

The Journal of Practical Medicine ›› 2025, Vol. 41 ›› Issue (3): 358-364.doi: 10.3969/j.issn.1006-5725.2025.03.008
• Clinical Research • Previous Articles
Youqiang ZHANG,Ling YAN( ),Wei LIAO,Guang WANG,Xiaoheng CHEN,Rui FAN,Zuwei. LIU
),Wei LIAO,Guang WANG,Xiaoheng CHEN,Rui FAN,Zuwei. LIU
Received:2024-06-09
Online:2025-02-10
Published:2025-02-19
Contact:
Ling YAN
E-mail:13017405609@163.com
CLC Number:
Youqiang ZHANG,Ling YAN,Wei LIAO,Guang WANG,Xiaoheng CHEN,Rui FAN,Zuwei. LIU. Study of modified anteromedial approach and preserves the superior extensor retinaculum for clinical effect of Pilon fracture[J]. The Journal of Practical Medicine, 2025, 41(3): 358-364.
Tab.1
Comparison of operation time, intraoperative blood loss and postoperative diversion of the two groups"
| 参数 | 观察组 (n = 27) | 对照组 (n = 29) | t值 | P值 |
|---|---|---|---|---|
| 手术时间/min | 115.92 ± 12.23 | 172.75 ± 15.09 | 9.280 | < 0.01 |
| 术中失血量/mL | 129.25 ± 16.15 | 177.24 ± 14.36 | 11.762 | < 0.01 |
| 术后引流量/mL | 82.44 ± 25.57 | 115.06 ± 21.95 | 5.133 | < 0.01 |
Tab.2
Comparison of pain VAS scores between the two groups"
| 参数 | 观察组 (n = 27) | 对照组 (n = 29) | t值 | P值 |
|---|---|---|---|---|
| 术后3 d | 6.00 ± 1.49 | 6.86 ± 1.24 | 2.352 | 0.022 |
| 术后1周 | 4.70 ± 1.20 | 5.41 ± 1.24 | 2.172 | 0.034 |
| 术后4周 | 2.07 ± 1.26 | 2.45 ± 1.32 | 2.702 | 0.009 |
Tab.3
Comparison of fracture reduction in the two groups"
| 参数 | 观察组 (n = 27) | 对照组 (n = 29) | χ2值 | P值 |
|---|---|---|---|---|
| 解剖复位/例 | 18 | 17 | ||
| 复位可/例 | 8 | 10 | ||
| 复位差/例 | 1 | 2 | ||
| 复位优良率 | 26(96.29) | 27(93.10) | ||
| 解剖复位率 | 18(66.67) | 17(58.62) | 0.386 | 0.534 |
Tab.4
Comparison of fracture reduction in the two groups"
| 参数 | 观察组 (n = 27) | 对照组 (n = 29) | χ 2 值 | P值 |
|---|---|---|---|---|
| 皮肤浅表坏死、感染 | 1 | 5 | ||
| 深部软组织感染 | 0 | 2 | ||
| 骨髓炎 | 0 | 1 | ||
| 创伤性关节炎 | 1 | 2 | ||
| 合计/[例(%)] | 2(7.7) | 10(34.4) | 4.586 | 0.032 |
Tab.5
Comparison of ankle joint function at 3,6 and"
| 项目 | 观察组 (n = 27) | 对照组 (n = 29) | F值 | P值 |
|---|---|---|---|---|
| 术后3个月 | 79.66 ± 6.64 | 73.93 ± 8.58 | 6.363 | 0.015* |
| 术后6个月 | 85.59 ± 7.26 | 81.41 ± 7.22 | 5.679 | 0.021* |
| 术后12个月 | 89.78 ± 7.97 | 86.83 ± 8.94 | 4.780 | 0.033* |

Fig.1
Preoperative anterolateral and lateral radiography and CT of the ankle joint"
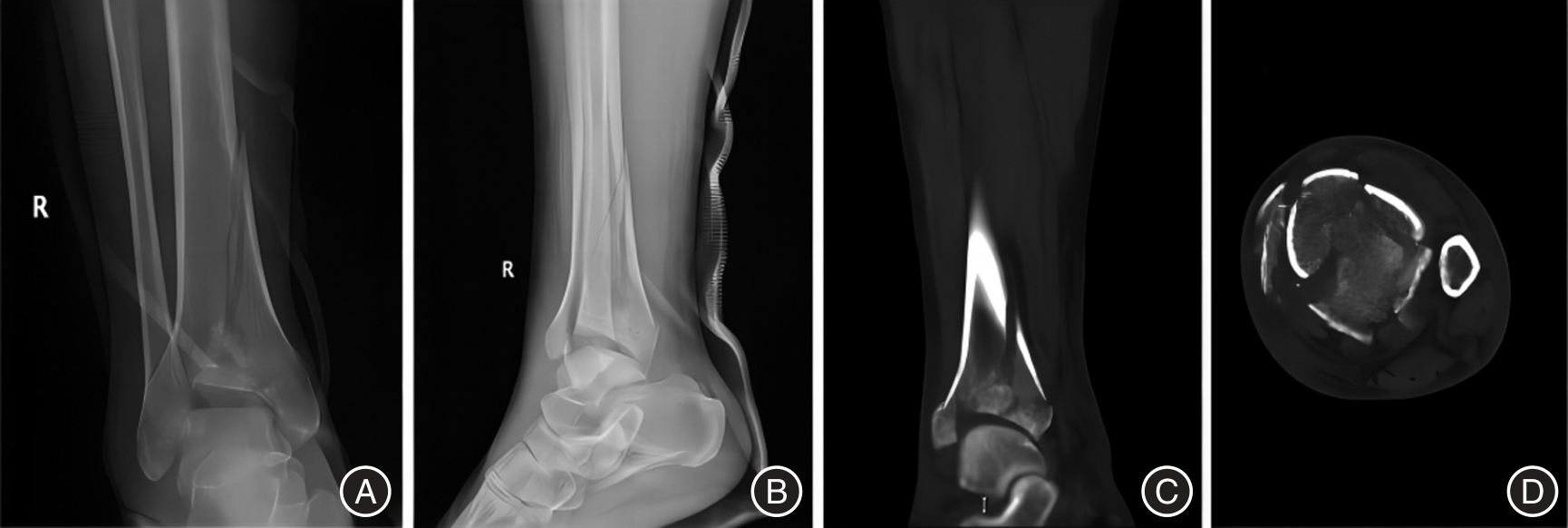

Fig.2
Intraoperative and postoperative X-ray reexamination"
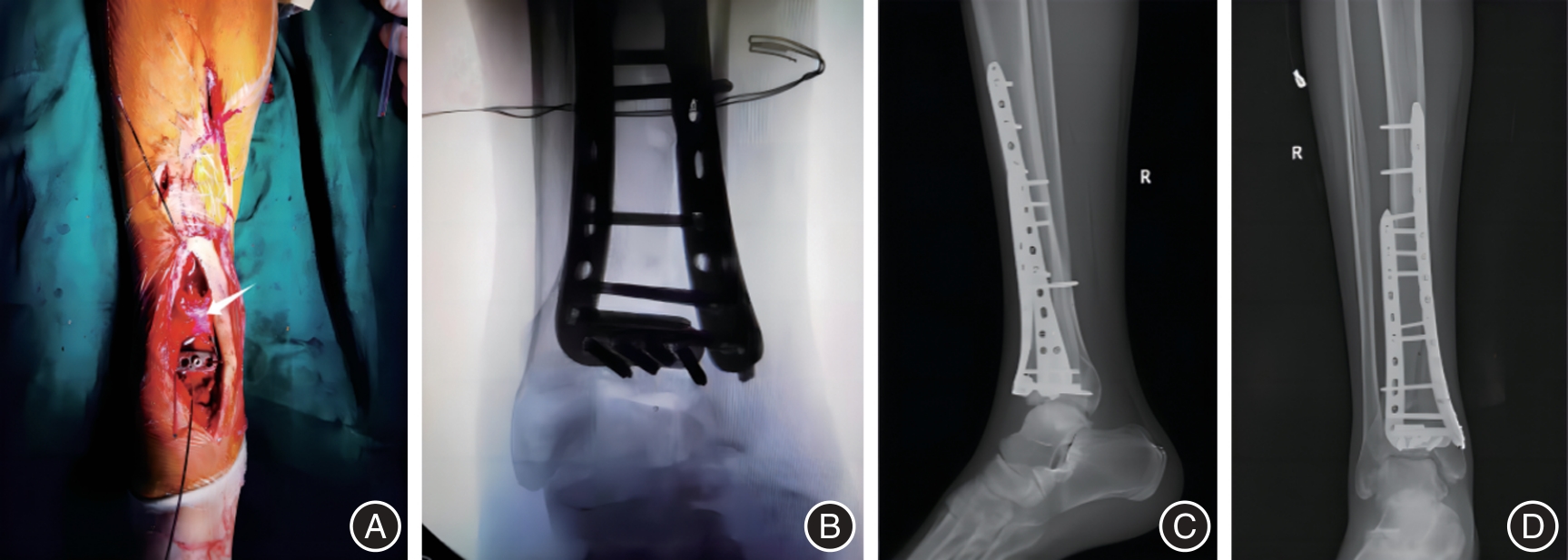

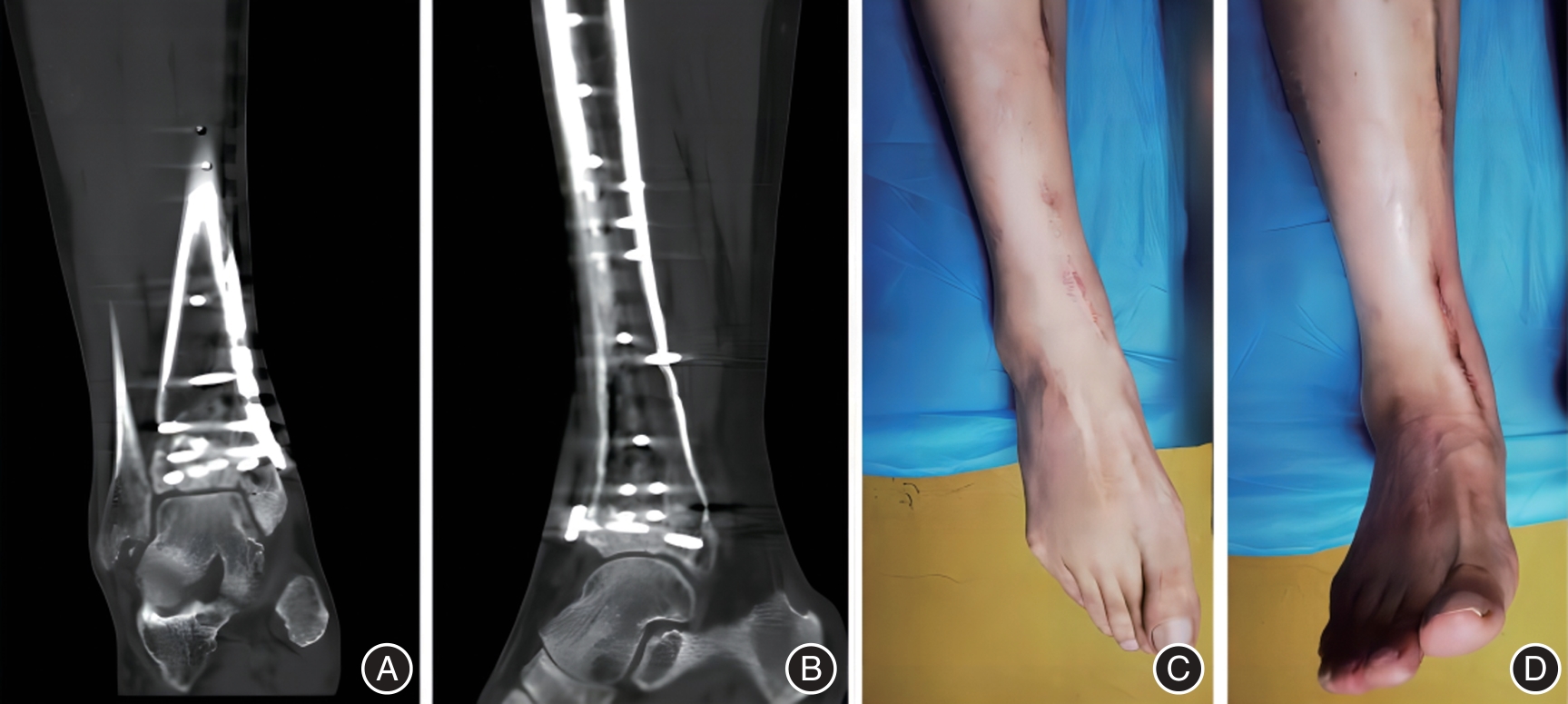
Fig.3
CT reexamination and functional recovery of ankle joint 1 year after surgery"
| 1 |
VAN RYSSELBERGHE N L, CAMPBELL S T, GOODNOUGH L H, et al.Metaphyseal callus formation in pilon fractures is associated with loss of alignment: Is stiffer better?[J].Injury,2021,52(4): 977-981. doi:10.1016/j.injury.2020.10.080
doi: 10.1016/j.injury.2020.10.080 |
| 2 |
HU H, ZhANG J, XIE X G,et al.Identification of risk factors for surgical site infection after type II and type III tibial pilon fracture surgery[J]. World J Clin Cases, 2022,10(19): 6399-6405. doi:10.12998/wjcc.v10.i19.6399
doi: 10.12998/wjcc.v10.i19.6399 |
| 3 |
PINA-RIVA A, MUT-PONS R, LlOPIS E. Presurgical Perspective and Postsurgical Evaluation of Tibial Pilon Fractures[J]. Semin Musculoskelet Radiol, 2022,26(6): 623-634. doi:10.1055/s-0042-1760122
doi: 10.1055/s-0042-1760122 |
| 4 | 张宪高, 张一, 王志强. 胫骨远端pilon骨折手术入路研究进展[J]. 中华骨与关节外科杂志, 2021,14(4): 303-309. |
| 5 |
WILLIAMS C E, JOO P, OH I, et al. Arthroscopically Assisted Internal Fixation of Foot and Ankle Fractures: A Systematic Review[J]. Foot Ankle Orthop, 2021,6(1): 683315514. doi:10.1177/2473011420950214
doi: 10.1177/2473011420950214 |
| 6 |
SUNG Y T, WU J S.The Visual Analogue Scale for Rating, Ranking and Paired-Comparison (VAS-RRP): A new technique for psychological measurement[J]. Behav Res Methods, 2018,50(4): 1694-1715. doi:10.3758/s13428-018-1041-8
doi: 10.3758/s13428-018-1041-8 |
| 7 |
HUANG M, WANG Q, GUAN J, et al.Tips and Tricks in surgical reduction of the posterior column of AO/OTA C3 pilon fractures[J]. BMC Musculoskelet Disord, 2022,23(1): 2. doi:10.1186/s12891-021-04890-6
doi: 10.1186/s12891-021-04890-6 |
| 8 |
VELASCO B T, CHIEN B, KWON J Y,et al.Online Ratings and Reviews of American Orthopaedic Foot and Ankle Surgeons[J]. Foot Ankle Spec, 2020,13(1): 43-49. doi:10.1177/1938640019832363
doi: 10.1177/1938640019832363 |
| 9 |
GULBRANDSEN T R, HULICK R M, P0LK A J,et al. Does surgical approach affect sagittal plane alignment and pilon fracture outcomes?[J]. Injury, 2020,51(3): 750-758. doi:10.1016/j.injury.2020.01.020
doi: 10.1016/j.injury.2020.01.020 |
| 10 | 唐润,杨杰,李毅,等. 改良内侧入路治疗内侧柱压缩性Pilon骨折[J]. 中国骨伤, 2022,35(3): 248-252. |
| 11 |
ASSAL M,RAY A, STERN R. The extensile approach for the operative treatment of high-energy pilon fractures: Surgical technique and soft-tissue healing[J]. J Orthop Trauma, 2007,21(3): 198-206. doi:10.1097/bot.0b013e3180316780
doi: 10.1097/bot.0b013e3180316780 |
| 12 | 刘斌, 邱贵兴, 裴福兴, 等. 骨科加速康复围手术期疼痛管理专家共识[J]. 中华骨与关节外科杂志, 2022,15(10): 739-745. |
| 13 |
YAO Y, LI G, LI J,et al. Short-Term Outcomes of Enhanced Recovery after Surgery (ERAS) for Ankle Fracture Patients: A Single-Center Retrospective Cohort Study[J]. Orthop Surg, 2023,15(3):766-776. doi:10.1111/os.13621
doi: 10.1111/os.13621 |
| 14 |
KORRAPATI A, TA C N, MITCHELL B C, et al. Fracture blisters: Predictors for time to definitive fixation in pilon fractures[J]. Eur J Orthop Surg Traumatol, 2024,34(1):161-166. doi:10.1007/s00590-023-03623-w
doi: 10.1007/s00590-023-03623-w |
| 15 | 余进伟,陈豪杰,张雁儒,等. 新型Pilon钢板治疗C型Pilon骨折的疗效研究[J]. 中国修复重建外科杂志, 2023,37(1):31-36. |
| 16 |
MURAWSKI C D, MITTWEDE P N, WAWROSE R A,et al. Management of High-Energy Tibial Pilon Fractures[J]. J Bone Joint Surg Am, 2023,105(14):1123-1137. doi:10.2106/jbjs.21.01377
doi: 10.2106/jbjs.21.01377 |
| 17 |
MA Z, ZHAN J, ZHU N, et al. A comparative study of the clinical efficacy of supination-adduction type II ankle fracture surgery based on the medial pilon fracture concept versus the ankle fracture concept[J]. BMC Musculoskelet Disord, 2021,22(1): 936. doi:10.1186/s12891-021-04818-0
doi: 10.1186/s12891-021-04818-0 |
| 18 | 李庆虎, 傅佰圣, 赵闯, 等. Pilon骨折术后感染的危险因素分析[J]. 实用骨科杂志, 2021,27(7): 598-600. |
| 19 |
KORRAPATI A, TA C N, MITCHELL B C, et al. Fracture blisters: predictors for time to definitive fixation in pilon fractures[J]. Eur J Orthop Surg Traumatol, 2024,34(1):161-166. doi:10.1007/s00590-023-03623-w
doi: 10.1007/s00590-023-03623-w |
| 20 | 姜刚强, 焦福德, 应霁翀, 等. 分期手术治疗复杂闭合Pilon骨折[J]. 中国骨伤, 2022,35(9):878-882. |
| 21 | 胡远军, 成瑞萍, 史会明, 等. 改良前内侧入路治疗Ruedi-Allgower Ⅲ型Pilon骨折的疗效[J]. 实用骨科杂志, 2020,26(2): 124-127. |
| 22 | 周骅, 薛剑锋, 周朝, 等. 改良前内侧手术入路对Ruedi-Allgower Ⅲ型Pilon骨折的临床效果分析[J]. 浙江创伤外科, 2022,27(1): 139-140. |
| 23 | 黄绍飞,杨云平,黄海. 改良前内侧入路治疗复杂闭合性Pilon骨折的疗效[J]. 中华实验外科杂志, 2020,37(11):2121. |
| 24 | 付鲲鹏, 张晓敏, 赵艳霞, 等. 改良前内侧入路与前外侧入路对C3型Pilon骨折复位及疗效的影响[J]. 西南国防医药, 2020,30(8): 739-742. |
| 25 | 王伟, 刘增瑞, 李艳卫, 等. 两种手术入路治疗Pilon骨折43例疗效观察[J]. 实用骨科杂志, 2014,20(12): 1141-1142. |
| 26 | 陈伟练, 黎俊豪, 郑伟坤. 改良双切口锁定加压钢板固定治疗高能量闭合性Pilon骨折疗效分析[J]. 创伤外科杂志, 2018,20(11): 855-858. |
| 27 |
LEE W, TRAN S, COODPER M T, et al. Clinical Outcomes of Osteochondral Lesions of the Tibial Plafond Following Arthroscopic Microfracture[J]. Foot Ankle Int, 2019,40(9): 1018-1024. doi:10.1177/1071100719850145
doi: 10.1177/1071100719850145 |
| 28 |
MALIGE A, YEAZELL S, NWACHUKU C.Surgical fixation of pilon injuries: A comparison of the anterolateral and posterolateral approach[J].Arch Orthop Trauma Surg, 2019,139(9): 1179-1185. doi:10.1007/s00402-019-03145-3
doi: 10.1007/s00402-019-03145-3 |
| 29 | 俞光荣, 洪浩. 踝关节损伤的治疗进展与思考[J]. 中国骨伤, 2016,29(12): 1071-1073. |
| [1] | Yingyuan ZHANG,Chunyan MOU,Danqing XU,Yuanzhen WANG,Lixian CHANG,Chunyun LIU,Weikun LI,Hongyan WEI,Li LIU. Comparison of clinical efficacy of TMF and TDF in the treatment of hepatitis B liver fibrosis [J]. The Journal of Practical Medicine, 2024, 40(22): 3215-3220. |
| [2] | Yanping WANG,Wenhui GAO,Yanting WU,Jun YANG,Yi ZHOU,Xiaoshun. JIAN. Analysis of influencing factors on clinical efficacy of neutropenia with febrile neutropenia in tumor patients [J]. The Journal of Practical Medicine, 2024, 40(18): 2597-2601. |
| [3] | ZHANG Tong, LI Xiaoyong, CHEN Yanjun, CHEN Shengyang, HU Shuiquan, CHENG Bingbing, TONG Hao, SONG Lishan.. Clinical efficacy of IRE ablation combined with PD ⁃1 inhibitor and chemotherapy in treatment of locally advanced pancreatic cancer [J]. The Journal of Practical Medicine, 2023, 39(9): 1153-1158. |
| [4] |
HUANG Hancong, CHEN Qianhua, YANG Xiaorui..
Effects of cisplatin and pemetrexed combined with recombinant human endostatin injection in elderly patients with lung adenocarcinoma [J]. The Journal of Practical Medicine, 2023, 39(8): 1009-1014. |
| [5] | Shijun YOU,Xue LIANG,Chunlian WANG,Yuhan. SONG. The effect of modified ginseng and schisandra decoction on the efficacy and inflammatory indicators of children with lobar pneumonia (lung spleen deficiency syndrome) caused by mycoplasma pneumonia infection [J]. The Journal of Practical Medicine, 2023, 39(24): 3281-3285. |
| [6] | Chengnian ZHANG,Xuecheng LI,Zheng ZHANG,Daijie. ZHANG. Clinical efficacy of olecranon osteotomy approach vs lateral elbow approach for the treatment of transarticular coronal shear fracture of the distal humerus with open reduction and internal fixation surgery [J]. The Journal of Practical Medicine, 2023, 39(19): 2506-2510. |
| [7] | Jianghao PAN,Jianming SUN,Jiaming SONG,Guangyin FU,Yong LEI,Xiaojie. ZHANG. Evaluation value of monitoring changes of ultrasonic elastic imaging parameters before and after CDT combined with ART in patients with acute deep venous thrombosis of lower extremities [J]. The Journal of Practical Medicine, 2023, 39(18): 2362-2367. |
| [8] |
ZHANG Juan, YU Yakun, TIAN Jingjing, HUANG Yichen, DUO Ruixue, SHEN Haili..
The clinical efficacy and safety of tofacitinib for difficult ⁃ to ⁃ treat rheumatoid arthritis:A retrospective case study [J]. The Journal of Practical Medicine, 2022, 38(8): 1006-1011. |
| [9] |
NAN Ran, LI Yixuan..
Effect of Qinggan Huashi Huoxue decoction combined with silybin capsule on liver fibrosis in patients with alcoholic liver disease [J]. The Journal of Practical Medicine, 2022, 38(8): 1022-1026. |
| [10] |
ZHANG Qi, ZHANG Qingqing, WANG Zesheng, GAO Jinwei, CHENG Xiaozhou, ZHANG Yupeng, WANG Xiaohu, CAO Weijia, QU Kunpeng. .
Research status of endoscopic thyroidectomy and parathyroid auto ⁃ transplantation [J]. The Journal of Practical Medicine, 2022, 38(8): 1032-1036. |
| [11] |
WANG Xiaoxia, LUO Jianjun, DENG Yong, FANG Xiangming..
Efficacy of antioxidant combined with conventional therapy in patients with severe craniocerebral injury complicated with pulmonary infection [J]. The Journal of Practical Medicine, 2022, 38(16): 2066-2070. |
| [12] | LIU Yang, HE Chunshui, ZHANG Lifeng, ZENG Wei, LIN Yao, GENG Caijuan, WANG Ke, WANG Qiqi, HUANG Wei, WEI Haijun.. Clinical efficacy of AngioJet⁃assisted mechanical thrombectomy for the treatment of acute lower limb isch⁃ emia and its prognosis [J]. The Journal of Practical Medicine, 2022, 38(10): 1255-1259. |
| [13] | LI Yiyu, GUAN Yaxin, WU Bin. Research progress in bisphosphonates for treatment of primary osteoporosis [J]. The Journal of Practical Medicine, 2021, 37(5): 569-573. |
| [14] |
LI Zhichao, GUO Xia, WANG Shi, YIN Wei..
Effects of Huaiqihuang Granule on immune function in children with recurrent systemic lupus erythemato⁃sus [J]. The Journal of Practical Medicine, 2021, 37(4): 525-529. |
| [15] |
ZHOU Heping, ZHA Zhengjiang, WANG Lei, CHEN Min, ZHANG Qingchao, TANG Jian..
Clinical effect of neuroendoscopic surgery on patients with severe intraventricular hemorrhage [J]. The Journal of Practical Medicine, 2021, 37(23): 3003-3007. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||