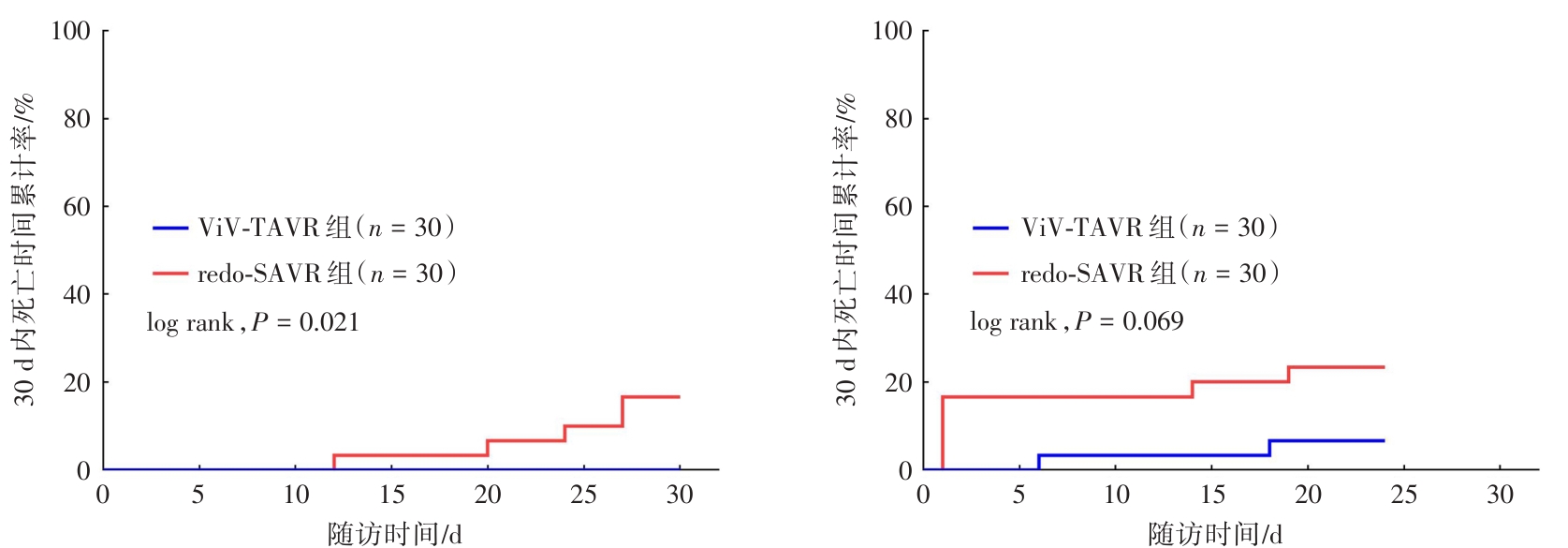
目的 比较经导管瓣中瓣置换术(ViV-TAVR)与二次外科主动脉瓣置换术(redo-SAVR)在生物瓣膜衰败患者中的应用效果及安全性。 方法 回顾性收集2020年1月至2022年6月医院收治的61例接受ViV-TAVR或redo-SAVR治疗的生物瓣膜衰败患者临床资料。根据治疗方案不同分为ViV-TAVR组(n = 31)与redo-SAVR组(n = 30)。比较两组围术期相关指标(手术时间、住院时间、机械通气时间、重症监护室观察时间),术前(T1)、术后1个月(T2)、术后3个月(T3)、术后6个月(T4)超声心动图指标,主要终点事件与次要终点事件。 结果 ViV-TAVR组手术时间、住院时间较redo-SAVR组更短,体外循环辅助较redo-SAVR组更少,差异有统计学意义(P < 0.05)。组内比较显示,术后1个月(T2)、术后3个月(T3)、术后6个月(T4)时点两组左心室射血分数(LVEF)、主动脉瓣峰值流速(AVmax)、峰值跨瓣压差(PGmax)、PGmean均低于术前(T1)时点,T3、T4时点两组左心室舒张末期内径(LVEDD)均低于T1、T2时点,差异有统计学意义(P < 0.05)。ViV-TAVR组30 d内死亡率低于redo-SAVR组,差异有统计学意义(P < 0.05);两组24个月内的全因死亡率比较,差异无统计学意义(P > 0.05)。ViV-TAVR组急性肾衰竭发生率低于redo-SAVR组,差异有统计学意义(P < 0.05)。 结论 相较于redo-SAVR,ViV-TAVR能有效降低生物瓣膜衰败患者30 d内的死亡风险以及急性肾衰竭的发生风险,但其远期死亡率与redo-SAVR相当。
中图分类号: