

The Journal of Practical Medicine ›› 2026, Vol. 42 ›› Issue (6): 969-980.doi: 10.3969/j.issn.1006-5725.2026.06.009
• Oncology: Diagnosis, Treatment and Prevention • Previous Articles Next Articles
Sudong LIANG1( ),Ziqiang HUANG1,Jianzhong LIN2
),Ziqiang HUANG1,Jianzhong LIN2
Received:2025-12-25
Revised:2026-01-30
Accepted:2026-02-03
Online:2026-03-25
Published:2026-03-26
Contact:
Sudong LIANG
E-mail:hupo5357979@163.com
CLC Number:
Sudong LIANG,Ziqiang HUANG,Jianzhong LIN. The short-term and long-term efficacy of rezvilutamide combined with androgen deprivation therapy in the treatment of patients with metastatic hormone-sensitive prostate cancer and its influence on the expression of FPSAR and ProGRP[J]. The Journal of Practical Medicine, 2026, 42(6): 969-980.
Tab.1
The baseline data of the two groups before PSM"
| 资料 | 瑞维鲁胺组(n = 44) | 比卡鲁胺组(n = 58) | χ2 /t值 | P值 |
|---|---|---|---|---|
| 年龄(x ± s)/岁 | 67.52 ± 7.13 | 70.36 ± 6.76 | 2.052 | 0.043 |
| 体质量(x ± s)/kg | 67.86 ± 8.57 | 66.51 ± 10.93 | 0.676 | 0.500 |
| 基础疾病 | ||||
| 合并糖尿病 | 11(25.00) | 18(31.03) | 0.448 | 0.503 |
| 合并高血压 | 16(36.36) | 25(43.10) | 0.473 | 0.492 |
| 临床分期 | 0.015 | 0.902 | ||
| Ⅳa期 | 8(18.18) | 10(17.24) | ||
| Ⅳb期 | 36(81.82) | 48(82.76) | ||
| 转移部位 | 0.126 | 0.989 | ||
| 骨转移 | 22(50.00) | 27(46.55) | ||
| 骨转移 + 淋巴结转移 | 14(31.82) | 20(34.48) | ||
| 内脏转移(肺、肝) | 5(11.36) | 7(12.07) | ||
| 多部位转移(骨 + 内脏 + 淋巴结) | 3(6.82) | 4(6.90) | ||
| ECOG评分 | 0.001 | 0.971 | ||
| 0 ~ 1分 | 41(93.18) | 53(91.38) | ||
| 2分 | 3(6.82) | 5(8.62) | ||
| Gleason评分 | 0.266 | 0.606 | ||
| ≥ 8分 | 29(65.91) | 41(70.69) | ||
| < 8分 | 15(34.09) | 17(29.31) | ||
| 肿瘤负荷 | 1.061 | 0.303 | ||
| 高瘤负荷 | 31(70.45) | 46(79.31) | ||
| 低瘤负荷 | 13(29.55) | 12(20.69) | ||
| 基线血清PSA(x ± s)/(ng/mL) | 79.52 ± 15.17 | 80.24 ± 17.23 | 0.220 | 0.826 |
| 基线LDH(x ± s)/(U/L) | 238.79 ± 47.83 | 240.52 ± 51.09 | 0.174 | 0.862 |
| 基线NLR(x ± s) | 2.41 ± 0.63 | 2.71 ± 0.45 | 2.805 | 0.006 |
| 基线PLR(x ± s) | 125.36 ± 25.47 | 135.14 ± 30.17 | 1.732 | 0.086 |
Tab.2
The baseline data of the two groups after PSM"
| 资料 | 瑞维鲁胺组(n = 41) | 比卡鲁胺组(n = 41) | χ2 /t值 | P值 |
|---|---|---|---|---|
| 年龄(x ± s)/岁 | 68.32 ± 7.15 | 68.79 ± 6.95 | 0.302 | 0.764 |
| 体质量(x ± s)/kg | 67.52 ± 8.34 | 67.23 ± 8.57 | 0.155 | 0.877 |
| 基础疾病 | ||||
| 合并糖尿病 | 10(24.39) | 11(26.83) | 0.064 | 0.800 |
| 合并高血压 | 15(36.59) | 17(41.46) | 0.205 | 0.651 |
| 临床分期 | 0.082 | 0.775 | ||
| Ⅳa期 | 7(17.07) | 8(19.51) | ||
| Ⅳb期 | 34(82.93) | 33(80.49) | ||
| 转移部位 | 0.373 | 0.946 | ||
| 骨转移 | 21(51.22) | 20(48.78) | ||
| 骨转移 + 淋巴结转移 | 13(31.71) | 14(34.15) | ||
| 内脏转移(肺、肝) | 4(9.76) | 5(12.20) | ||
| 多部位转移(骨 + 内脏 + 淋巴结) | 3(7.32) | 2(4.88) | ||
| ECOG评分 | - | 1.000 | ||
| 0 ~ 1分 | 38(92.68) | 39(95.12) | ||
| 2分 | 3(7.32) | 2(4.88) | ||
| Gleason评分 | 0.053 | 0.817 | ||
| ≥ 8分 | 27(65.85) | 26(63.41) | ||
| < 8分 | 14(34.15) | 15(36.59) | ||
| 肿瘤负荷 | 0.064 | 0.800 | ||
| 高瘤负荷 | 30(73.17) | 31(75.61) | ||
| 低瘤负荷 | 11(26.83) | 10(24.39) | ||
| 基线血清PSA(x ± s)/(ng/mL) | 78.52 ± 14.17 | 79.65 ± 15.21 | 0.348 | 0.729 |
| 基线LDH(x ± s)/(U/L) | 235.71 ± 42.78 | 237.14 ± 48.25 | 0.142 | 0.887 |
| 基线NLR(x ± s) | 2.38 ± 0.61 | 2.51 ± 0.52 | 1.038 | 0.302 |
| 基线PLR(x ± s) | 124.29 ± 23.41 | 126.34 ± 27.63 | 0.362 | 0.718 |
Tab.3
Comparison of recent therapeutic effects ofthe two groups"
| 项目 | 瑞维鲁胺组 | 比卡鲁胺组 | Z/χ2 值 | P值 |
|---|---|---|---|---|
| 疗效等级 | 1.972 | 0.049 | ||
| 完全缓解 | 3(7.32) | 1(2.44) | ||
| 部分缓解 | 25(60.98) | 20(48.78) | ||
| 稳定 | 9(21.95) | 9(21.95) | ||
| 进展 | 4(9.76) | 11(26.83) | ||
| DCR | 37(90.24) | 30(73.17) | 3.998 | 0.046 |
| PSA50 | 37(90.24) | 29(70.73) | 4.970 | 0.026 |
| PSA90 | 30(73.17) | 21(51.22) | 4.201 | 0.040 |
Tab.4
Comparison of laboratory indicators between the two groups"
| 组别 | 例数 | FPSAR/% | LDH/(U/L) | proGRP/(pg/mL) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 基线 | 治疗24周 | 差值 | 基线 | 治疗24周 | 差值 | 基线 | 治疗24周 | 差值 | ||
| 瑞维鲁胺组 | 41 | 13.79 ± 4.01 | 20.51 ± 3.36* | 6.72 ± 3.69 | 235.71 ± 42.78 | 206.36 ± 30.51* | 29.35 ± 36.65 | 45.14 ± 8.36 | 30.05 ± 7.14* | 15.09 ± 7.75 |
| 比卡鲁胺组 | 41 | 13.57 ± 3.86 | 16.32 ± 4.23* | 2.75 ± 4.05 | 237.14 ± 48.25 | 231.25 ± 50.36 | 5.89 ± 49.31 | 46.01 ± 9.74 | 37.14 ± 8.51* | 8.87 ± 9.13 |
| t值 | 0.253 | 4.966 | 4.640 | 0.142 | 2.707 | 2.445 | 0.434 | 4.087 | 3.326 | |
| P值 | 0.801 | < 0.001 | < 0.001 | 0.887 | 0.008 | 0.017 | 0.656 | < 0.001 | 0.001 | |
| 组别 | 例数 | NLR | PLR | PSA/(ng/mL) | ||||||
| 基线 | 治疗24周 | 差值 | 基线 | 治疗24周 | 差值 | 基线 | 治疗24周 | 差值 | ||
| 瑞维鲁胺组 | 41 | 2.38 ± 0.61 | 1.71 ± 0.36* | 0.67 ± 0.49 | 124.29 ± 23.41 | 93.05 ± 10.76* | 31.24 ± 17.09 | 78.52 ± 14.17 | 1.75 ± 0.52* | 76.77 ± 7.35 |
| 比卡鲁胺组 | 41 | 2.51 ± 0.52 | 2.03 ± 0.41* | 0.48 ± 0.47 | 126.34 ± 27.63 | 110.14 ± 7.94* | 16.20 ± 17.79 | 79.65 ± 15.21 | 2.96 ± 0.71* | 76.69 ± 7.96 |
| t值 | 1.038 | 3.755 | 1.792 | 0.362 | 8.183 | 3.904 | 0.348 | 8.804 | 0.047 | |
| P值 | 0.302 | < 0.001 | 0.077 | 0.718 | < 0.001 | < 0.001 | 0.729 | < 0.001 | 0.962 | |
Tab.5
Comparison of the incidence rates of adverse events between the two groups"
| 分类 | 不良事件 | 分级 | 瑞维鲁胺组(n = 41) | 比卡鲁胺组(n = 41) | χ2值 | P值 |
|---|---|---|---|---|---|---|
| 内分泌系统 | 潮热 | 1级 | 18(43.90) | 16(39.02) | 0.201 | 0.654 |
| 2级 | 5(12.20) | 4(9.76) | - | 1.000 | ||
| 3级 | 0(0.00) | 1(2.44) | - | 1.000 | ||
| 乳房胀痛 | 1级 | 6(14.63) | 8(19.51) | 0.345 | 0.557 | |
| 2级 | 2(4.88) | 3(7.32) | - | 1.000 | ||
| 3级 | 0(0.00) | 0(0.00) | - | - | ||
| 心血管系统 | 高血压 | 1级 | 7(17.07) | 5(12.20) | 0.391 | 0.532 |
| 2级 | 4(9.76) | 3(7.32) | - | 1.000 | ||
| 3级 | 1(2.44) | 1(2.44) | 0.513 | 0.474 | ||
| 心悸 | 1级 | 3(7.32) | 2(4.88) | - | 1.000 | |
| 2级及以上 | 0(0.00) | 0(0.00) | - | - | ||
| 消化系统 | 恶心 | 1级 | 5(12.20) | 6(14.63) | 0.105 | 0.745 |
| 2级 | 1(2.44) | 1(2.44) | 0.513 | 0.474 | ||
| 腹泻 | 1级 | 4(9.76) | 3(7.32) | - | 1.000 | |
| 2级及以上 | 0(0.00) | 0(0.00) | - | - | ||
| 血液系统 | 中性粒细胞减少 | 1级 | 2(4.88) | 1(2.44) | - | 1.000 |
| 2级及以上 | 0(0.00) | 0(0.00) | - | - | ||
| 贫血 | 1级 | 3(7.32) | 2(4.88) | - | 1.000 | |
| 2级及以上 | 0(0.00) | 0(0.00) | - | - | ||
| 神经系统 | 乏力 | 1级 | 10(24.39) | 9(21.95) | 0.069 | 0.794 |
| 2级 | 3(7.32) | 2(4.88) | - | 1.000 | ||
| 头晕 | 1级 | 4(9.76) | 3(7.32) | - | 1.000 | |
| 2级及以上 | 0(0.00) | 0(0.00) | - | - | ||
| 皮肤及附件 | 皮疹 | 1级 | 2(4.88) | 1(2.44) | - | 1.000 |
| 2级及以上 | 0(0.00) | 0(0.00) | ||||
| 其他 | 骨痛加重 | 1级 | 1(2.44) | 2(4.88) | - | 1.000 |
| 2级 | 0(0.00) | 1(2.44) | - | 1.000 | ||
| 合计 | 任何不良事件 | - | 35(85.37) | 33(80.49) | 0.345 | 0.557 |
| 3级 | - | 1(2.44) | 2(4.88) | - | 1.000 |
Tab.6
Comparison of PFS and OS during follow-up between the two groups"
| 组别 | 例数 | PFS | |||||
|---|---|---|---|---|---|---|---|
| 均值 | 中位数 | ||||||
| 估计值 | SE | 95%CI | 估计值 | SE | 95%CI | ||
| 瑞维鲁胺组 | 41 | 32.55 | 1.587 | 29.443 ~ 35.665 | 37.20 | 1.701 | 33.866 ~ 40.534 |
| 比卡鲁胺组 | 41 | 17.18 | 2.090 | 13.088 ~ 21.279 | 15.30 | 2.162 | 11.063 ~ 19.537 |
| Log-rank χ2 值 | 28.309 | ||||||
| P值 | < 0.001 | ||||||
| 组别 | 例数 | OS | |||||
| 均值 | 中位数 | ||||||
| 估计值 | SE | 95%CI | 估计值 | SE | 95%CI | ||
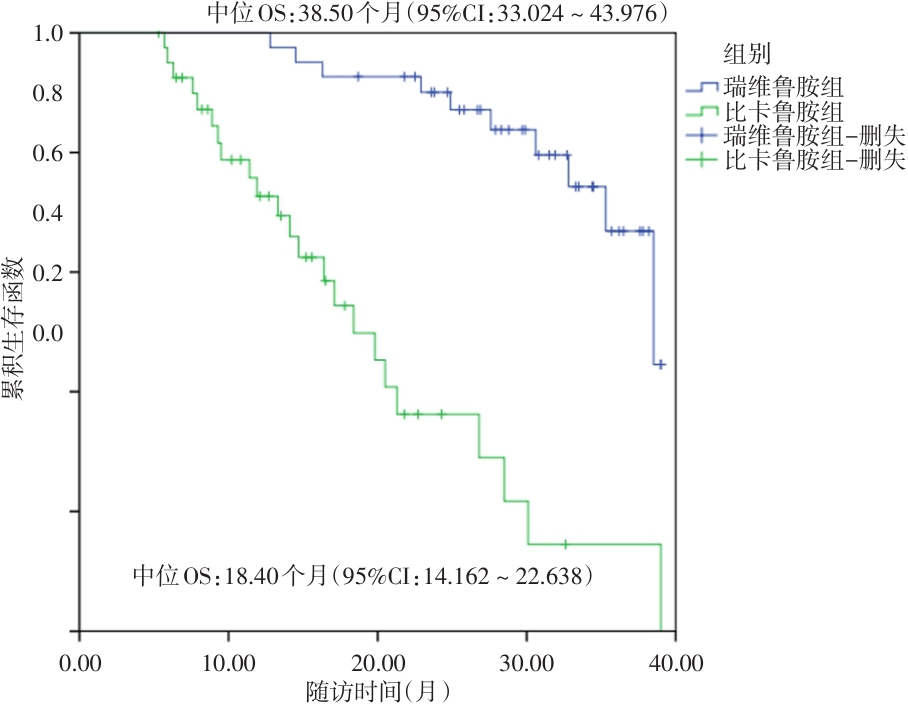
| 瑞维鲁胺组 | 41 | 34.93 | 1.193 | 32.586 ~ 37.264 | 38.50 | 2.794 | 33.024 ~ 43.976 |
| 比卡鲁胺组 | 41 | 20.61 | 2.050 | 16.593 ~ 24.627 | 18.40 | 2.162 | 14.162 ~ 22.638 |
| Log-rank χ2 值 | 29.209 | ||||||
| P值 | < 0.001 | ||||||
Fig.1
Comparison of PFS between the two groups"
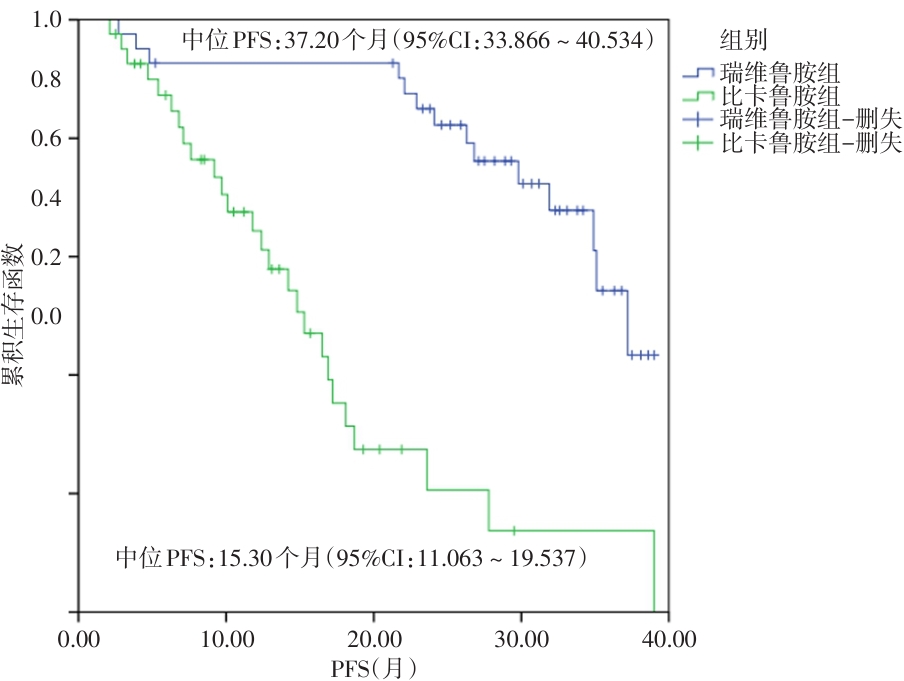
Fig.2
Comparison of OS between the two groups"
Tab.7
Comparison of clinical characteristics among patients with different prognoses"
| 资料 | 生存组(n = 49) | 死亡组(n = 33) | χ2 /t值 | P值 |
|---|---|---|---|---|
| 年龄(x ± s)/岁 | 66.98 ± 7.63 | 67.08 ± 7.71 | 0.058 | 0.954 |
| 体质量(x ± s)/kg | 67.34 ± 8.41 | 67.17 ± 8.23 | 0.091 | 0.928 |
| 基础疾病 | ||||
| 合并糖尿病 | 12(24.49) | 9(27.27) | 0.080 | 0.777 |
| 合并高血压 | 18(36.73) | 14(42.42) | 0.205 | 0.651 |
| 临床分期 | 3.129 | 0.077 | ||
| Ⅳa期 | 12(24.49) | 3(9.09) | ||
| Ⅳb期 | 37(75.51) | 30(90.91) | ||
| 转移部位 | 30.169 | < 0.001 | ||
| 骨转移 | 36(73.47) | 5(15.15) | ||
| 骨转移 + 淋巴结转移 | 11(22.45) | 16(48.48) | ||
| 内脏转移(肺、肝) | 2(4.08) | 7(21.21) | ||
| 多部位转移(骨 + 内脏 + 淋巴结) | 0(0.00) | 5(15.15) | ||
| ECOG评分 | 1.961 | 0.161 | ||
| 0 ~ 1分 | 48(97.96) | 29(87.88) | ||
| 2分 | 1(2.04) | 4(12.12) | ||
| Gleason评分 | 13.054 | 0.001 | ||
| ≥ 8分 | 24(48.98) | 29(87.88) | ||
| < 8分 | 25(51.02) | 4(12.12) | ||
| 肿瘤负荷 | 19.012 | < 0.001 | ||
| 高瘤负荷 | 28(57.14) | 33(100.00) | ||
| 低瘤负荷 | 21(42.86) | 0(0.00) | ||
| 基线血清PSA(x ± s)/(ng/mL) | 68.72 ± 14.93 | 85.71 ± 17.53 | 4.709 | < 0.001 |
| 基线LDH(x ± s)/(U/L) | 229.85 ± 40.69 | 240.63 ± 50.49 | 1.067 | 0.289 |
| 基线NLR(x ± s) | 2.10 ± 0.57 | 2.97 ± 0.34 | 7.867 | < 0.001 |
| 基线PLR(x ± s) | 111.14 ± 20.71 | 139.51 ± 30.34 | 5.037 | < 0.001 |
| 基线FPSAR(x ± s)/% | 14.95 ± 3.63 | 11.05 ± 3.05 | 5.095 | < 0.001 |
| 基线proGRP(x ± s)/(pg/mL) | 39.71 ± 8.14 | 50.57 ± 9.52 | 5.532 | < 0.001 |
| 治疗方式 | 8.570 | 0.003 | ||
| 瑞维鲁胺 + ADT | 31(63.27) | 10(30.30) | ||
| 比卡鲁胺 + ADT | 18(36.73) | 23(69.70) |
Tab.8
mHSPC patient prognosis influencing factorassignment table"
| 自变量 | 赋值 |
|---|---|
| 治疗方式 | 比卡鲁胺 + ADT = 0,瑞维鲁胺 + ADT = 1 |
| 肿瘤负荷 | 低瘤负荷 = 0,高瘤负荷 = 1 |
| 转移部位 | 非多部位转移 = 0,多部位转移 = 1 |
| Gleason评分 | < 8分 = 0,≥ 8分 = 1 |
| 基线PSA | < 45 ng/mL = 0,≥ 45 ng/mL = 1 |
| 基线FPSAR | < 15% = 0,≥ 15% = 1 |
| 基线NLR | < 3.0 = 0,≥ 3.0 = 1 |
| 基线PLR | < 150 = 0,≥ 150 = 1 |
| 基线proGRP | < 45 pg/mL = 0,≥ 45 pg/mL = 1 |
Tab.9
Cox regression analysis of prognostic factors for mHSPC patients"
| 自变量 | β | SE | Wald χ2 | HR | 95%CI | P值 | VIF |
|---|---|---|---|---|---|---|---|
| 治疗方式 | -0.967 | 0.392 | 6.283 | 0.380 | 0.182 ~ 0.795 | 0.012 | 1.086 |
| 肿瘤负荷 | 1.086 | 0.385 | 8.761 | 2.963 | 1.451 ~ 6.050 | 0.003 | 1.324 |
| 转移部位 | 0.855 | 0.372 | 5.318 | 2.351 | 1.164 ~ 4.746 | 0.018 | 1.395 |
| Gleason评分 | 0.281 | 0.369 | 0.587 | 1.324 | 0.645 ~ 2.719 | 0.385 | 1.243 |
| 基线PSA | 0.579 | 0.395 | 3.728 | 1.784 | 0.893 ~ 3.564 | 0.105 | 1.482 |
| 基线FPSAR | -0.754 | 0.362 | 4.378 | 0.470 | 0.232 ~ 0.952 | 0.036 | 1.189 |
| 基线NLR | 0.484 | 0.397 | 2.876 | 1.623 | 0.793 ~ 3.321 | 0.187 | 1.369 |
| 基线PLR | 0.465 | 0.399 | 2.528 | 1.591 | 0.773 ~ 3.278 | 0.213 | 1.304 |
| 基线proGRP | 0.983 | 0.391 | 7.342 | 2.672 | 1.314 ~ 5.438 | 0.007 | 1.215 |
| [1] |
FILHO A M, LAVERSANNE M, FERLAY J, et al. The GLOBOCAN 2022 cancer estimates: Data sources, methods, and a snapshot of the cancer burden worldwide[J]. Int J Cancer, 2025,156(7):1336-1346. doi: 10.1002/ijc.35278 .
doi: 10.1002/ijc.35278 |
| [2] |
BRAY F, LAVERSANNE M, SUNG H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2024,74(3):229-263. doi: 10.3322/caac.21834 .
doi: 10.3322/caac.21834 |
| [3] |
李唯尊, 邢晨, 安恒庆. STAT活化抑制蛋白2基因在前列腺癌中的表达水平及与临床病理特征的关系[J]. 实用医学杂志, 2025, 41(18): 2844-2852. doi:10.3969/j.issn.1006-5725. 2025.18.009 .
doi: 10.3969/j.issn.1006-5725. 2025.18.009 |
| [4] |
RAVAL A D, CHEN S, LITTLETON N, et al. Real-world use of androgen-deprivation therapy intensification for metastatic hormone-sensitive prostate cancer: A systematic review[J]. BJU Int, 2025,135(3):408-421. doi: 10.1111/bju.16577 .
doi: 10.1111/bju.16577 |
| [5] |
FIZAZI K, CLARKE N W, DE SANTIS M, et al. Capivasertib plus abiraterone in PTEN-deficient metastatic hormone-sensitive prostate cancer: CAPItello-281 phase III study[J]. Ann Oncol, 2026,37(1):53-68. doi: 10.1016/j.annonc.2025.10.004 .
doi: 10.1016/j.annonc.2025.10.004 |
| [6] |
GU W, HAN W, LUO H, et al. Rezvilutamide versus bicalutamide in combination with androgen-deprivation therapy in patients with high-volume, metastatic, hormone-sensitive prostate cancer (CHART): A randomised, open-label, phase 3 trial[J]. Lancet Oncol, 2022, 23(10): 1249-1260. doi: 10.1016/S1470-2045(22)00507-1 .
doi: 10.1016/S1470-2045(22)00507-1 |
| [7] |
KEAM S J. Rezvilutamide: First Approval[J]. Drugs, 2023,83(2):189-193. doi: 10.1007/s40265-022-01831-y .
doi: 10.1007/s40265-022-01831-y |
| [8] |
SINGH K, MANDAL S, NAYAK P, et al. Rezvilutamide for metastatic hormone-sensitive prostate cancer[J]. Lancet Oncol, 2022,23(11):e490. doi: 10.1016/S1470-2045(22)00624-6 .
doi: 10.1016/S1470-2045(22)00624-6 |
| [9] |
GARRIDO M M, MARTA J C, BERNARDINO R M, et al. The percentage of [-2]pro-prostate-specific antigen and the prostate health index outperform prostate-specific antigen and the percentage of free prostate-specific antigen in the detection of clinically significant prostate cancer and can be used as reflex tests[J]. Arch Pathol Lab Med, 2022, 146(6): 691-700. doi: 10.5858/arpa.2021-0079-OA .
doi: 10.5858/arpa.2021-0079-OA |
| [10] |
YASHI M, NISHIHARA D, YOKOYAMA M, et al. Plasma progastrin-releasing peptide level shows different predictive profiles for treatment response by androgen receptor axis-targeted agents in patients with metastatic castration-resistant prostate cancer[J]. Cancer Rep (Hoboken), 2023, 6(3): e1762. doi: 10.1002/cnr2.1762 .
doi: 10.1002/cnr2.1762 |
| [11] |
GILLESSEN S, BOSSI A, DAVIS I D, et al. Management of patients with advanced prostate cancer-metastatic and/or castration-resistant prostate cancer: Report of the Advanced Prostate Cancer Consensus Conference (APCCC) 2022[J]. Eur J Cancer, 2023, 185: 178-215. doi: 10.1016/j.ejca.2023.02.018 .
doi: 10.1016/j.ejca.2023.02.018 |
| [12] |
YOUNES A, HILDEN P, COIFFIER B, et al. International Working Group consensus response evaluation criteria in lymphoma (RECIL 2017)[J]. Ann Oncol, 2017, 28(7): 1436-1447. doi: 10.1093/annonc/mdx097 .
doi: 10.1093/annonc/mdx097 |
| [13] |
BARBOSA F G, QUEIROZ M A, FERRARO D A, et al. Prostate-specific Membrane Antigen PET: Therapy response assessment in metastatic prostate cancer[J]. Radiographics,2020, 40(5): 1412-1430. doi: 10.1148/rg.2020200058 .
doi: 10.1148/rg.2020200058 |
| [14] |
FREITES-MARTINEZ A, SANTANA N, ARIAS-SANTIAGO S, et al. Using the Common Terminology Criteria for Adverse Events (CTCAE-Version 5.0) to evaluate the severity of adverse events of anticancer therapies[J]. Actas Dermosifiliogr (Engl Ed), 2021, 112(1): 90-92. doi: 10.1016/j.ad.2019.05.009 .
doi: 10.1016/j.ad.2019.05.009 |
| [15] |
CHEN W, YOSHIDA S, MIURA N, et al. Efficacy of docetaxel addition to next-generation androgen receptor-axis-targeted therapies and androgen deprivation therapy in metastatic hormone-sensitive prostate cancer: A tumor volume-specific analysis[J]. Int J Urol, 2025,32(4): 361-370. doi: 10.1111/iju.15657 .
doi: 10.1111/iju.15657 |
| [16] |
PARIKH M, TANGEN C, HUSSAIN M H A, et al. Three- and seven-month prostate-specific antigen levels as prognostic markers for overall survival in metastatic hormone-sensitive prostate cancer: Results from SWOG S1216, a phase 3 randomized trial of androgen deprivation plus orteronel or bicalutamide[J]. Eur Urol Oncol, 2024, 7(5): 1097-1104. doi: 10.1016/j.euo. 2024. 03.001 .
doi: 10.1016/j.euo. 2024. 03.001 |
| [17] |
BIAN X, GU W, ZHANG X, et al. Correlation of PSA and survival in metastatic hormone-sensitive prostate cancer treated with rezvilutamide plus ADT in the CHART trial[J]. Med, 2025, 6(2): 100520. doi: 10.1016/j.medj.2024.09.009 .
doi: 10.1016/j.medj.2024.09.009 |
| [18] |
SINGH K. Rezvilutamide for metastatic castration-sensitive prostate cancer: CHART trial[J]. Indian J Urol, 2023,39(2): 171-172. doi: 10.4103/iju.iju_336_22 .
doi: 10.4103/iju.iju_336_22 |
| [19] |
ARMSTRONG A J, AZAD A A, IGUCHI T, et al. Improved survival with enzalutamide in patients with metastatic hormone-sensitive prostate cancer[J]. J Clin Oncol, 2022, 40(15): 1616-1622. doi: 10.1200/JCO.22.00193 .
doi: 10.1200/JCO.22.00193 |
| [20] |
HONG J, ZENG X, CHEN W, et al. Cost-effectiveness analysis of rezvilutamide versus bicalutamide and androgen-deprivation therapy in patients with high-volume, metastatic, hormone-sensitive prostate cancer: A markov's model-based evaluation[J]. Front Public Health, 2025, 13: 1574780. doi: 10.3389/fpubh.2025.1574780 .
doi: 10.3389/fpubh.2025.1574780 |
| [21] |
JIA A Y, SPRATT D E. Bicalutamide monotherapy with radiation therapy for localized prostate cancer: A non-evidence-based alternative[J]. Int J Radiat Oncol Biol Phys, 2022, 113(2): 316-319. doi: 10.1016/j.ijrobp.2022.01.037 .
doi: 10.1016/j.ijrobp.2022.01.037 |
| [22] |
GOLDBERG H, GLICKSMAN R, WOON D, et al. Can post-treatment free PSA ratio be used to predict adverse outcomes in recurrent prostate cancer?[J]. BJU Int, 2021, 127(6): 654-664. doi: 10.1111/bju.15236 . Epub 2020 Sep 26.
doi: 10.1111/bju.15236 |
| [23] |
DING H, LI S, XU X, et al. Cost-effectiveness analysis of rezvilutamide versus bicalutamide in the treatment of metastatic hormone-sensitive prostate cancer[J]. BMJ Open, 2024, 14(7): e073170. doi: 10.1136/bmjopen-2023-073170 .
doi: 10.1136/bmjopen-2023-073170 |
| [24] |
FAROKHI S, ROUSHANI M. Flower-like core-shell nanostructures based on natural asphalt coated with Ni-LDH nanosheets as an electrochemical platform for prostate cancer biomarker sensing[J]. Mikrochim Acta, 2023, 190(5): 198. doi: 10.1007/s00604-023-05779-y .
doi: 10.1007/s00604-023-05779-y |
| [25] |
ZHANG C, REN J, KANG Y, et al. Case report and literature review of rezvilutamide in the treatment of hormone-sensitive prostate cancer[J]. Front Oncol, 2024, 14: 1374039. doi: 10.3389/fonc.2024.1374039 .
doi: 10.3389/fonc.2024.1374039 |
| [26] |
NAH E H, CHO S, PARK H, et al. Establishment and validation of reference intervals for tumor markers (AFP, CEA, CA19-9, CA15-3, CA125, PSA, HE4, Cyfra 21-1, and ProGRP) in primary care centers in Korea: A cross-sectional retrospective study[J]. Health Sci Rep, 2023,6(2): e1107. doi: 10.1002/hsr2.1107 .
doi: 10.1002/hsr2.1107 |
| [27] |
崔英杰,张桂芳. 治疗转移性激素敏感性前列腺癌的第2代雄激素受体拮抗剂瑞维鲁胺[J]. 中国新药杂志, 2024, 33(20): 2109-2113. doi: 10.3969/j.issn.1003-3734.2024.20.005 .
doi: 10.3969/j.issn.1003-3734.2024.20.005 |
| [28] |
WU H, GONG M, YUAN R. Relationship between neutrophil-lymphocyte ratio (NLR) and platelet-lymphocyte ratio (PLR) in peripheral blood and prognosis after castration therapy for prostate cancer[J]. Indian J Cancer,2024, 61(1): 193-199. doi: 10.4103/ijc.ijc_211_24 .
doi: 10.4103/ijc.ijc_211_24 |
| [29] |
TAHSIN S, SANE N S, CERNYAR B, et al. AR loss in prostate cancer stroma mediated by NF-κB and p38-MAPK signaling disrupts stromal morphogen production[J]. Oncogene, 2024,43(27): 2092-2103. doi: 10.1038/s41388-024-03064-7 .
doi: 10.1038/s41388-024-03064-7 |
| [30] |
PENG S, ZHANG R, ZOU Z, et al.Real-world multicenter study of rezvilutamide plus androgen deprivation therapy in Chinese patients with high-volume metastatic hormone-sensitive prostate cancer[J]Front Oncol, 2025, 15: 1657772. doi: 10.3389/fonc. 2025.1657772 .
doi: 10.3389/fonc. 2025.1657772 |
| [31] |
LIN K L, TALMOR B, CRUMBAKER M, et al. A review of hot flash management in patients with prostate cancer[J]. J Clin Endocrinol Metab, 2025, 110(9): 2509-2519. doi: 10.1210/clinem/dgaf302 .
doi: 10.1210/clinem/dgaf302 |
| [32] |
TSUBOI I, SCHULZ R J, LAUKHTINA E, et al. Incidence, management, and prevention of gynecomastia and breast pain in patients with prostate cancer undergoing antiandrogen therapy: A systematic review and meta-analysis of randomized controlled trials[J]. Eur Urol Open Sci, 2025, 73: 31-42. doi: 10.1016/j.euros.2025.01.001 .
