

The Journal of Practical Medicine ›› 2025, Vol. 41 ›› Issue (19): 3034-3040.doi: 10.3969/j.issn.1006-5725.2025.19.011
• Clinical Research • Previous Articles
Xin WU1,Geqi DING2,Lufeng LI1,Tie HU3,Fei. ZENG3( )
)
Received:2025-06-24
Online:2025-10-10
Published:2025-10-10
Contact:
Fei. ZENG
E-mail:565933022@qq.com
CLC Number:
Xin WU,Geqi DING,Lufeng LI,Tie HU,Fei. ZENG. Association of serum sST2, NT⁃proBNP and echocardiographic parameters with myocardial remodeling in patients with heart failure after acute myocardial infarction[J]. The Journal of Practical Medicine, 2025, 41(19): 3034-3040.
Tab.1
Serum sST2, NT?proBNP and echocardiographic parameters among patients with different cardiac function grades"
| 临床资料 | Killip Ⅱ级组(n = 36) | Killip Ⅲ级组(n = 61) | Killip Ⅳ级组(n = 23) | χ2/F值 | P值 |
|---|---|---|---|---|---|
| 年龄/岁 | 61.47 ± 9.50 | 62.39 ± 9.17 | 64.53 ± 7.75 | 0.821 | 0.443 |
| 性别/例 | 1.330 | 0.514 | |||
| 男 | 22 | 43 | 17 | ||
| 女 | 14 | 18 | 6 | ||
| 糖尿病/[例(%)] | 7(19.44) | 13(21.31) | 5(21.74) | 0.062 | 0.969 |
| 高血压/[例(%)] | 14(38.89) | 34(55.74) | 15(68.18) | 5.096 | 0.078 |
| 冠心病家族史/[例(%)] | 2(5.56) | 4(6.56) | 4(17.39) | 3.086 | 0.214 |
| sST2/(ng/mL) | 59.48 ± 9.75 | 68.51 ± 12.82 | 82.13 ± 15.17 | 23.081 | < 0.001 |
| NT?proBNP/(ng/L) | 674.27 ± 183.96 | 880.61 ± 204.79? | 1026.34 ± 257.96?△ | 21.325 | < 0.001 |
| LVEDD/mm | 53.29 ± 5.47 | 57.05 ± 5.96? | 60.96 ± 6.26?△ | 12.210 | < 0.001 |
| LVESD/mm | 44.95 ± 6.96 | 47.08 ± 5.31? | 52.75 ± 5.38?△ | 12.774 | < 0.001 |
| LVEF/% | 43.63 ± 5.28 | 40.56 ± 5.17? | 37.36 ± 4.46?△ | 10.925 | < 0.001 |
| LAD/mm | 38.13 ± 4.70 | 43.39 ± 5.59 | 46.80 ± 6.47 | 19.029 | < 0.001 |
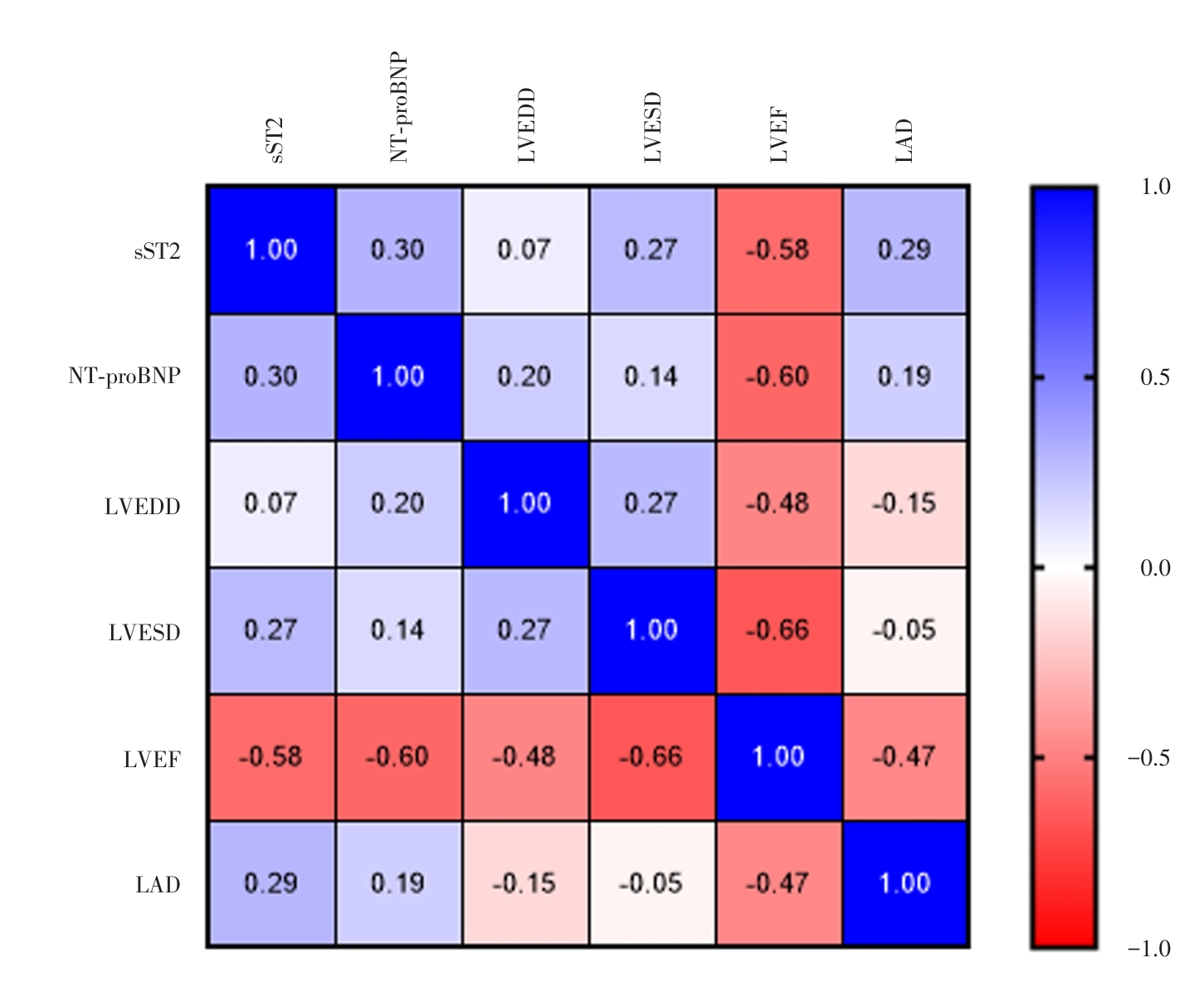
Fig.1
Correlation between serum sST2, NT-proBNP and echocardiographic parameters"
Tab.2
Univariate analysis"
| 临床资料 | 心肌重塑组(n = 31) | 非心肌重塑组(n = 89) | χ2/t/Z值 | P值 |
|---|---|---|---|---|
| 年龄/岁 | 63.59 ± 10.04 | 62.14 ± 9.85 | 0.702 | 0.483 |
| 性别/例 | 0.958 | 0.328 | ||
| 男 | 12 | 26 | ||
| 女 | 19 | 63 | ||
| 糖尿病/[例(%)] | 9(29.03) | 16(17.98) | 1.704 | 0.192 |
| 高血压/[例(%)] | 19(61.29) | 44(49.44) | 1.295 | 0.255 |
| 冠心病家族史/[例(%)] | 3(9.68) | 7(7.87) | 0.099 | 0.753 |
| 心功能分级/[例(%)] | 10.702 | 0.001 | ||
| Ⅱ级 | 6(19.35) | 30(33.71) | ||
| Ⅲ级 | 11(35.48) | 50(56.18) | ||
| Ⅳ级 | 14(45.17) | 9(10.11) | ||
| sST2/(ng/mL) | 84.38 ± 17.02 | 62.85 ± 15.48 | 6.498 | < 0.001 |
| NT?proBNP/(ng/L) | 1003.64 ± 224.36 | 791.95 ± 195.63 | 4.992 | < 0.001 |
| LVEDD/mm | 58.57 ± 7.92 | 56.01 ± 6.53 | 1.776 | 0.078 |
| LVESD/mm | 48.73 ± 5.64 | 47.11 ± 5.16 | 1.469 | 0.144 |
| LVEF/% | 38.93 ± 4.86 | 41.51 ± 5.57 | 2.291 | 0.023 |
| LAD/mm | 45.59 ± 4.93 | 41.37 ± 3.68 | 5.015 | < 0.001 |
Tab.3
Multivariate analysis"
| 变量 | β | SE | Wald χ2 | P值 | OR(95%CI) |
|---|---|---|---|---|---|
| sST2 | 0.415 | 0.198 | 4.393 | 0.037 | 1.514(1.027 ~ 2.232) |
| NTproBNP | 1.019 | 0.332 | 9.420 | 0.002 | 2.770(1.445 ~ 5.311) |
| LAD | 0.606 | 0.277 | 6.019 | 0.015 | 1.833(1.130 ~ 2.975) |

Fig.2
Construction of a nomogram of myocardial remodeling in HF patients after AMI"
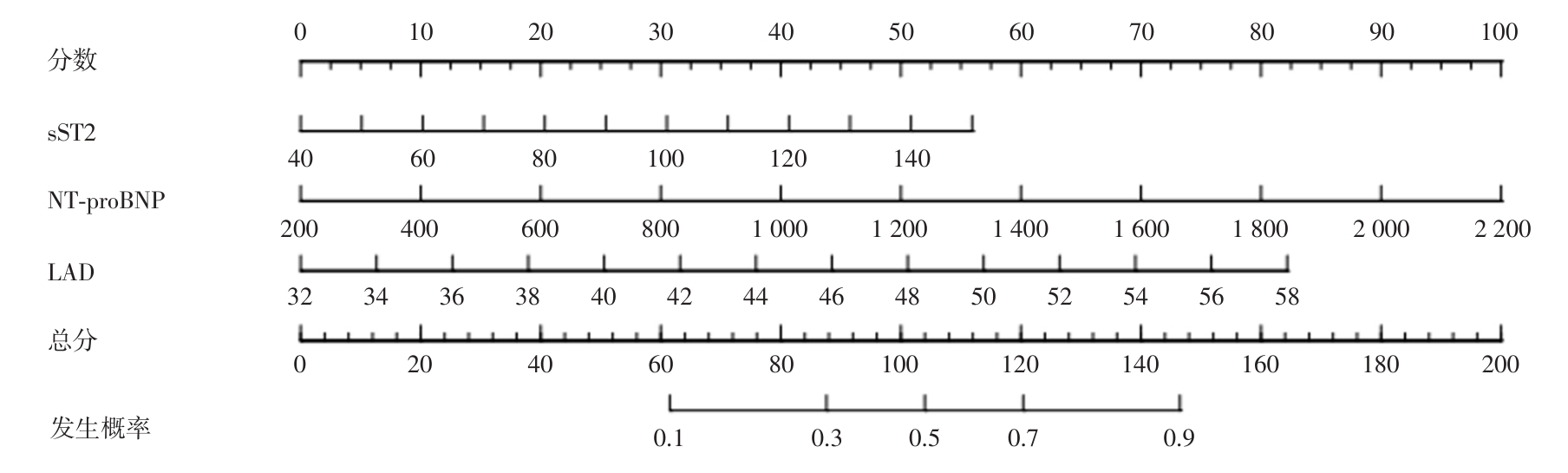
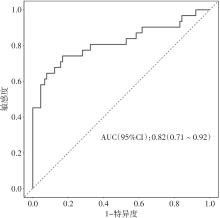
Fig.3
ROC curve of the nomogram for predicting myocardial remodeling in HF patients after AMI"
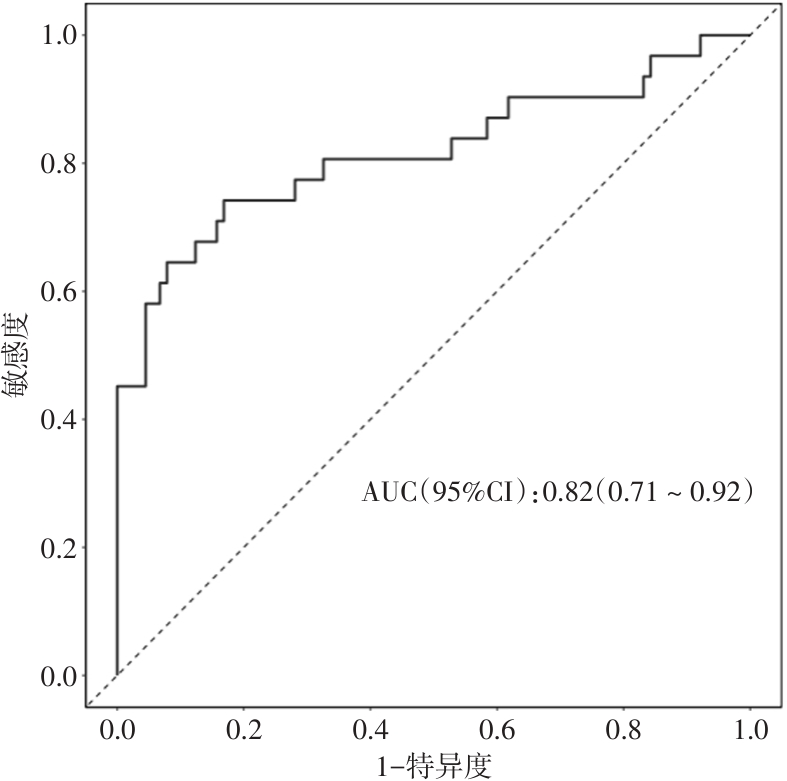
Fig.4
Calibration curve of the nomogram for predicting myocardial remodeling in HF patients after AMI"
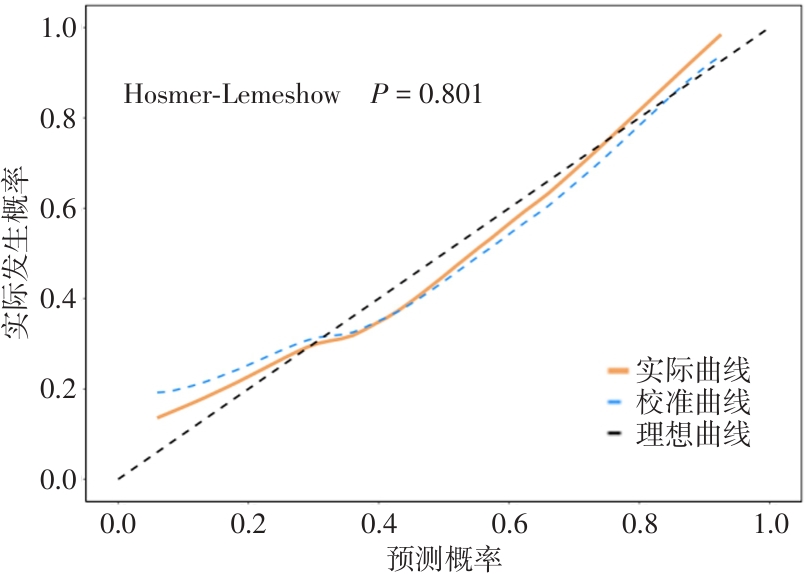
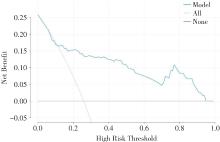
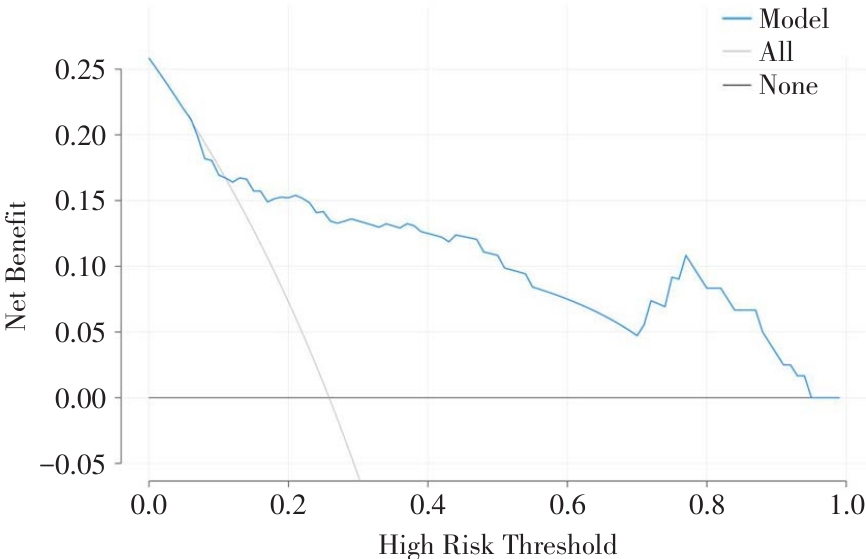
Fig.5
Decision curve of the nomogram for myocardial remodeling in HF patients after AMI"
| [1] |
HERNANDEZ A F, UDELL J A, JONES W S, et al. Effect of Empagliflozin on Heart Failure Outcomes After Acute Myocardial Infarction: Insights From the EMPACT-MI Trial [J]. Circulation, 2024,149(21):1627-1638. doi:10.1161/circulationaha.124.069217
doi: 10.1161/circulationaha.124.069217 |
| [2] |
LI Y W, CHEN S X, YANG Y, et al. Colchicine Inhibits NETs and Alleviates Cardiac Remodeling after Acute Myocardial Infarction [J]. Cardiovasc Drugs Ther, 2024,38(1):31-41. doi:10.1007/s10557-022-07326-y
doi: 10.1007/s10557-022-07326-y |
| [3] |
PAN Y, ZHOU Z, ZHANG H, et al. The Atrqβ-001 Vaccine Improves Cardiac Function and Prevents Postinfarction Cardiac Remodeling in Mice [J]. Hypertens Res, 2019,42(3):329-340. doi:10.1038/s41440-018-0185-3
doi: 10.1038/s41440-018-0185-3 |
| [4] |
CARBERRY J, MARQUIS-GRAVEL G, O'MEARA E, et al. Where Are We With Treatment and Prevention of Heart Failure in Patients Post-Myocardial Infarction? [J]. JACC Heart Fail, 2024,12(7):1157-1165. doi:10.1016/j.jchf.2024.04.025
doi: 10.1016/j.jchf.2024.04.025 |
| [5] |
YNDIGEGN T, LINDAHL B, MARS K, et al. Beta-Blockers after Myocardial Infarction and Preserved Ejection Fraction [J]. N Engl J Med, 2024,390(15):1372-1381. doi:10.1056/nejmoa2401479
doi: 10.1056/nejmoa2401479 |
| [6] |
JIMENEZ-ZEPEDA V H, LEE H, TAY J, et al. N-Terminal Pro-Brain Natriuretic Peptide (Ntprobnp) in Patients with Symptomatic Multiple Myeloma: Report from a Single Institution [J]. Ann Hematol, 2021,100(10):2521-2527. doi:10.1007/s00277-021-04591-z
doi: 10.1007/s00277-021-04591-z |
| [7] |
WANG H, HE K, LIU Y, et al. Expression and Immune Infiltration Studies of Il-33-St2-Nf-κb Signaling Pathway in Prostate Cancer [J]. Prostate, 2024,84(15):1398-1410. doi:10.1002/pros.24778
doi: 10.1002/pros.24778 |
| [8] | 邓昭美,邓志发,徐廉. 基于超声心动图参数和血清学指标构建预测老年慢性心力衰竭患者预后的风险列线图模型[J]. 中华老年心脑血管病杂志,2024,26(9):997-1001. |
| [9] | 孙玥,范洋溢,高旭光. 基于IL-33/ST2L通路研究黄芩苷对缺血性脑卒中大鼠的神经保护作用[J]. 中国免疫学杂志,2023,39(6):1258-1263. |
| [10] |
FIROUZABADI N, DASHTI M, DEHSHAHRI A, et al. Biomarkers of IL-33 and sST2 and Lack of Association with Carvedilol Therapy in Heart Failure [J]. Clin Pharmacol, 2020,12(6):53-58. doi:10.2147/cpaa.s256290
doi: 10.2147/cpaa.s256290 |
| [11] |
HE D, XU H, ZHANG H, et al. Disruption of the Il-33-St2-Akt Signaling Axis Impairs Neurodevelopment by Inhibiting Microglial Metabolic Adaptation and Phagocytic Function [J]. Immunity, 2022,55(1):159-173. doi:10.1016/j.immuni.2021.12.001
doi: 10.1016/j.immuni.2021.12.001 |
| [12] |
李欣雨,吴洋,张红梅,等. 深度学习技术在超声心动图图像质量控制中的应用[J]. 实用医学杂志,2024,40(1):108-113. doi:10.3969/j.issn.1006-5725.2024.01.019
doi: 10.3969/j.issn.1006-5725.2024.01.019 |
| [13] | 中国医师协会心血管内科医师分会,中国心血管健康联盟,心肌梗死后心力衰竭防治专家共识工作组. 2020心肌梗死后心力衰竭防治专家共识[J]. 中国循环杂志,2020,35(12):1166-1180. |
| [14] | 中华医学会超声医学分会超声心动图学组. 中国成年人超声心动图检查测量指南[J]. 中华超声影像学杂志,2016,25(8):645-666. |
| [15] | 中国医师协会胸痛专业委员会,中华心血管病杂志(网络版)编辑委员会,急性心肌梗死后心室重构防治专家共识起草组. 急性心肌梗死后心室重构防治专家共识[J]. 中华心血管病杂志(网络版),2020,3(1): 1-7. |
| [16] | 代爽,冯艳红. 全自动三维超声右心室定量软件评价系统性红斑狼疮患者右心室收缩功能[J]. 实用医学杂志,2023,39(5):636-641. |
| [17] |
YAP J, IREI J, LOZANO-GERONA J, et al. Macrophages in Cardiac Remodelling After Myocardial Infarction [J]. Nat Rev Cardiol, 2023,20(6):373-385. doi:10.1038/s41569-022-00823-5
doi: 10.1038/s41569-022-00823-5 |
| [18] |
CHAKRABORTY P, FARHAT K, PO S S, et al. Autonomic Nervous System and Cardiac Metabolism: Links Between Autonomic and Metabolic Remodeling in Atrial Fibrillation [J]. JACC Clin Electrophysiol, 2023,9(2):1196-1206. doi:10.1016/j.jacep.2023.02.019
doi: 10.1016/j.jacep.2023.02.019 |
| [19] | 康路,忽德运,王攀. 冠心病患者经胸超声心动图定量参数和心室重塑相关血清指标关系及对预后预测价值[J]. 临床误诊误治,2023,36(4):57-62. |
| [20] |
EZEKOWITZ J A, O'CONNOR C M, TROUGHTON R W, et al. N-Terminal Pro-B-Type Natriuretic Peptide and Clinical Outcomes: Vericiguat Heart Failure With Reduced Ejection Fraction Study [J]. JACC Heart Fail, 2020,8(11):931-939. doi:10.1016/j.jchf.2020.08.008
