实用医学杂志 ›› 2024, Vol. 40 ›› Issue (12): 1659-1664.doi: 10.3969/j.issn.1006-5725.2024.12.008
廖恺,田允鸿,郑荣辉,何彩娴,彭继勇,李慧君( )
)
Kai LIAO,Yunhong TIAN,Ronghui ZHENG,Caixian HE,Jiyong PENG,Huijun LI()
摘要:
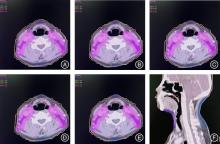
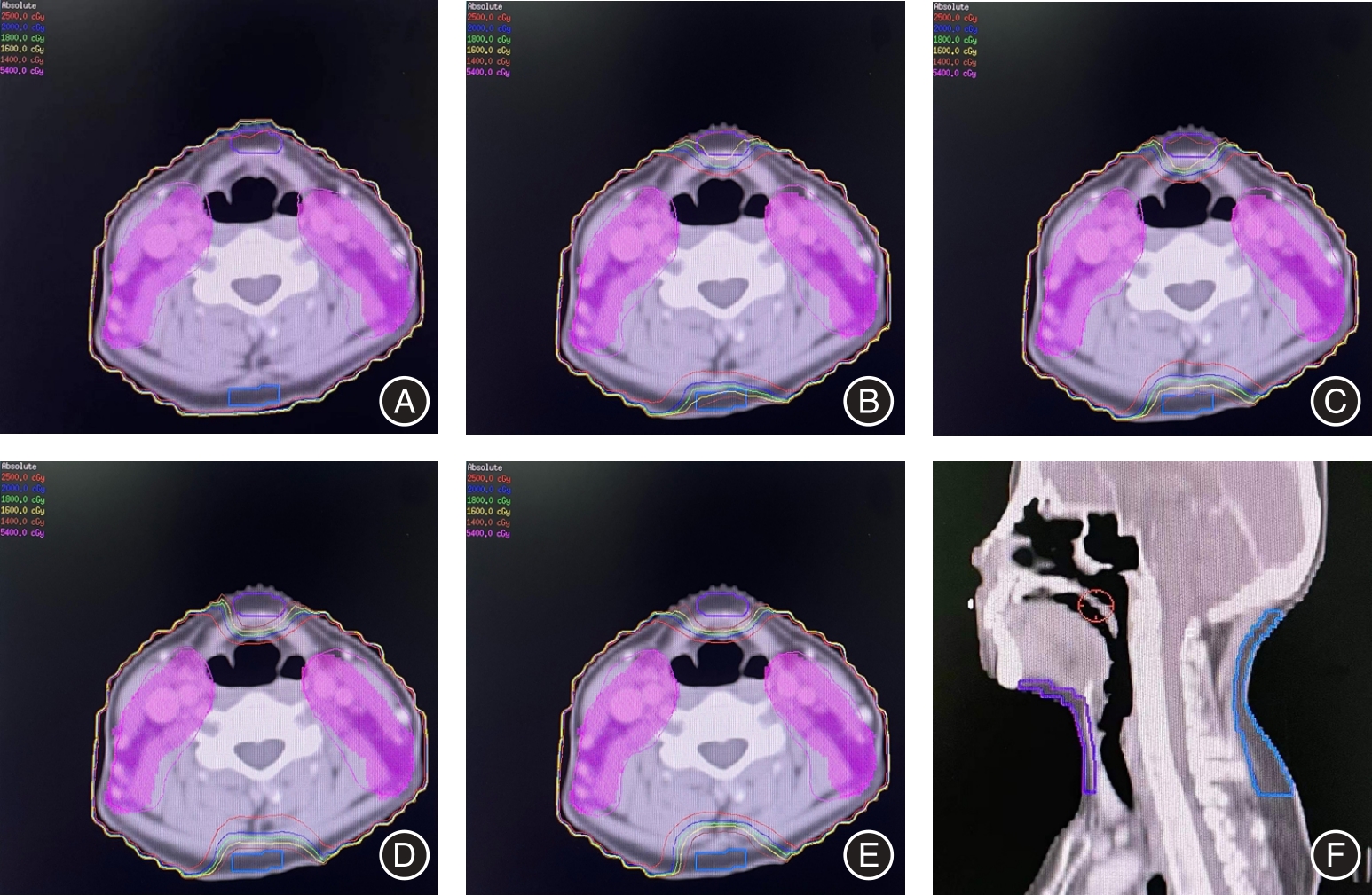
目的 从剂量学角度探讨早期鼻咽癌调强放疗模式下为减少头颈淋巴水肿设置颈前后部限量环的最佳限制剂量。 方法 纳入2022年1-9月在广州医科大学附属肿瘤医院行放疗CT定位的初治早期鼻咽癌患者15例,每个病例设计5套放疗计划。计划A为常规无限量环计划,计划B-E为设置限量环计划,分别设置20、18、16、14 Gy等剂量限制梯度,其余参数与计划A保持一致。通过随机区组设计资料的方差分析和两两比较,评估对靶区覆盖及危及器官限量的影响,确定最佳剂量限值。 结果 最终确定16 Gy为取得靶区覆盖及危及器官限量平衡的最佳剂量限值截点。颈前后部设置16 Gy限量环,与常规计划相比,基本不影响靶区剂量覆盖(P > 0.05),仅稍影响均匀性(P < 0.05);不影响内耳、下颌骨、脑干的剂量(均P > 0.05);可以显著降低口腔、喉、甲状腺剂量(均P < 0.05);稍增加腮腺、脊髓剂量(均P < 0.05),但仍在耐受量范围内。 结论 通过剂量学研究,确定了颈前后部限量环的最佳剂量限值,以期为临床提供一种减少早期鼻咽癌放疗后头颈淋巴水肿的调强放疗计划设计方式。
中图分类号: