

The Journal of Practical Medicine ›› 2025, Vol. 41 ›› Issue (19): 3016-3025.doi: 10.3969/j.issn.1006-5725.2025.19.009
• Clinical Research • Previous Articles
Xiaoyi CHEN1,Chao WANG2,Yan. NIE1( )
)
Received:2025-07-18
Online:2025-10-10
Published:2025-10-10
Contact:
Yan. NIE
E-mail:18702550672@163.com
CLC Number:
Xiaoyi CHEN,Chao WANG,Yan. NIE. A predictive model for bowel preparation quality and mild adverse events in colonoscopy[J]. The Journal of Practical Medicine, 2025, 41(19): 3016-3025.
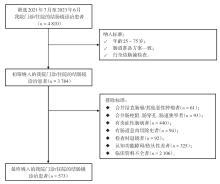
Fig.1
Inclusion flow chart"
Tab.1
Comparison of BBPS scores between qualified and unqualified bowel preparation groups"
| 组别 | 例数 | 右半结肠 | 横结肠 | 左半结肠 | 总分 |
|---|---|---|---|---|---|
| 不合格组 | 112 | 1.00 ± 0.30 | 1.06 ± 0.31 | 0.98 ± 0.23 | 3.04 ± 0.46 |
| 合格组 | 461 | 2.28 ± 0.45 | 2.27 ± 0.44 | 2.31 ± 0.46 | 6.86 ± 0.81 |
| t值 | 28.589 | 27.484 | 29.696 | 48.043 | |
| P值 | < 0.001 | < 0.001 | < 0.001 | < 0.001 |
Tab.2
Occurrence of minor adverse events after colonoscopy"
| 项目 | 第2天 | 第14天 | 第30天 | 合计 |
|---|---|---|---|---|
| 腹痛 | 44 | 16 | 6 | 60 |
| 腹胀 | 34 | 21 | 2 | 54 |
| 腹泻 | 13 | 10 | 1 | 22 |
| 便秘 | 11 | 7 | 3 | 21 |
| 恶心呕吐 | 8 | 1 | 0 | 9 |
| 便血 | 6 | 5 | 2 | 13 |
| 饥饿感 | 14 | 5 | 2 | 16 |
| 出现任一轻微不良事件 | 83(14.49) | 44(7.68) | 13(2.27) | 106(18.50) |
Tab.3
Single factor analysis of unqualified bowel preparation quality in two groups"
| 因素 | 不合格组(n = 112) | 合格组(n = 461) | χ2 值 | P值 |
|---|---|---|---|---|
| 年龄 | 17.851 | < 0.001 | ||
| ≥ 60岁 | 34(30.36) | 63(13.67) | ||
| < 60岁 | 78(69.64) | 398(86.33) | ||
| 性别 | 0.042 | 0.839 | ||
| 男 | 61(54.46) | 256(55.53) | ||
| 女 | 51(45.54) | 205(44.47) | ||
| BMI | 8.731 | 0.003 | ||
| ≥ 28 kg/m2 | 29(25.89) | 66(14.32) | ||
| < 28 kg/m2 | 83(74.11) | 395(85.68) | ||
| 既往史 | ||||
| 便秘史 | 26(23.21) | 33(7.16) | 25.150 | < 0.001 |
| 阑尾手术史 | 36(32.14) | 123(26.68) | 1.341 | 0.247 |
| 肠镜检查史 | 53(47.32) | 207(44.90) | 0.213 | 0.645 |
| 合并基础疾病 | ||||
| 高血压病 | 45(40.18) | 141(30.59) | 3.782 | 0.052 |
| 糖尿病 | 32(28.57) | 37(8.03) | 35.911 | < 0.001 |
| 高血脂 | 12(10.71) | 98(21.26) | 3.521 | 0.061 |
| 周排便次数 | 1.274 | 0.259 | ||
| ≤ 3次 | 10(8.93) | 59(12.80) | ||
| > 3次 | 102(91.07) | 402(87.20) | ||
| 规律排便 | 62(55.36) | 299(64.86) | 3.490 | 0.062 |
| 检查前末次排便有渣 | 7(6.25) | 14(3.04) | 2.635 | 0.105 |
| 合并用药 | ||||
| 钙拮抗剂药物 | 63(56.25) | 149(32.32) | 22.135 | < 0.001 |
| 他汀类药物 | 14(12.50) | 83(18.00) | 1.941 | 0.164 |
| 双胍类药物 | 8(7.14) | 35(7.59) | 0.026 | 0.871 |
| 未按要求饮食 | 18(16.07) | 33(7.16) | 8.829 | 0.003 |
| 末次大便性状 | 1.995 | 0.158 | ||
| 较差/差 | 11(9.82) | 28(6.07) | ||
| 较好/好 | 101(90.18) | 433(93.93) | ||
| Bristol粪便分型 | 39.390 | < 0.001 | ||
| 1 ~ 2型 | 23(20.54) | 17(3.69) | ||
| 3 ~ 7型 | 89(79.46) | 444(96.31) |
Tab.4
Multivariate analysis of unqualified bowel preparation quality in two groups"
| 变量 | β | SE | Wald | P值 | OR值 | 95%CI |
|---|---|---|---|---|---|---|
| 年龄(≥ 60岁) | 1.158 | 0.283 | 16.726 | < 0.001 | 3.182 | 1.827 ~ 5.542 |
| BMI(≥ 28 kg/m2) | 0.847 | 0.299 | 8.058 | 0.005 | 2.334 | 1.300 ~ 4.189 |
| 便秘史(是) | 1.427 | 0.329 | 18.879 | < 0.001 | 4.168 | 2.189 ~ 7.935 |
| 糖尿病(是) | 1.319 | 0.309 | 18.207 | < 0.001 | 3.742 | 2.041 ~ 6.859 |
| 合并使用钙拮抗剂药物(是) | 0.946 | 0.242 | 15.290 | < 0.001 | 2.576 | 1.603 ~ 4.141 |
| 按要求饮食(否) | 0.703 | 0.359 | 3.842 | 0.050 | 2.019 | 1.000 ~ 4.078 |
| Bristol粪便分型(1 ~ 2型) | 1.910 | 0.384 | 24.744 | < 0.001 | 6.754 | 3.182 ~ 14.336 |
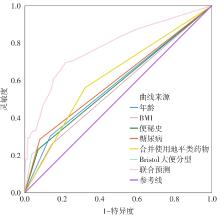
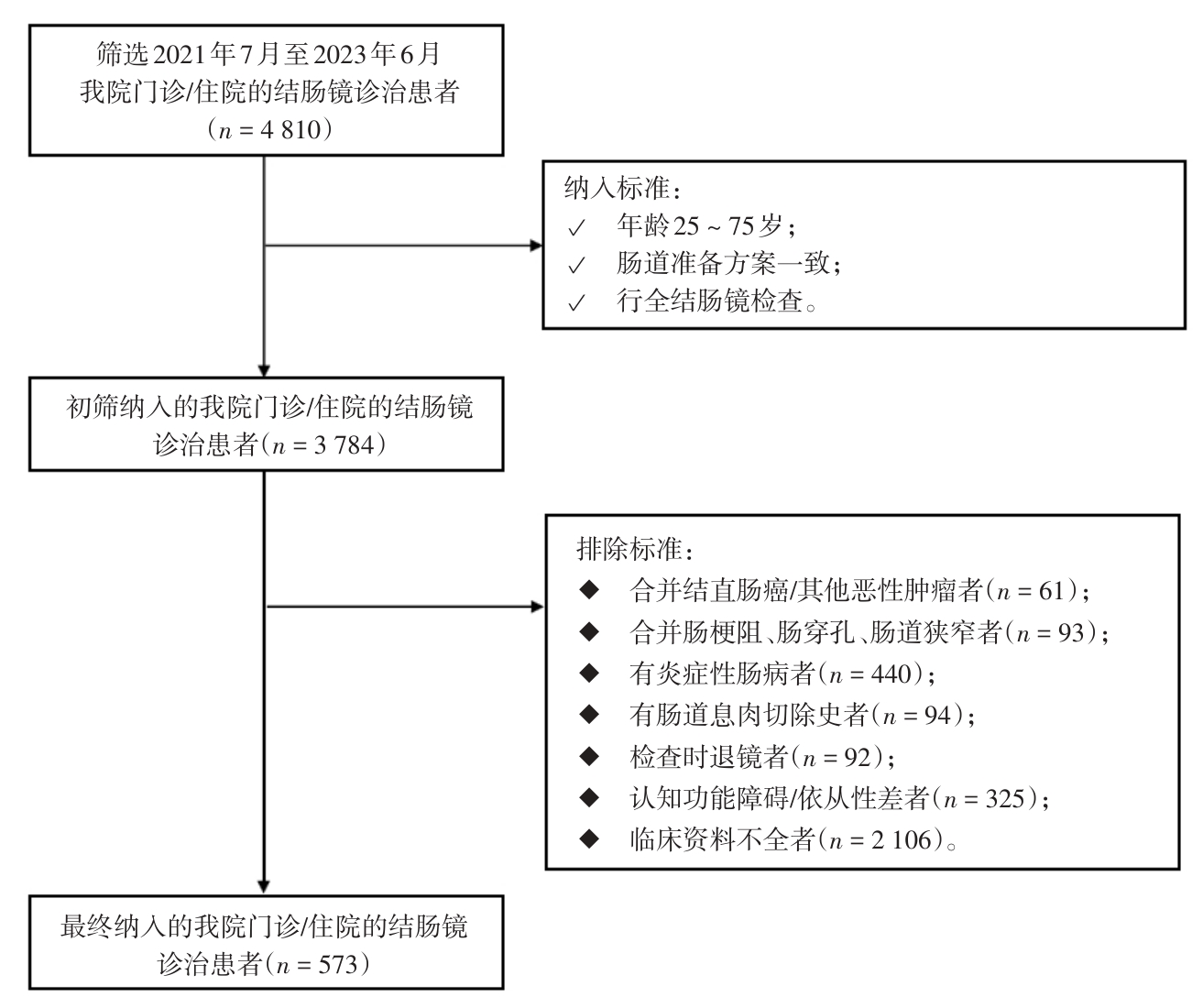
Fig.2
ROC curve analysis of unqualified bowel preparation"
Tab.5
Univariate analysis of minor adverse events after colonoscopy"
| 因素 | 发生组(n = 106) | 未发生组(n = 467) | χ2 值 | P值 |
|---|---|---|---|---|
| 年龄 | 16.262 | < 0.001 | ||
| ≥ 60岁 | 32(30.19) | 65(13.92) | ||
| < 60岁 | 74(69.81) | 402(86.08) | ||
| 性别 | 1.063 | 0.303 | ||
| 男 | 55(51.89) | 268(57.39) | ||
| 女 | 51(48.11) | 199(42.61) | ||
| BMI | 5.942 | 0.015 | ||
| ≥ 28 kg/m2 | 26(24.53) | 69(14.78) | ||
| < 28 kg/m2 | 80(75.47) | 398(85.22) | ||
| 既往史 | ||||
| 吸烟史 | 43(40.57) | 147(31.48) | 3.220 | 0.073 |
| 饮酒史 | 31(29.25) | 139(29.76) | 0.011 | 0.916 |
| 过敏史 | 28(26.42) | 105(22.48) | 0.749 | 0.387 |
| 合并基础疾病数量 | 8.655 | 0.003 | ||
| ≥ 1 | 60(56.60) | 191(40.90) | ||
| 0 | 46(43.40) | 276(59.10) | ||
| 活检/息肉切除术 | 45(42.45) | 131(28.05) | 8.419 | 0.004 |
| 镇静剂 | 5.024 | 0.025 | ||
| 使用 | 39(36.79) | 228(48.82) | ||
| 未使用 | 67(63.21) | 239(51.18) | ||
| 合并用药情况 | ||||
| 阿司匹林 | 47(44.34) | 209(44.75) | 0.006 | 0.938 |
| 华法林 | 19(13.21) | 26(6.00) | 18.229 | < 0.001 |
| NSAID | 17(16.04) | 84(17.99) | 0.226 | 0.634 |
Tab.6
Multivariate analysis of minor adverse events after colonoscopy"
| 变量 | β | SE | Wald | P值 | OR值 | 95%CI |
|---|---|---|---|---|---|---|
| 年龄(≥ 60岁) | 0.905 | 0.261 | 11.968 | 0.001 | 2.471 | 1.480 ~ 4.125 |
| BMI(≥ 28 kg/m2) | 0.489 | 0.276 | 3.134 | 0.077 | 1.630 | 0.949 ~ 2.801 |
| 合并基础疾病数量(≥ 1) | 0.584 | 0.228 | 6.567 | 0.010 | 1.793 | 1.147 ~ 2.802 |
| 活检/息肉切除术(是) | 0.661 | 0.233 | 8.053 | 0.005 | 1.936 | 1.227 ~ 3.055 |
| 镇静剂(使用) | -0.360 | 0.233 | 2.393 | 0.122 | 0.697 | 0.442 ~ 1.101 |
| 合并使用华法林(是) | 1.302 | 0.339 | 14.749 | 0.000 | 3.675 | 1.891 ~ 7.141 |
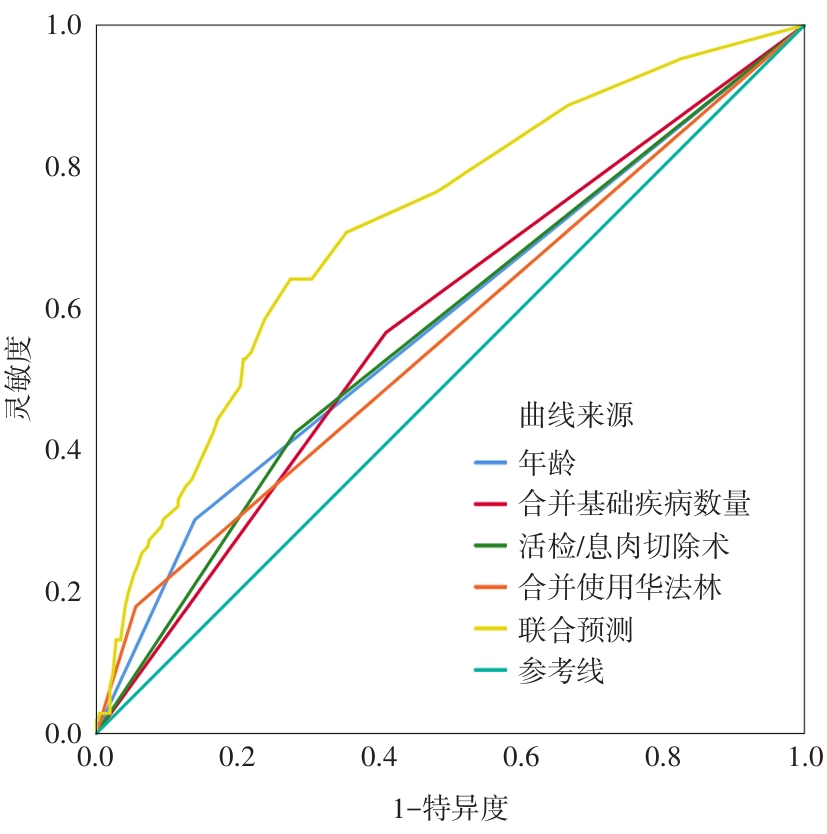
Fig.3
ROC curve of minor adverse events after colonoscopy"
Tab.7
Clinical risk score of unqualified bowel preparation for colonoscopy diagnosis and treatment"
| 自变量 | 条目 | 分值 |
|---|---|---|
| 1 | 年龄(≥ 60岁) | 14 |
| 2 | BMI(≥ 28 kg/m2) | 10 |
| 3 | 便秘史(是) | 18 |
| 4 | 糖尿病(是) | 16 |
| 5 | 合并使用钙拮抗剂药物(是) | 11 |
| 6 | Bristol粪便分型(1 ~ 2型) | 31 |
Tab.8
Clinical risk score table of minor adverse events in bowel preparation for colonoscopy diagnosis and treatment"
| 自变量 | 条目 | 分值 |
|---|---|---|
| 1 | 年龄(≥ 60岁) | 25 |
| 2 | 合并基础疾病数量(≥ 1) | 18 |
| 3 | 活检/息肉切除术(是) | 20 |
| 4 | 合并使用华法林(是) | 37 |
Tab.9
Construction of logistic regression model for two clinical risk scores"
| 变量 | β | SE | Wald | P值 | OR值 | 95%CI |
|---|---|---|---|---|---|---|
| 肠道准备质量临床风险评分 | 0.037 | 0.008 | 20.214 | < 0.001 | 1.038 | 1.021 ~ 1.055 |
| 轻微不良事件临床风险评分 | 0.049 | 0.009 | 29.247 | < 0.001 | 1.051 | 1.032 ~ 1.070 |
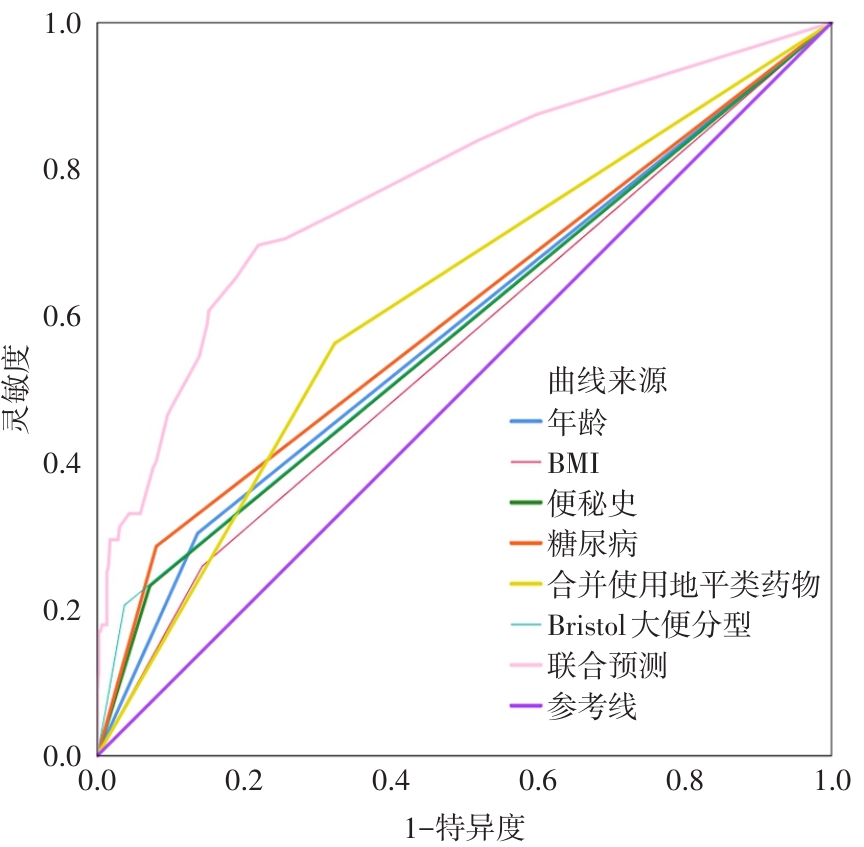
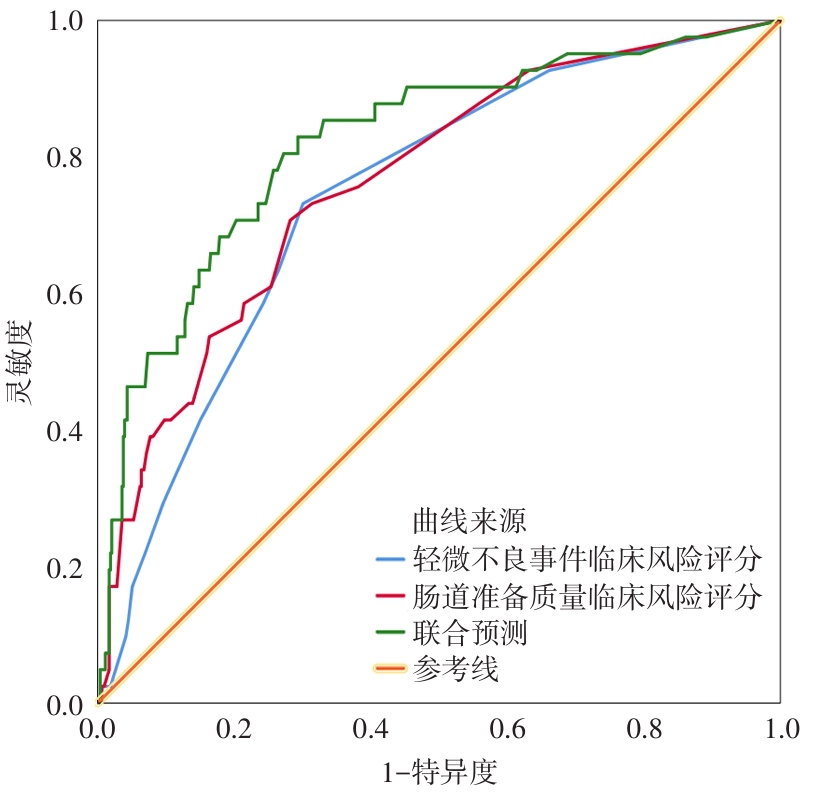
Fig.4
ROC curve of clinical risk score of unqualified bowel preparation and minor adverse events"
| [1] | 吴园园,赵忠艳,夏盛隆,等. 结肠镜检查患者肠道准备合格率及其影响因素[J]. 中国基层医药,2021,28(1):14-18. |
| [2] |
GIMENO-GARCÍA A Z, BENÍTEZ-ZAFRA F, NICOLÁS-PÉREZ D,et al. Colon Bowel Preparation in the Era of Artificial Intelligence: Is There Potential for Enhancing Colon Bowel Cleansing?[J]. Medicina (Kaunas), 2023,59(10):1834. doi:10.3390/medicina59101834
doi: 10.3390/medicina59101834 |
| [3] |
SHAUKAT A, KAHI C J, BURKE C A,et al. ACG Clinical Guidelines: Colorectal Cancer Screening 2021[J]. Am J Gastroenterol,2021,116(3):458-479. doi:10.14309/ajg.0000000000001122
doi: 10.14309/ajg.0000000000001122 |
| [4] |
SEWITCH M J, AZALGARA V M, SING M F. Screening Indication Associated With Lower Likelihood of Minor Adverse Events in Patients Undergoing Outpatient Colonoscopy[J]. Gastroenterol Nurs,2018,41(2):159-164. doi:10.1097/sga.0000000000000308
doi: 10.1097/sga.0000000000000308 |
| [5] | 杨欣,赵大梅,杨艳芹,等. 老年患者结肠镜检查前肠道准备状况及其影响因素调查[J]. 护理实践与研究,2020,17(23):15-17. |
| [6] | 李丹,郭孟然,刘海峰,等. 儿童结肠镜术前肠道准备质量的影响因素[J]. 临床儿科杂志,2020,38(6):438-442. |
| [7] | 高永祥,张晋昕. Logistic回归分析的样本量确定[J]. 循证医学,2018,18(2):122-124. |
| [8] | 刘娅,刘晓晴,杨雪凝,等. 结肠镜检查患者肠道准备失败风险预测模型的构建及验证[J]. 中华护理杂志,2024,59(9):1091-1098. |
| [9] | 中国医师协会内镜医师分会消化内镜专业委员会,中国抗癌协会肿瘤内镜学专业委员会. 中国消化内镜诊疗相关肠道准备指南(2019,上海)[J]. 中华消化内镜杂志,2019,36(7):457-469. |
| [10] |
PARMAR R, MARTEL M, ROSTOM A,et al. Validated Scales for Colon Cleansing: A Systematic Review[J]. Am J Gastroenterol,2016,111(2):197-204. doi:10.1038/ajg.2015.417
doi: 10.1038/ajg.2015.417 |
| [11] |
PAN J, XIN L, MA Y F,et al. Colonoscopy Reduces Colorectal Cancer Incidence and Mortality in Patients With Non-Malignant Findings:A Meta-Analysis[J]. Am J Gastroenterol,2016,111(3):355-365. doi:10.1038/ajg.2015.418
doi: 10.1038/ajg.2015.418 |
| [12] | 杨蕾,杨幼林. 结肠镜检查轻微不良事件危险因素及预防[J]. 医学综述,2020,26(4):762-765. |
| [13] | 王亚军,杨幼林. 结肠镜检查不良事件及处理方法的临床研究进展[J]. 国际消化病杂志,2019,39(5):325-328+340. |
| [14] | 荀林娟,席米娜,宋瑞梅,等. 老年患者结肠镜检查前肠道准备质量的影响因素及护理对策[J]. 临床与病理杂志,2021,41(4):860-865. |
| [15] |
KO C W, RIFFLE S, SHAPIRO J A,et al. Incidence of minor complications and time lost from normal activities after screening or surveillance colonoscopy[J]. Gastrointest Endosc,2007,65(4):648-656. doi:10.1016/j.gie.2006.06.020
doi: 10.1016/j.gie.2006.06.020 |
| [16] |
JOHNSON D A, BARKUN A N, COHEN L B,et al. Optimizing adequacy of bowel cleansing for colonoscopy:Recommendations from the US multi-society task force on colorectal cancer[J]. Gastroenterology,2014,147(4):903-924. doi:10.1053/j.gastro.2014.07.002
doi: 10.1053/j.gastro.2014.07.002 |
| [17] |
BAUDET J S, DIAZ-BETHENCOURT D, AVILÉS J,et al. Minor adverse events of colonoscopy on ambulatory patients:The impact of moderate sedation[J]. Eur J Gastroenterol Hepatol,2009,21(6):656-661. doi:10.1097/meg.0b013e328314b7e3
doi: 10.1097/meg.0b013e328314b7e3 |
| [18] |
BINI E J, FIROOZI B, CHOUNG R J,et al.Systematic evaluation of complications related to endoscopy in a training setting: A prospective 30-day outcomes study[J]. Gastrointest Endosc,2003,57(1):8-16. doi:10.1067/mge.2003.15
doi: 10.1067/mge.2003.15 |
| [19] |
DE JONGE V, SINT NICOLAAS J, VAN BAALEN O,et al. The incidence of 30-day adverse events after colonoscopy among outpatients in the Netherlands[J]. Am J Gastroenterol,2012,107(6):878-884. doi:10.1038/ajg.2012.40
doi: 10.1038/ajg.2012.40 |
| [20] |
DENIS B, GENDRE I, SAULEAU E,et al. Harms of colonoscopy in a colorectal cancer screening programme with faecal occult blood test:A population-based cohort study[J]. Dig Liver Dis,2013,45(6):474-480. doi:10.1016/j.dld.2013.01.006
doi: 10.1016/j.dld.2013.01.006 |
| [21] | 陈栩槿,杨成,朱先兰,等. 结肠镜检查困难程度的患者相关因素分析[J]. 胃肠病学,2023,28(8):455-461. |
| [22] | NGUYEN D L, WIELAND M. Risk factors predictive of poor quality preparation during average risk colonoscopy screening:The importance of health literacy[J]. J Gastrointestin Liver Dis,2010,19(4):369-372. |
| [23] |
MCNABB-BALTAR J, DORREEN A, DHAHAB H AL,et al. Age Is the Only Predictor of Poor Bowel Preparation in the Hospitalized Patient[J]. Can J Gastroenterol Hepatol,2016,2016:2139264. doi:10.1155/2016/2139264
doi: 10.1155/2016/2139264 |
| [24] |
BORG B B, GUPTA N K, ZUCKERMAN G R,et al. Impact of obesity on bowel preparation for colonoscopy[J]. Clin Gastroenterol Hepatol,2009,7(6):670-675. doi:10.1016/j.cgh.2009.02.014
doi: 10.1016/j.cgh.2009.02.014 |
| [25] | 王田田,尤丽丽. 结肠镜检查前肠道准备质量影响因素的Meta分析[J]. 护理研究,2021,35(2):223-230. |
| [26] |
SEO E H, KIM T O, PARK M J,et al. Optimal preparation-to-colonoscopy interval in split-dose PEG bowel preparation determines satisfactory bowel preparation quality:An observational prospective study[J]. Gastrointest Endosc,2012,75(3):583-590. doi:10.1016/j.gie.2011.09.029
doi: 10.1016/j.gie.2011.09.029 |
| [27] | 梁蓉,杨支兰,闫晓晓,等. 老年患者结肠镜检查前肠道准备现状及其影响因素分析[J]. 中国护理管理,2019,19(2):182-187. |
| [28] | 张娜,徐苗苗,张亚峰,等. 结肠镜肠道准备质量受检者影响因素的Meta分析[J]. 护理研究,2023,37(6):963-969. |
| [29] | 黄鸣秋,韩丹,朱怀军,等. 临床药师参与门诊结肠镜检查患者肠道准备不充分预测因素分析及模型建立[J]. 药学与临床研究,2023,31(2):172-176. |
| [30] |
MALHOTRA A, SHAH N, DEPASQUALE J,et al. Use of Bristol Stool Form Scale to predict the adequacy of bowel preparation-a prospective study[J]. Colorectal Dis,2016,18(2):200-204. doi:10.1111/codi.13084
doi: 10.1111/codi.13084 |
| [31] |
WANG C N, YANG R, HOOKEY L. Does It work in Clinical Practice? A Comparison of Colonoscopy Cleansing Effectiveness in Clinical Practice Versus Efficacy from Selected Prospective Trials[J]. J Can Assoc Gastroenterol,2020,3(3):111-119. doi:10.1093/jcag/gwy070
doi: 10.1093/jcag/gwy070 |
| [32] |
MANTA R, TREMOLATERRA F, AREZZO A,et al. Complications during colonoscopy: Prevention,diagnosis,and management[J]. Tech Coloproctol,2015,19(9):505-513. doi:10.1007/s10151-015-1344-z
doi: 10.1007/s10151-015-1344-z |
| [33] |
LEE Y C, WANG H P, CHIU H M,et al. Factors determining post-colonoscopy abdominal pain: Prospective study of screening colonoscopy in 1000 subjects[J]. J Gastroenterol Hepatol,2006,21(10):1575-1580. doi:10.1111/j.1440-1746.2006.04145.x
doi: 10.1111/j.1440-1746.2006.04145.x |
| [34] |
KO C W, RIFFLE S, MICHAELS L,et al. Serious complications within 30 days of screening and surveillance colonoscopy are uncommon[J]. Clin Gastroenterol Hepatol,2010,8(2):166-173. doi:10.1016/j.cgh.2009.10.007
doi: 10.1016/j.cgh.2009.10.007 |
| [35] |
GARDEZI S A, TIBBATTS C. Improving bowel preparation for colonoscopy in a cost effective manner[J]. BMJ Qual Improv Rep,2017,6(1):u204560.w5376. doi:10.1136/bmjquality.u204560.w5376
doi: 10.1136/bmjquality.u204560.w5376 |
| [36] |
ALVAREZ-GONZALEZ M A, PANTALEON M A, FLORES-LE ROUX J A,et al. Randomized Clinical Trial: A Normocaloric Low-Fiber Diet the Day Before Colonoscopy Is the Most Effective Approach to Bowel Preparation in Colorectal Cancer Screening Colonoscopy[J]. Dis Colon Rectum,2019,62(4):491-497. doi:10.1097/dcr.0000000000001305
doi: 10.1097/dcr.0000000000001305 |
| [37] | 林铠浩,蔡伟聪,刘芳江,等. 深圳市社区居民结直肠癌高危人群肠镜检查的依从性及其影响因素[J]. 现代预防医学,2023,50(17):3168-3172. |
| [1] | Jianjun ZHANG,Haipeng WANG,Guangfeng DONG,Ming CHEN,Jinqi LIU,Hao ZHANG,Mingjuan SUN,Meng LU,Huizhuan ZHAI,Xingguang HUANG,Zengjun LI,Dongyang. WANG. A randomized controlled trial on the efficacy of compound polyethylene glycol electrolyte powder combined with linaclotide for bowel preparation in elderly constipated patients before colonoscopy [J]. The Journal of Practical Medicine, 2025, 41(19): 2967-2971. |
| [2] | Fengwei QIN,Jiang LIU,Wen CHEN,Yonghui FENG,Sineng ZHANG. Analysis of influencing factors for early residual low back pain after percutaneous vertebro plasty [J]. The Journal of Practical Medicine, 2025, 41(18): 2884-2889. |
| [3] | Biao LENG,Dequan HONG,Ming TAN,Ming TIAN,Shanliang XIE,Yaoran. TU. Value of serum TFPI-1 combined with NF-κB in prognostic analysis of severe traumatic brain injury [J]. The Journal of Practical Medicine, 2025, 41(16): 2455-2460. |
| [4] | Yi LU,Shilong DAI,Mingjun WANG,Jing ZHOU,Junying HAO,Chen ZHENG,Xinbo XU,Shan DING,Qingsong ZHANG. The relationship between the triglyceride⁃glucose index and its modified index and colorectal cancer: A prospective cohort study [J]. The Journal of Practical Medicine, 2025, 41(15): 2362-2371. |
| [5] | Hongmei FU,Chao. YU. Analysis of the influencing factors for achieving textbook outcomes of liver surgery after laparoscopic liver resection in patients with laparoscopic liver resection for liver lesions [J]. The Journal of Practical Medicine, 2025, 41(10): 1466-1472. |
| [6] | Li LI,Lin. TANG. Analysis of influencing factors of non⁃suicidal self⁃injury behavior and motivation in adult patients with depression [J]. The Journal of Practical Medicine, 2024, 40(4): 466-470. |
| [7] | Min LI,Hongqiang ZHAO,Bin CAO,Lili LIU,Yuzhen BAO,Fengyong. YANG. Logistic regression versus CART decision tree model for predicting pulmonary infection in elderly patients with heart failure with reduced left ventricular ejection fraction [J]. The Journal of Practical Medicine, 2024, 40(23): 3349-3355. |
| [8] | Yuncan WANG,Guangyun CAO,Haibo WU,Na WANG. The relationship between internal carotid artery wall shear stress and carotid plaque neovascularization was evaluated by carotid color ultrasound [J]. The Journal of Practical Medicine, 2024, 40(22): 3232-3237. |
| [9] | Yanping WANG,Wenhui GAO,Yanting WU,Jun YANG,Yi ZHOU,Xiaoshun. JIAN. Analysis of influencing factors on clinical efficacy of neutropenia with febrile neutropenia in tumor patients [J]. The Journal of Practical Medicine, 2024, 40(18): 2597-2601. |
| [10] | Xueyan HU,Fanliang MENG,Juanjuan. DONG. Prognostic analysis of patients with bone metastases from primary non-small cell lung cancer with different pathologic staging [J]. The Journal of Practical Medicine, 2024, 40(16): 2316-2325. |
| [11] | Jia HUANG,Haoxian HUANG,Liji LU,Hengwei. SHENG. Research of difficult airway assessment in patients with obstructive sleep apnea hypopnea syndrome [J]. The Journal of Practical Medicine, 2024, 40(10): 1460-1466. |
| [12] |
XU Yao, XIAO Chaoqun, ZHOU Yanli, LI Juanhua, LIU Fang, WANG Zhijian..
Current status of depression in pregnant women and its influencing factorsin pregnant women [J]. The Journal of Practical Medicine, 2023, 39(4): 493-498. |
| [13] | Yao MENG,Zhao LIU,Jing ZHANG,Changxiao. ZHAO. Comparison of curative effect and prognosis of preserving nipple and areola in patients with breast cancer by different reconstruction operations [J]. The Journal of Practical Medicine, 2023, 39(22): 2903-2908. |
| [14] | Guangdao CHEN,Saiddin Aziz.. Diagnostic value and influencing factors of Xpert MTB/RIF assay for active tuberculosis in children [J]. The Journal of Practical Medicine, 2023, 39(19): 2440-2445. |
| [15] | GU Yicen , WANG Yuhao, JING Ru, PENG Jinbi, HAN Yuhao, YANG Daoyu, QUAN Ningbin, LI Xudong. . Current status and influencing factors of hesitation of occupational pneumoconiosis patients on Covid ⁃ 19 vaccination in Guangdong Province [J]. The Journal of Practical Medicine, 2023, 39(15): 1974-1981. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||