doi: 10.1016/j.euros.2025.01.001 |
| [33] |
IBÁÑEZ C, TOURÍS-LORES M, MONTESA Á, et al. Drug-drug interactions in metastatic hormone-sensitive prostate cancer (mHSPC): practical considerations for treating men with androgen receptor pathway inhibitors and common medications in this stage[J]. Expert Opin Drug Metab Toxicol, 2025, 21(6): 625-636. doi: 10.1080/17425255.2025.2478167 .
doi: 10.1080/17425255.2025.2478167 |
| [34] |
WU H, SUN L, FENG R, et al. Cost-effectiveness of rezvilutamide versus bicalutamide and androgen-deprivation therapy in patients with highvolume, metastatic, hormone-sensitive prostate cancer[J]. Front Pharmacol,2024, 14: 1269129. doi: 10.3389/fphar.2023.1269129 .
doi: 10.3389/fphar.2023.1269129 |
| [35] |
AZAD A A, PETRYLAK D P, IGUCHI T, et al. Enzalutamide and prostate-specific antigen levels in metastatic prostate cancer: A secondary analysis of the ARCHES randomized clinical trial[J]. JAMA Netw Open, 2025, 8(5): e258751. doi: 10.1001/jamanetworkopen.2025.8751 .
doi: 10.1001/jamanetworkopen.2025.8751 |
| [36] |
MORRIS M J, CASTELLANO D, HERRMANN K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naive patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomised, controlled trial[J]. Lancet,2024, 404(10459): 1227-1239. doi: 10.1016/S0140-6736(24)01653-2 .
doi: 10.1016/S0140-6736(24)01653-2 |
| [37] |
CHOWDHURY S, BJARTELL A, AGARWAL N, et al. Deep, rapid, and durable prostate-specific antigen decline with apalutamide plus androgen deprivation therapy is associated with longer survival and improved clinical outcomes in TITAN patients with metastatic castration-sensitive prostate cancer[J]. Ann Oncol, 2023, 34(5): 477-485. doi: 10.1016/j.annonc.2023.02.009 .
doi: 10.1016/j.annonc.2023.02.009 |
| [38] |
MOHAMMED NAWI A, MASDOR N A, OTHMAN R, et al. Survival rate and prognostic factors of localised prostate cancer in southeast asian countries: A systematic review with meta-analysis[J]. Asian Pac J Cancer Prev, 2023, 24(9): 2941-2095. doi: 10.31557/APJCP.2023.24.9.2941 .
doi: 10.31557/APJCP.2023.24.9.2941 |
| [39] |
LI L, ZHANG Q, WANG Y, et al. Evaluating the diagnostic and prognostic value of serum TuM2-PK, NSE, and ProGRP in small cell lung cancer[J]. J Clin Lab Anal, 2023, 37(7): e24865. doi: 10.1002/jcla.24865 . Epub 2023 Apr 23.
doi: 10.1002/jcla.24865 |
| [1] | Weizun LI,Chen XING,Hengqing AN. STAT activation inhibitory protein 2 is involved in reprogramming of lipid metabolism by regulating the prostate cancer development [J]. The Journal of Practical Medicine, 2025, 41(18): 2844-2852. |
| [2] | Junzhi LIU,Lei QIU,Kun XU,Jianwei LIU,Dehua HU,Hua ZHU,Cheng SHEN,Ming LU,Jiangang. CHEN. Establishment of a nomogram model for predicting pelvic lymph node metastasis in prostate cancer based on systemic immune-infiltration inflammation index [J]. The Journal of Practical Medicine, 2025, 41(15): 2349-2354. |
| [3] | Hongchao SHAO,Qiyuan LUO,Wenbin GAO,Wen LUO,Mushi YE. Resveratrol inhibits prostate cancer growth and hormone resistance: An in vivo study [J]. The Journal of Practical Medicine, 2025, 41(12): 1835-1839. |
| [4] | Weifeng LIU,Zheng DAI,Yibin ZHOU,Kaiwen FENG,Kai WEI,Gule SUN,Dongrong YANG,Jin. ZHU. The value of urine protein kinase Y⁃linked gene promoter site methylation in early diagnosis of prostate cancer [J]. The Journal of Practical Medicine, 2024, 40(5): 688-694. |
| [5] | Canwei CHEN,Zhuangwen LIAO,Ziwen FAN,Shuai HUANG,Yan HUANG,Binwei CHEN. LAMP3 inhibited the proliferation, metastatic and PC⁃3⁃induced vasculogenesis of HUVEC by regulating VEGF/AKT signaling [J]. The Journal of Practical Medicine, 2024, 40(2): 182-187. |
| [6] | Minyu HUANG,Jun WU,Tianzi QIN,Wei ZHOU,Lize SU,Rong QIU,Lu. HUANG. The prognostic value of serum DCLK1 and sTim⁃3 in patients undergoing radical prostatectomy for prostate cancer [J]. The Journal of Practical Medicine, 2023, 39(18): 2368-2372. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||