实用医学杂志 ›› 2025, Vol. 41 ›› Issue (22): 3467-3473.doi: 10.3969/j.issn.1006-5725.2025.22.001
• 专题报道:生殖健康 •
魏志霞,冯莉,杨海澜( )
)
Zhixia WEI,Li FENG,Hailan. YANG()
摘要:
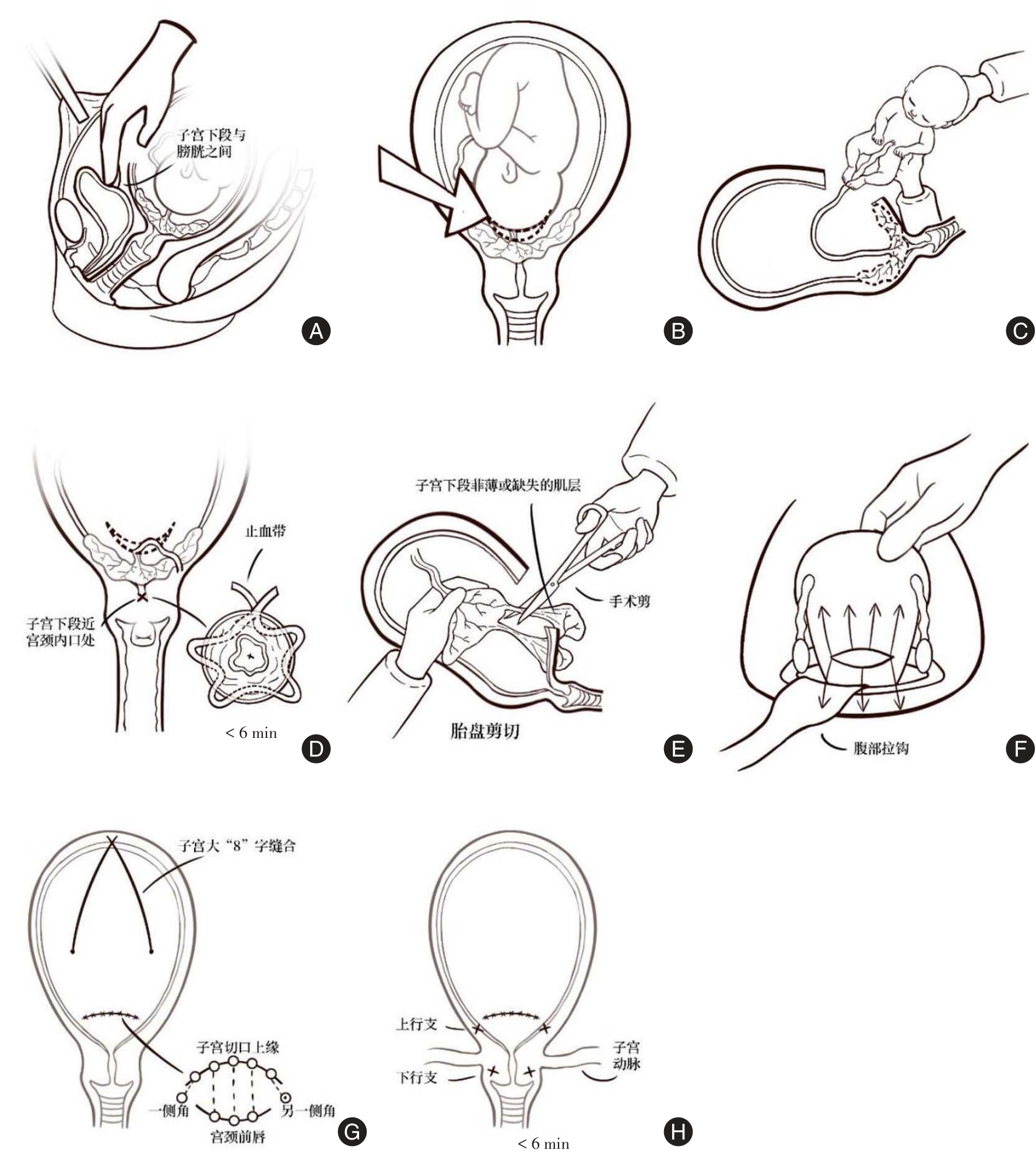
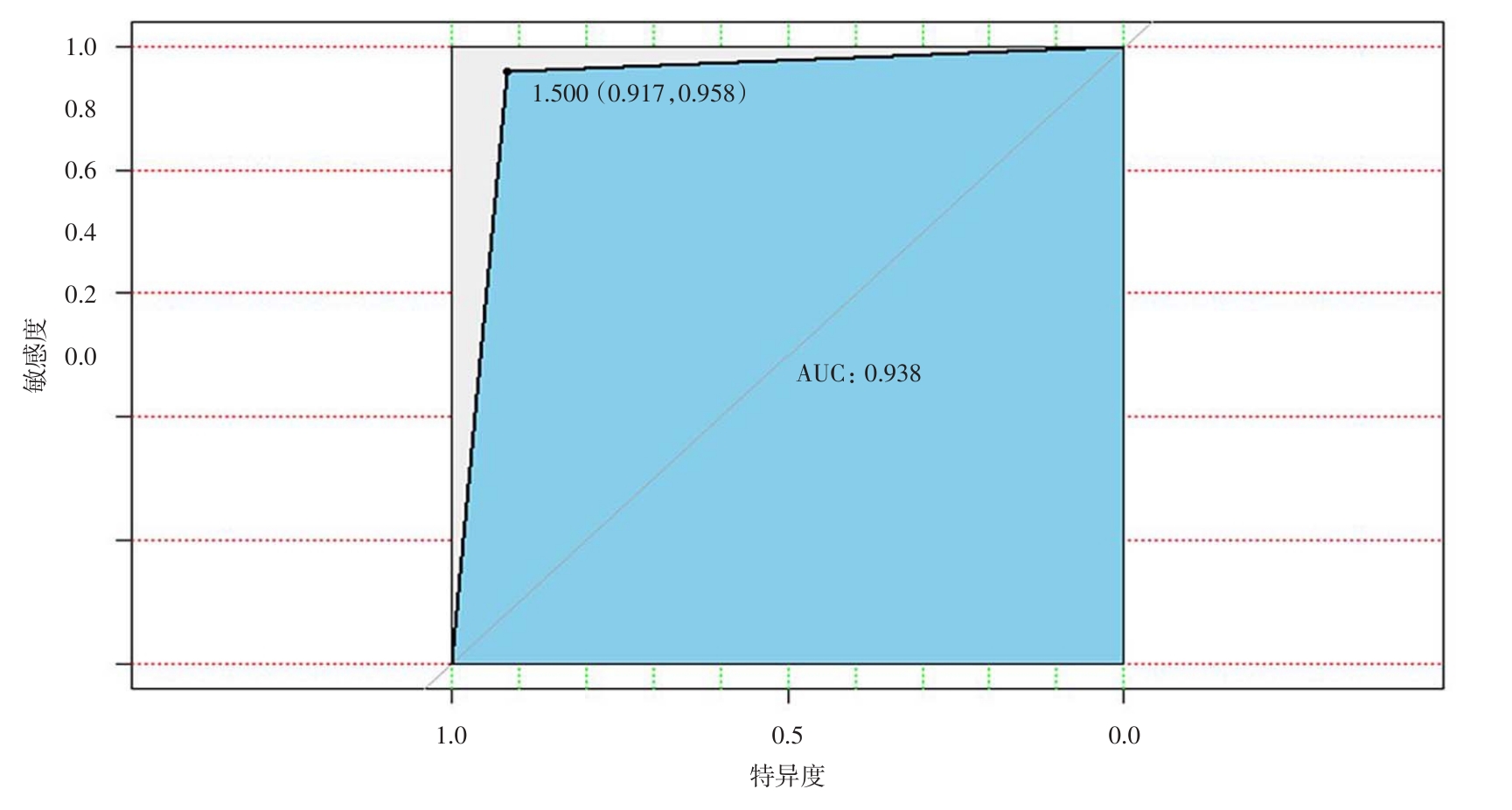
目的 探析改良式剖宫产术对胎盘植入性疾病(PAS)妊娠结局的应用效果。 方法 采用回顾性研究设计,选取于2016年1月至2025年1月间在山西医科大学第一医院行剖宫产手术的176例PAS孕妇作为研究对象,2021年1月17日前接受传统剖宫产手术的患者为对照组(n = 115),2021年1月17日后接受改良剖宫产手术的患者为改良组(n = 61)。收集并比较两组患者孕周、年龄、孕次、术中出血量等临床资料;后使用随机森林算法构建PAS不良妊娠结局的风险预测模型。 结果 改良组中仅1例患者需要进行子宫切除(1.64%),显著低于对照组的19例(16.52%)。此外,改良组患者术中诊断胎盘植入率高于对照组,改良组患者失血性休克、弥散性血管内凝血、新生儿窒息的发生率低于对照组,而发生子宫捆绑和子宫动脉结扎术的比例高于对照组,差异有统计学意义(P < 0.05)。将患者按照出血量分为低出血量和高出血量两个亚组进行后续分析,结果显示,两组患者孕次比较,差异有统计学意义(P < 0.05);而两组中进行改良术式的患者比例差异无统计学意义(P > 0.05)。构建模型预测难治性产后出血(AUC = 0.938,95%CI:0.917 ~ 0.958),采用Gini系数进行模型特征分析,孕次、流产次数及超声诊断胎盘植入等自变量在预测难治性产后出血方面发挥着关键作用(P < 0.05)。 结论 改良剖宫产术式在处理PAS时,能够有效减少术中及术后的出血量,显著降低子宫切除的风险,从而改善妊娠结局。
中图分类号: