

The Journal of Practical Medicine ›› 2025, Vol. 41 ›› Issue (10): 1555-1562.doi: 10.3969/j.issn.1006-5725.2025.10.018
• Clinical Research • Previous Articles
Jun LIU,Fulin TIAN,Lin CHEN,Jian. LI
Received:2024-12-25
Online:2025-05-25
Published:2025-05-21
CLC Number:
Jun LIU,Fulin TIAN,Lin CHEN,Jian. LI. The relationship between normal high blood pressure and grade 1 hypertension in early pregnancy and maternal preeclampsia and adverse pregnancy outcomes[J]. The Journal of Practical Medicine, 2025, 41(10): 1555-1562.
Tab.1
General information of pregnant women"
| 项目 | 血压正常(n = 2 029) | 正常高值血压(n = 375) | 1级高血压(n = 158) | F/χ2 值 | P值 |
|---|---|---|---|---|---|
| 年龄/岁 | 28.02 ± 5.49 | 28.13 ± 5.82 | 28.26 ± 5.99 | 0.270 | 0.763 |
| 孕前体质量指数/(kg/m2) | 25.54 ± 5.98 | 30.79 ± 7.46* | 32.32 ± 8.04*# | 46.244 | < 0.001 |
| 孕期体质量增加/kg | 12.01 ± 5.08 | 13.19 ± 5.64 | 14.53 ± 6.07 | 9.821 | < 0.001 |
| 民族(汉族)/[例(%)] | 2 008(98.97) | 370(98.67) | 155(98.12) | 1.136 | 0.567 |
| 婚姻状况(已婚)/[例(%)] | 1 983(97.73) | 364(97.07) | 151(95.57) | 3.158 | 0.206 |
| 高血压家族史/[例(%)] | 61(3.01) | 14(3.73) | 12(7.59) | 9.561 | 0.008 |
| 妊娠期糖尿病/[例(%)] | 66(3.25) | 15(4.00) | 8(5.06) | 1.796 | 0.407 |
| 既往PE史/[例(%)] | 7(0.34) | 3(0.80) | 2(1.27) | 3.702 | 0.157 |
| 初孕产妇/[例(%)] | 1 623(79.99) | 294(78.40) | 126(79.75) | 0.495 | 0.781 |
| 流产史/[例(%)] | 103(5.08) | 18(4.80) | 7(4.43) | 0.164 | 0.921 |
| 早产史/[例(%)] | 20(0.99) | 4(1.07) | 2(1.27) | 0.126 | 0.939 |
| 辅助生育治疗史/[例(%)] | 101(4.98) | 18(4.80) | 8(5.06) | 0.025 | 0.988 |
| 孕次 | 1.86 ± 0.32 | 1.91 ± 0.44 | 1.98 ± 0.37 | 4.110 | 0.017 |
| 产次 | 0.92 ± 0.13 | 1.06 ± 0.28 | 1.22 ± 0.34 | 59.076 | < 0.001 |
| 产前检查/次 | 5.13 ± 1.89 | 5.22 ± 2.01 | 8.13 ± 2.24 | 120.084 | < 0.001 |
| SBP/mmHg | 109.73 ± 6.78 | 128.34 ± 7.16 | 148.13 ± 7.66 | 226.605 | < 0.001 |
| DBP/mmHg | 66.92 ± 5.98 | 85.82 ± 4.03 | 94.33 ± 4.08 | 486.250 | < 0.001 |
Tab.2
Comparison of PE and adverse pregnancy outcomes among women with different blood pressure levels in early pregnancy"
| 项目 | 血压正常(n = 2 029) | 正常高值血压(n = 375) | 1级高血压(n = 158) | χ2值 | P值 |
|---|---|---|---|---|---|
| PE | 76(3.75) | 29(7.73) | 22(13.92) | 39.420 | < 0.001 |
| 剖宫产 | 624(30.75) | 112(29.87) | 66(41.77) | 8.697 | 0.013 |
| 胎盘早剥 | 39(1.92) | 17(4.53) | 13(8.23) | 27.917 | < 0.001 |
| 自发性早产(37周前分娩) | 81(3.99) | 18(4.80) | 9(5.70) | 1.426 | 0.490 |
| 产后出血 | 131(6.46) | 26(6.93) | 12(7.59) | 0.389 | 0.823 |
| 孕20周后死胎 | 6(0.30) | 3(0.08) | 1(0.63) | 2.325 | 0.313 |
| 阿氏评分< 7 | 24(1.18) | 6(1.60) | 11(6.96) | 31.090 | < 0.001 |
| 新生儿入住NICU | 257(12.67) | 54(14.40) | 22(13.92) | 0.969 | 0.616 |
| 小于胎龄儿 | 209(10.30) | 38(10.13) | 16(10.12) | 0.013 | 0.994 |
| 巨大儿 | 194(9.56) | 36(9.60) | 16(10.13) | 0.054 | 0.973 |
| 出生28 d内死亡 | 6(0.30) | 1(0.27) | 1(0.63) | 0.565 | 0.754 |
Tab.3
Cox regression variable assignment table"
| 变量 | 赋值 | |
|---|---|---|
| 因变量 | ||
| PE | 否 = 0,是 = 1 | |
| 剖宫产 | 否 = 0,是 = 1 | |
| 胎盘早剥 | 否 = 0,是 = 1 | |
| 阿氏评分<7 | 否 = 0,是 = 1 | |
| 自发性早产 | 否 = 0,是 = 1 | |
| 产后出血 | 否 = 0,是 = 1 | |
| 孕20周后死胎 | 否 = 0,是 = 1 | |
| 新生儿入住NICU | 否 = 0,是 = 1 | |
| 小于胎龄儿 | 否 = 0,是 = 1 | |
| 巨大儿 | 否 = 0,是 = 1 | |
| 出生28 d内死亡 | 否 = 0,是 = 1 | |
| 自变量 | ||
| 正常高值血压* | 否 = 0,是 = 1 | |
| 1级高血压# | 否 = 0,是 = 1 | |
| 年龄/岁 | < 35 = 0,≥ 35 = 1 | |
| 孕期体质量增加/kg | < 10 = 0,≥ 10 = 1 | |
| 婚姻状况 | 未婚、丧偶、离异、分居 = 0,已婚 = 1 | |
| 妊娠期糖尿病 | 否 = 0,是 = 1 | |
| 初孕产妇 | 否 = 0,是 = 1 | |
| 早产史 | 否 = 0,是 = 1 | |
| 孕次 | ≤ 2 = 0,≥ 3 = 1 | |
| 产前检查/次 | ≤ 5 = 0,≥ 6 = 1 | |
| 孕前体质量指数/(kg/m2) | < 24 = 0,≥ 24 = 1 | |
| 民族 | 少数民族 = 0,汉族 = 1 | |
| 高血压家族史 | 否 = 0,是 = 1 | |
| 既往PE史 | 否 = 0,是 = 1 | |
| 流产史 | 否 = 0,是 = 1 | |
| 辅助生育治疗史 | 否 = 0,是 = 1 | |
| 产次 | ≤ 2 = 0,≥ 3 = 1 | |
Tab.4
Cox regression analysis of the effects of normal high blood pressure and primary blood pressure on women's PE and adverse pregnancy outcomes"
| 样本组合 | 因变量 | 自变量 | β | SE | Wald χ2 | P值 | HR | 95%CI |
|---|---|---|---|---|---|---|---|---|
| 组合(1) | PE | 正常高值血压 | 0.771 | 0.289 | 7.141 | 0.007 | 2.163 | 1.228 ~ 3.809 |
| 剖宫产 | 正常高值血压 | 0.293 | 0.475 | 0.380 | 0.537 | 1.341 | 0.528 ~ 3.405 | |
| 胎盘早剥 | 正常高值血压 | 0.015 | 0.047 | 0.109 | 0.740 | 1.016 | 0.925 ~ 1.115 | |
| 自发性早产 | 正常高值血压 | 0.026 | 0.053 | 0.249 | 0.617 | 1.027 | 0.925 ~ 1.140 | |
| 产后出血 | 正常高值血压 | 0.131 | 0.136 | 0.932 | 0.334 | 1.141 | 0.873 ~ 1.491 | |
| 孕20周后死胎 | 正常高值血压 | 0.243 | 0.134 | 3.275 | 0.070 | 1.276 | 0.980 ~ 1.661 | |
| 阿氏评分< 7 | 正常高值血压 | 0.352 | 0.192 | 3.361 | 0.066 | 1.422 | 0.976 ~ 2.071 | |
| 新生儿入住NICU | 正常高值血压 | 0.263 | 0.335 | 0.614 | 0.432 | 1.301 | 0.674 ~ 2.511 | |
| 小于胎龄儿 | 正常高值血压 | 0.085 | 0.082 | 1.076 | 0.299 | 1.089 | 0.927 ~ 1.279 | |
| 巨大儿 | 正常高值血压 | 0.289 | 0.246 | 1.380 | 0.240 | 1.336 | 0.824 ~ 2.166 | |
| 出生28 d内死亡 | 正常高值血压 | 0.242 | 0.167 | 2.101 | 0.147 | 1.275 | 0.918 ~ 1.770 | |
| 组合(2) | PE | 1级高血压 | 1.343 | 0.400 | 11.272 | < 0.001 | 3.829 | 1.749 ~ 8.385 |
| 剖宫产 | 1级高血压 | 0.881 | 0.317 | 7.752 | 0.005 | 2.414 | 1.298 ~ 4.489 | |
| 胎盘早剥 | 1级高血压 | 0.931 | 0.384 | 5.881 | 0.015 | 2.537 | 1.196 ~ 5.384 | |
| 自发性早产 | 1级高血压 | 0.339 | 0.345 | 0.963 | 0.326 | 1.404 | 0.713 ~ 2.764 | |
| 产后出血 | 1级高血压 | 0.211 | 0.194 | 1.192 | 0.274 | 1.236 | 0.845 ~ 1.807 | |
| 孕20周后死胎 | 1级高血压 | 0.073 | 0.089 | 0.662 | 0.415 | 1.076 | 0.902 ~ 1.283 | |
| 阿氏评分< 7 | 1级高血压 | 0.604 | 0.274 | 4.852 | 0.027 | 1.829 | 1.069 ~ 3.130 | |
| 新生儿入住NICU | 1级高血压 | 0.297 | 0.220 | 1.809 | 0.178 | 1.346 | 0.873 ~ 2.075 | |
| 小于胎龄儿 | 1级高血压 | 0.348 | 0.217 | 2.578 | 0.108 | 1.417 | 0.926 ~ 2.168 | |
| 巨大儿 | 1级高血压 | 0.211 | 0.344 | 0.375 | 0.539 | 1.235 | 0.629 ~ 2.424 | |
| 出生28 d内死亡 | 1级高血压 | 0.345 | 0.273 | 1.592 | 0.206 | 1.414 | 0.826 ~ 2.417 |
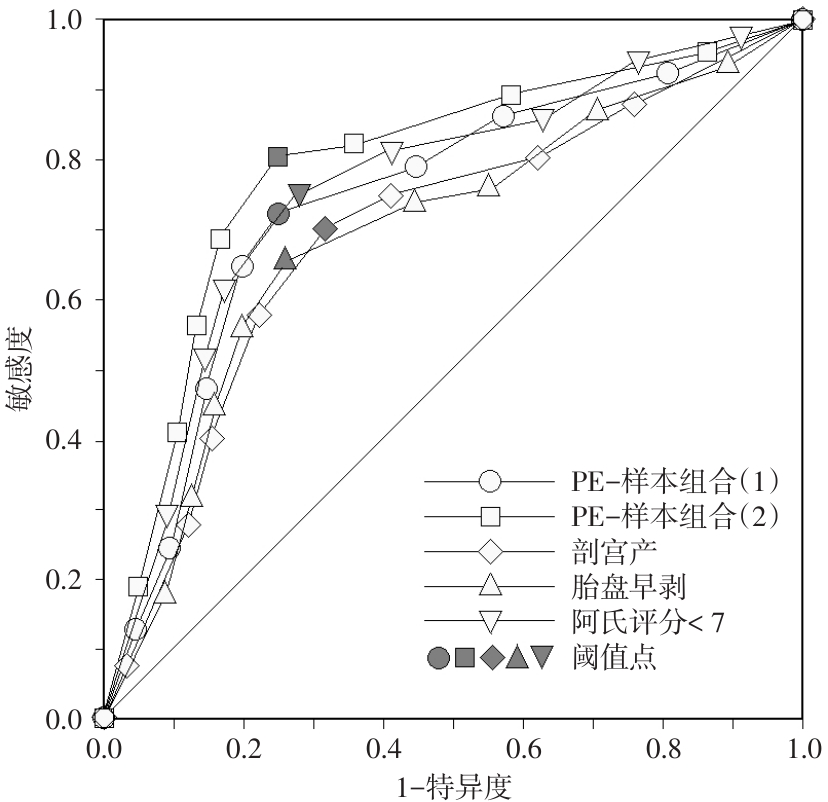
Tab.5
Prediction and evaluation value of early pregnancy blood pressure values for PE and adverse pregnancy outcomes in women-ROC analysis results"
| 预测目标 | AUC(95%CI) | 阈值(自变量SBP/DBP) | 灵敏度 | 特异度 | 约登指数 | 准确度 |
|---|---|---|---|---|---|---|
| PE(1) | 0.757(0.553 ~ 0.942) | 139/89 | 0.725 | 0.752 | 0.477 | 0.748 |
| PE(2) | 0.789(0.634 ~ 0.937) | 159/99 | 0.810 | 0.752 | 0.562 | 0.756 |
| 剖宫产 | 0.717(0.496 ~ 0.914) | 159/99 | 0.703 | 0.683 | 0.386 | 0.684 |
| 胎盘早剥 | 0.709(0.474 ~ 0.935) | 159/99 | 0.665 | 0.735 | 0.400 | 0.730 |
| 阿氏评分< 7 | 0.742(0.519 ~ 0.947) | 159/99 | 0.747 | 0.722 | 0.469 | 0.724 |
Fig.1
ROC analysis curve"
| 1 | 吕燕宇, 张兵, 王惠君, 等. 1991-2015年我国9省成年农民高血压患病率、知晓率和治疗率的变化趋势及人口经济学差异[J]. 中华流行病学杂志, 2020, 41(4): 498-503. |
| 2 |
BERHE A K, ILESANMI A O, AIMAKHU C O, et al. Effect of pregnancy induced hypertension on adverse perinatal outcomes in Tigray regional state, Ethiopia: A prospective cohort study[J]. BMC Pregnancy Childbirth, 2019, 20(1): 7. doi:10.1186/s12884-019-2708-6
doi: 10.1186/s12884-019-2708-6 |
| 3 |
TENÓRIO M B, FERREIRA R C, MOURA F A, et al. Cross-Talk between Oxidative Stress and Inflammation in Preeclampsia[J]. Oxid Med Cell Longev, 2019,2019: 8238727. doi:10.1155/2019/8238727
doi: 10.1155/2019/8238727 |
| 4 | 谢幸, 孔北华, 段涛. 妇产科学[M]. 北京: 人民卫生出版社, 2018. |
| 5 | 《中国高血压防治指南》修订委员会. 中国高血压防治指南2018年修订版[J]. 心脑血管病防治, 2019, 19(1): 1-44. |
| 6 | 赵睿学, 王停, 荆鲁, 等. 基于国内外新版高血压指南探讨高血压前期存在的问题与思考[J]. 实用心脑肺血管病杂志, 2022, 30(1): 1-5. |
| 7 |
YANO Y, REIS J P, COLANGELO L A, et al. Association of Blood Pressure Classification in Young Adults Using the 2017 American College of Cardiology/American Heart Association Blood Pressure Guideline With Cardiovascular Events Later in Life [J]. JAMA, 2018, 320(17): 1774-1782. doi:10.1001/jama.2018.13551
doi: 10.1001/jama.2018.13551 |
| 8 | 中华医学会妇产科学分会妊娠期高血压疾病学组. 妊娠期高血压疾病诊治指南(2015)[J]. 中华围产医学杂志, 2016, 19(3): 161-169. |
| 9 | 肖燕璇, 张立力, 黎嘉琪,等. 单胎子痫前期孕妇产前体质量指数与母婴结局关系探讨[J]. 实用医学杂志, 2023, 39(18): 2357-2361. |
| 10 | 王红,王静,申春华,等. 6892例高龄孕产妇不良妊娠结局危险因素分析[J]. 热带医学杂志,2019,19(2):226-228. |
| 11 | 季燕雯, 陈先侠, 王海霞, 等. 早发型子痫前期不良妊娠结局的影响因素分析[J]. 实用医学杂志, 2020, 36(12): 1590-1594. |
| 12 | 徐美春, 吕玲, 高冬霞. 心理压力、妊娠压力和慢性高血压及三者结合对子痫前期风险发病的评估[J]. 医学综述, 2015, 21(12): 2302-2303. |
| 13 |
HE D, WU S, ZHAO H, et al. High normal blood pressure in early pregnancy also contribute to early onset preeclampsia and severe preeclampsia[J]. Clin Exp Hypertens, 2018, 40(6): 539-546. doi:10.1080/10641963.2017.1407330
doi: 10.1080/10641963.2017.1407330 |
| 14 |
NOBLES C J, MENDOLA P, MUMFORD S L, et al. Preconception Blood Pressure and Its Change Into Early Pregnancy: Early Risk Factors for Preeclampsia and Gestational Hypertension[J]. Hypertension, 2020, 76(3): 922-929. doi:10.1161/hypertensionaha.120.14875
doi: 10.1161/hypertensionaha.120.14875 |
| 15 |
UEDA A, HASEGAWA M, MATSUMURA N, et al. Lower systolic blood pressure levels in early pregnancy are associated with a decreased risk of early-onset superimposed preeclampsia in women with chronic hypertension: A multicenter retrospective study[J]. Hypertens Res, 2022 .45(1): 135-145. doi:10.1038/s41440-021-00763-6
doi: 10.1038/s41440-021-00763-6 |
| 16 |
ZHU J, ZHANG J, NG M J, et al. Angiogenic factors during pregnancy in Asian women with elevated blood pressure in early pregnancy and the risk of preeclampsia: A longitudinal cohort study[J].BMJ Open, 2019, 9(11): e032237. doi:10.1136/bmjopen-2019-032237
doi: 10.1136/bmjopen-2019-032237 |
| 17 | 黄杨, 孟琳, 吕慧, 等. 血清PIGF、sFlt-1及PLGF水平对妊娠期高血压的预测效能及与子痫前期发病的关系[J]. 广东医学, 2023, 44(3): 284-287. |
| 18 |
NOBLES C J, MENDOLA P, MUMFORD S L, et al. Preconception Blood Pressure and Its Change Into Early Pregnancy: Early Risk Factors for Preeclampsia and Gestational Hypertension [J]. Hypertension, 2020, 76(3): 922-929. doi:10.1161/hypertensionaha.120.14875
doi: 10.1161/hypertensionaha.120.14875 |
| 19 |
WU Y, MA Y, WU K, et al. Blood pressure in early and mid-pregnancy and the risk of small-for-gestational-age birth: Findings of a large cohort study in China[J]. J Hum Hypertens, 2019, 33(6): 475-481. doi:10.1038/s41371-018-0150-2
doi: 10.1038/s41371-018-0150-2 |
| 20 |
LI Q, ZHENG L, GU Y, et al. Early pregnancy stage 1 hypertension and high mean arterial pressure increased risk of adverse pregnancy outcomes in Shanghai, China[J]. J Hum Hypertens, 2022, 36(10): 917-924. doi:10.1038/s41371-021-00523-6
doi: 10.1038/s41371-021-00523-6 |
| 21 |
HEIMBERGER S, PERDIGAO J L, MUELLER A, et al. Effect of blood pressure control in early pregnancy and clinical outcomes in African American women with chronic hypertension[J]. Pregnancy Hypertens, 2020, 20: 102-107. doi:10.1016/j.preghy.2020.03.008
doi: 10.1016/j.preghy.2020.03.008 |
| 22 |
MA S, WU L, YU Q, et al. Associations Between Trajectory of Different Blood Pressure Components in Pregnancy and Risk of Adverse Birth Outcomes - A Real World Study[J]. Risk Manag Healthc Policy, 2021, 14: 3255-3263. doi:10.2147/rmhp.s318956
doi: 10.2147/rmhp.s318956 |
| 23 |
MA Y, ZHANG X, CHE Q, et al. Reference ranges and trajectories for blood pressure in pregnancy: Findings from a follow-up study based on China Maternal and Newborn's Health Monitoring System[J]. Hypertens Pregnancy, 2020, 39(2): 117-125. doi:10.1080/10641955.2020.1742350
doi: 10.1080/10641955.2020.1742350 |
| 24 |
GUNDERSON E P, GREENBERG M, NGUYEN-HUYNH M N, et al. Early Pregnancy Blood Pressure Patterns Identify Risk of Hypertensive Disorders of Pregnancy Among Racial and Ethnic Groups[J]. Hypertension, 2022, 79(3): 599-613. doi:10.1161/hypertensionaha.121.18568
doi: 10.1161/hypertensionaha.121.18568 |
| 25 |
CÔTÉ M, BOUTIN A, GASSE C, et al. First Trimester Mean Arterial Pressure Measured Manually Versus Using an Automated Device and the Prediction of Preeclampsia: A Case-Cohort Study [J]. J Obstet Gynaecol Can, 2020, 42(3): 277-283. doi:10.1016/j.jogc.2019.06.017
doi: 10.1016/j.jogc.2019.06.017 |
| 26 | 王小兰, 杨舒盈, 曾雪英, 等. 孕期血压控制水平对轻中度慢性高血压孕妇妊娠结局的影响[J]. 中华高血压杂志, 2021, 29(3): 268-271. |
| 27 |
LIN L, ZHU Y, LI B, et al. Low-dose aspirin in the prevention of pre-eclampsia in China (APPEC study): Protocol for a multicentre randomized controlled trial[J]. Trials, 2018, 19(1): 608. doi:10.1186/s13063-018-2970-3
doi: 10.1186/s13063-018-2970-3 |
| 28 |
SHARMA S, SKOG J, TIMPKA S, et al. Preeclampsia and high blood pressure in early pregnancy as risk factors of severe maternal cardiovascular disease during 50-years of follow-up[J]. Pregnancy Hypertens, 2021, 26: 79-85. doi:10.1016/j.preghy.2021.09.005
doi: 10.1016/j.preghy.2021.09.005 |
| [1] | Yunting ZHUANG,Yao SONG,Qian CHEN,Yanxuan XIAO,Tian TAN,Wenhui LI,Ruiyan BAI,Zeshan LIN,Zhijian. WANG. Risk factor analysis and predictive indicators of postpartum haemorrhage in singleton pregnant women with severe preeclampsia [J]. The Journal of Practical Medicine, 2025, 41(8): 1155-1160. |
| [2] | Runfang WANG,Ya DUAN,Liyan DU,Xiaodan LIU,Wenning LIAN,Yan HUO,Dandan. YANG. Epidemiological status and risk factors associated with placental abruption among pregnant women in Hebei Province [J]. The Journal of Practical Medicine, 2025, 41(6): 904-910. |
| [3] | Zhaohua YAN,Jianbin ZHENG,Na ZHANG,Chunyan CAO,Luchun. YAN. MiR⁃365a⁃3p affects vascular endothelial cell function through TGF⁃β signaling pathway and participates in the pathogenesis of preeclampsia [J]. The Journal of Practical Medicine, 2024, 40(16): 2263-2269. |
| [4] | Sumei YU,Yuyue ZHANG,Liwen MA,Yuanjun KUANG,Qingning CHANG,Min KONG,ZHANG Huiping ZHANGx. Effect of miR⁃15a⁃5p on autophagy of placental trophoblasts in preeclampsia [J]. The Journal of Practical Medicine, 2024, 40(12): 1631-1636. |
| [5] | Xiaoying DAI,Ya SHEN,Xiaofang. TAN. Influencing factors of early miscarriage after recurrent spontaneous abortion based on ultrasound endometrial receptivity parameters and lymphocyte immunophenotype [J]. The Journal of Practical Medicine, 2024, 40(10): 1402-1406. |
| [6] | Weiwei HU,Xiaorong LI,Chunhui TIAN,Zhifen LIU,Junqi. YING. Effect of telmisartan combined with calcium dobesilate on hypertensive patients with type 2 diabetes mellitus on the blood pressure rhythm [J]. The Journal of Practical Medicine, 2023, 39(19): 2534-2540. |
| [7] | Yanxuan XIAO,Lili ZHANG,Jiaqi LI,Yunting ZHUANG,Yao SONG,Wenhui LI,Tian TAN,Haitao CHEN,Zhijian. WANG. Relationship between prenatal body mass index and pregnancy outcomes in singleton pregnant women with preeclampsia [J]. The Journal of Practical Medicine, 2023, 39(18): 2357-2361. |
| [8] | Lijun JIANG,Qian YU,Fudong WANG,Mingfu WU,Zhifeng LIU,Longfeng ZHANG,Libing. ZHANG. The role of blood pressure variability indicators combined with cerebral blood flow parameters in predicting intraventricular hemorrhage in very low birth weight preterm infants [J]. The Journal of Practical Medicine, 2023, 39(16): 2116-2121. |
| [9] | CAI Yanli, ZHU Jinming, ZHANG Yuehui, LUAN Xiaomei, PENG Fengyun, LI Qing, DU Changjiang. . Expression of SCUBE2 in serum and placental tissues of pregnant women with preeclampsia and its clini⁃ calsignificance [J]. The Journal of Practical Medicine, 2023, 39(12): 1518-1523. |
| [10] |
GAO Li′na, DONG Yan, HE Xiaochun, ZHANG Yufang, LIU Xiaoling, HAO Mao, ZHANG Li, LIU Xiaohui..
Effects of circular RNA circAAS on invasion and migration of human chorionic trophoblast cells [J]. The Journal of Practical Medicine, 2022, 38(17): 2151-2157. |
| [11] |
ZHANG Qiaoyun, LI Rui..
Effect of intraoperative blood pressure management on early postoperative acute kidney injury in elderly patients undergoing major abdominal surgery [J]. The Journal of Practical Medicine, 2021, 37(7): 894-898. |
| [12] |
WU Qirui, WANG Yanhua, LIU Linying, GAO Li′ na, YIN He, ZHANG Yuyue, HAN Kedong, ZHANG Huiping.
Role of miR ⁃488⁃3p in invasion and migration of trophoblast cells in preeclampsia placenta [J]. The Journal of Practical Medicine, 2021, 37(5): 601-605. |
| [13] |
CAO Dan, TANG Xiaofang, LI Minhui.
miR ⁃ 155 ⁃ 5p influences the occurrence of preeclampsia through targeted inhibition of Sirt1 [J]. The Journal of Practical Medicine, 2021, 37(4): 451-457. |
| [14] |
ZHANG Ziqu, LIU Yong, LI Jing⁃ wei, WANG Yali, ZHAI Yujun..
Effect of amlodipine ⁃ benazepril tablets on ambulatory blood pressure of grade 2 essential hypertension patients uncontrolled by free combination of two antihypertensive drugs #br#
#br#
[J]. The Journal of Practical Medicine, 2021, 37(18): 2375-2379.
|
| [15] |
PENG Yongbao, ZHANG Liqiong, LIU Huai. .
Relationship between the expression of HSP70 in umbilical artery blood and fetal birth status and short ⁃ term prognosis in patients with different types of severe preeclampsia [J]. The Journal of Practical Medicine, 2021, 37(16): 2084-2088. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||