doi: 10.1016/j.jchf.2020.08.008 |
| [21] |
SANTOSO A, MAULANA R, ALZAHRA F, et al. The Effects of Aerobic Exercise on N-terminal Pro-B-type Natriuretic Peptide and Cardiopulmonary Function in Patients With Heart Failure: A Meta-Analysis of Randomised Clinical Trials [J]. Heart Lung Circ, 2020,29(12):1790-1798. doi:10.1016/j.hlc.2020.05.098
doi: 10.1016/j.hlc.2020.05.098 |
| [22] | 中国医师协会心力衰竭专业委员会,国家心血管病专家委员会心力衰竭专业委员会,中华心力衰竭和心肌病杂志编辑委员会. 心力衰竭生物标志物临床应用中国专家共识[J]. 中华心力衰竭和心肌病杂志,2022,6(3):175-192. |
| [23] |
YIN C, LIU B, LI Y, et al. IL-33/ST2 Induces Neutrophil-Dependent Reactive Oxygen Species Production and Mediates Gout Pain [J]. Theranostics, 2020,10(26):12189-12203. doi:10.7150/thno.48028
doi: 10.7150/thno.48028 |
| [24] | THANIKACHALAM P V, RAMAMURTHY S, MALLAPU P, et al. Modulation of IL-33/ST2 Signaling as a Potential New Therapeutic Target for Cardiovascular Diseases [J]. Cytokine Growth Factor Rev, 2023,71(10):94-104. |
| [25] |
MEHRABI NASAB E, HASSANZADEH MAKOEI R, AGHAJANI H, et al. IL-33/ST2 Pathway as Upper-Hand of Inflammation in Allergic Asthma Contributes as Predictive Biomarker in Heart Failure [J]. ESC Heart Fail, 2022,9(6):3785-3790. doi:10.1002/ehf2.14111
doi: 10.1002/ehf2.14111 |
| [26] | 吴文海,陈天宝,陈宏伟. 超声心动图评价动脉导管未闭封堵术后左心室收缩功能变化[J]. 中国超声医学杂志,2024,40(11):1249-1253. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||