

The Journal of Practical Medicine ›› 2025, Vol. 41 ›› Issue (6): 812-817.doi: 10.3969/j.issn.1006-5725.2025.06.006
• Clinical Research • Previous Articles
Manjun LI1,Leilei HU2,Haijun HU2,Jing ZHANG2,Shuchun YU2,Zhenzhong LUO2,Wei. DENG2( )
)
Received:2024-12-14
Online:2025-03-25
Published:2025-03-31
Contact:
Wei. DENG
E-mail:dengweidoc@163.com
CLC Number:
Manjun LI,Leilei HU,Haijun HU,Jing ZHANG,Shuchun YU,Zhenzhong LUO,Wei. DENG. Comparison of the application of video stylet and video laryngoscope in nasotracheal intubation in oral surgery[J]. The Journal of Practical Medicine, 2025, 41(6): 812-817.
Tab.1
Comparison of general conditions between two groups of patients"
| 一般情况 | N组 | C组 | t/χ 2 值 | P值 |
|---|---|---|---|---|
| 例数 | 40 | 40 | ||
| 性别/例 | 0.452 | 0.501 | ||
| 男 | 23 | 20 | ||
| 女 | 17 | 20 | ||
| ASA分级/例 | 1.147 | 0.284 | ||
| Ⅰ | 11 | 7 | ||
| Ⅱ | 29 | 33 | ||
| 年龄/岁 | 41.51 ± 5.66 | 44.02 ± 6.77 | 1.799 | 0.076 |
| 体质量指数/(kg/m2) | 26.22 ± 2.61 | 27.19 ± 2.57 | 1.675 | 0.223 |
| 张口度/cm | 4.18 ± 1.16 | 4.41 ± 1.23 | 0.860 | 0.392 |
| 气道分级/例 | 0.912 | 0.340 | ||
| Ⅰ | 15 | 11 | ||
| Ⅱ | 25 | 29 | ||
| 喉结到鼻孔的垂直距离/cm | 8.07 ± 0.41 | 8.16 ± 0.33 | 1.082 | 0.283 |
| 鼻孔入路/例 | 0.581 | 0.446 | ||
| 左侧 | 12 | 9 | ||
| 右侧 | 28 | 31 |

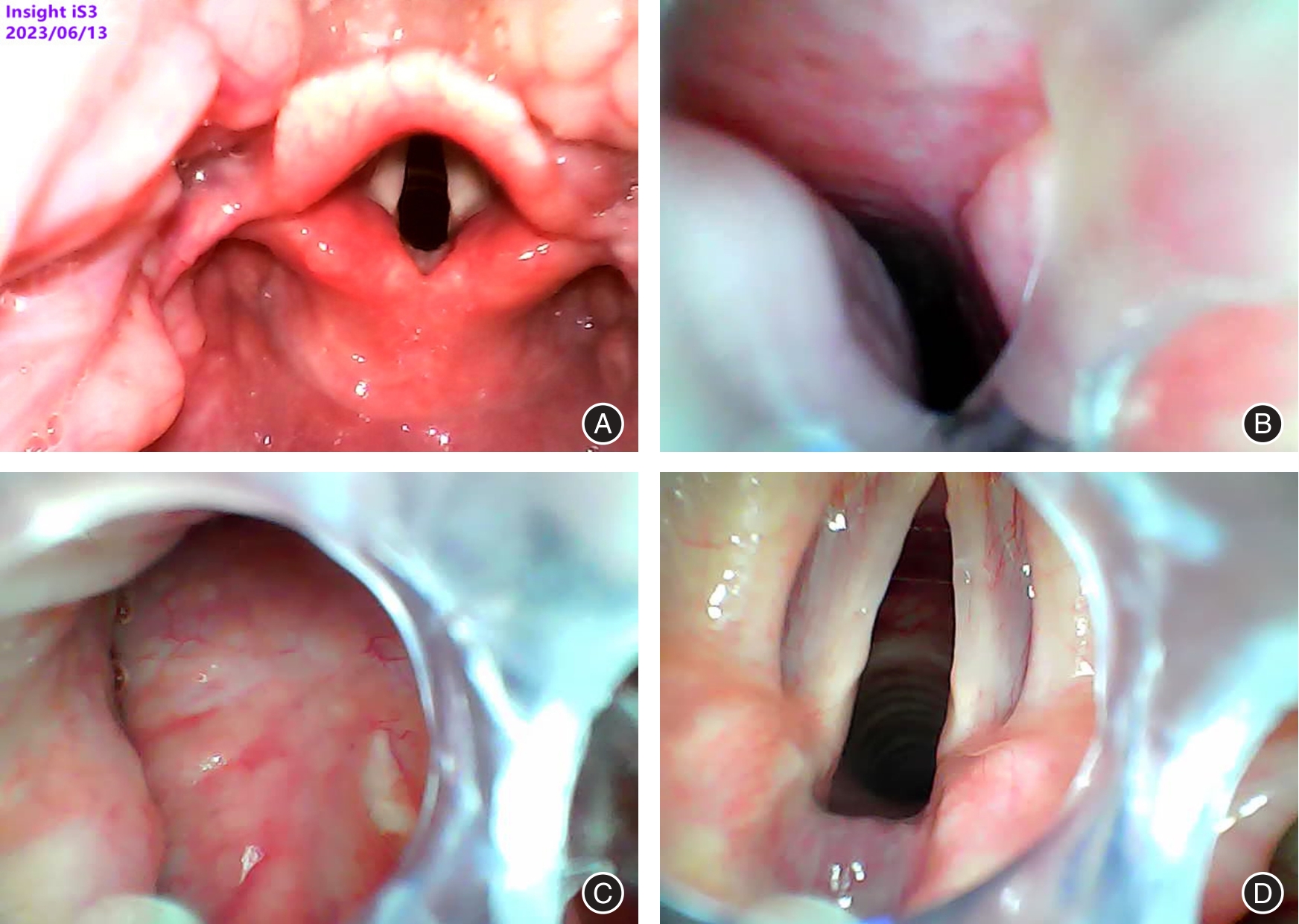
Fig. 1
Surgical procedure"
Tab.2
Comparison of intubation conditions between the two groups of patients"
| 插管情况 | N组(n = 40) | C组(n = 40) | t/χ2值 | P值 |
|---|---|---|---|---|
| 插管时间/s | 35.67 ± 8.71 | 44.96 ± 7.63 | 5.058 | < 0.001 |
| 鼻腔通过时间/s | 7.24 ± 2.33 | 9.57 ± 2.52 | 4.294 | < 0.001 |
| 声门暴露时间/s | 18.36 ± 5.22 | 20.82 ± 6.67 | 1.837 | 0.070 |
| 插管次数/[例(%)] | ||||
| 1次 | 31(77.5) | 27(67.5) | 1.003 | 0.317 |
| 2次 | 9(22.5) | 13(32.5) | 1.003 | 0.317 |
| C-L声门分级/[例(%)] | ||||
| Ⅰ级 | 21(52.5) | 24(60.0) | 0.457 | 0.499 |
| Ⅱ级 | 18(45.0) | 15(37.5) | 0.464 | 0.496 |
| Ⅲ级 | 1(2.5) | 1(2.5) | 0.513 | 0.474 |
| 助手协助情况/[例(%)] | ||||
| 套囊充气 | 0(0) | 10(25.0) | 11.429 | < 0.001 |
| 插管钳辅助 | 0(0) | 6(24.0) | 4.505 | 0.034 |
| 托举下颌 | 7(17.5) | 4(10.0) | 0.949 | 0.330 |
Tab.3
Comparison of vital signs between the two groups of patients before and after intubation"
| 组别 | MAP/mmHg | HR/(次/min) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T3 | T0 | T1 | T2 | T3 | ||
| N组(n = 40) | 73.52 ± 7.72 | 80.17 ± 8.23 | 89.58 ± 8.53 | 86.28 ± 8.27 | 64.88 ± 9.11 | 70.41 ± 9.28 | 74.24 ± 8.45 | 71.60 ± 8.51 | |
| C组(n = 40) | 71.52 ± 8.12 | 85.66 ± 8.45 | 95.58 ± 8.64 | 84.93 ± 8.34 | 60.57 ± 10.34 | 77.18 ± 9.95 | 84.98 ± 9.04 | 75.08 ± 8.26 | |
| t值 | 1.129 | 2.944 | 3.126 | 0.727 | 1.978 | 3.147 | 5.489 | 1.856 | |
| P值 | 0.262 | 0.004 | 0.003 | 0.469 | 0.052 | 0.002 | < 0.001 | 0.067 | |
Tab.4
Comparison of intubation complications between"
| 并发症 | N组(n = 40) | C组(n = 40) | t/χ2值 | P值 |
|---|---|---|---|---|
| 鼻出血 | ||||
| 轻度 | 2(5.0) | 15(37.5) | 12.624 | < 0.001 |
| 中度 | 0(0) | 2(5.0) | 0.513 | 0.474 |
| 重度 | 0(0) | 0(0) | ||
| 门齿松动 | 0(0) | 6(15.0) | 4.505 | 0.034 |
| 口腔黏膜出血 | 0(0) | 6(15.0) | 4.505 | 0.034 |
| 术后咽喉痛 | 1(2.5) | 2(5.0) | 0.002 | 0.963 |
| 1 |
HOSSEINPOUR S, TUNER J, FEKRAZAD R. Photobiomodulation in Oral Surgery: A Review[J]. Photobiomodul Photomed Laser Surg, 2019,37(12):814-825. doi:10.1089/photob.2019.4712
doi: 10.1089/photob.2019.4712 |
| 2 | 辛婧媛, 汤翠翠, 张丽华, 等. 可视喉镜引导下口腔手术患者经鼻气管内插管的临床观察[J]. 实用医学杂志, 2013,29(9):1542-1543. |
| 3 |
PIPER N, LACEY J, KONSTANTATOS A. Unilateral dilated pupil following nasotracheal intubation[J]. Anaesth Rep, 2021,9(2):e12142. doi:10.1002/anr3.12142
doi: 10.1002/anr3.12142 |
| 4 | WILLIAMS K D, TARIQ M, ACHAREKAR M V, et al. Submental Intubation in Maxillofacial Procedures: A More Desired Approach Than Nasotracheal Intubation and Tracheostomy[J]. Cureus, 2022,14(7):e27475. |
| 5 |
TSUKAMOTO M, TAURA S, KADOWAKI S, et al. Risk Factors for Postoperative Sore Throat After Nasotracheal Intubation[J]. Anesth Prog, 2022,69(3):3-8. doi:10.2344/anpr-69-01-05
doi: 10.2344/anpr-69-01-05 |
| 6 |
KIM J, JEON S. Nasotracheal intubation in pediatrics: A narrative review[J]. J Dent Anesth Pain Med, 2024,24(2):81-90. doi:10.17245/jdapm.2024.24.2.81
doi: 10.17245/jdapm.2024.24.2.81 |
| 7 |
HUANG S H, BAI J, JIN J, et al. Nasotracheal intubation in an angiosarcoma-related difficult airway: A case presentation[J]. Quant Imaging Med Surg, 2022,12(12):5492-5495. doi:10.21037/qims-22-469
doi: 10.21037/qims-22-469 |
| 8 |
PARK D H, LEE C A, JEONG C Y, et al. Nasotracheal intubation for airway management during anesthesia[J]. Anesth Pain Med (Seoul), 2021,16(3):232-247. doi:10.17085/apm.21040
doi: 10.17085/apm.21040 |
| 9 |
SAINI V K, ANGURANA S K. Nasotracheal Intubation Among Children Requiring Mechanical Ventilation: Good, Better, or Best?[J]. Pediatr Crit Care Med, 2020,21(11):1024-1025. doi:10.1097/pcc.0000000000002449
doi: 10.1097/pcc.0000000000002449 |
| 10 | 鲁媛媛,张永辉,余理想,等. 静脉麻醉可视喉镜下夹持式环杓关节复位技术临床报告[J]. 中华耳鼻咽喉头颈外科杂志, 2022,57(9):1095-1101. |
| 11 |
PARKEY S, ERICKSON T, HAYDEN E M, et al. Flexible nasotracheal intubation compared to blind nasotracheal intubation in the setting of simulated angioedema[J]. Am J Emerg Med, 2019,37(11):1995-1998. doi:10.1016/j.ajem.2019.02.012
doi: 10.1016/j.ajem.2019.02.012 |
| 12 | 刘具会,靳紫彬,徐文莉,等. 不同折弯角度可视管芯引导经鼻气管插管效果的比较[J]. 临床麻醉学杂志, 2021,37(6):617-620. |
| 13 |
DHAKATE V R, SINGAM A P, BHARADWAJ H S. Evaluation of Nasopharyngeal Airway to Facilitate Nasotracheal Intubation[J]. Ann Maxillofac Surg, 2020,10(1):57-60. doi:10.4103/ams.ams_190_19
doi: 10.4103/ams.ams_190_19 |
| 14 |
WAHDAN A S, EL-REFAI N, OMAR S H, et al. Endotracheal intubation in patients undergoing open abdominal surgery in the lateral position: A comparison between the intubating video stylet and fiberoptic intubating bronchoscopy[J]. Korean J Anesthesiol, 2021,74(3):234-241. doi:10.4097/kja.20384
doi: 10.4097/kja.20384 |
| 15 |
HUNG K C, CHANG Y J, CHEN I W, et al. Comparison of video-stylet and video-laryngoscope for endotracheal intubation in adults with cervical neck immobilisation: A meta-analysis of randomised controlled trials[J]. Anaesth Crit Care Pain Med, 2021,40(6):100965. doi:10.1016/j.accpm.2021.100965
doi: 10.1016/j.accpm.2021.100965 |
| 16 |
CHEN I W, LI Y Y, HUNG K C, et al. Comparison of video-stylet and conventional laryngoscope for endotracheal intubation in adults with cervical spine immobilization: A PRISMA-compliant meta-analysis[J]. Medicine (Baltimore), 2022,101(33):e30032. doi:10.1097/md.0000000000030032
doi: 10.1097/md.0000000000030032 |
| 17 |
ZHANG T, ZHAO K Y, ZHANG P, et al. Comparison of video laryngoscope, video stylet, and flexible videoscope for transoral endotracheal intubation in patients with difficult airways: A randomized, parallel-group study[J]. Trials, 2023,24(1):599. doi:10.1186/s13063-023-07641-1
doi: 10.1186/s13063-023-07641-1 |
| 18 |
KING B J, PADNOS I, MANCUSO K, et al. Comparing Video and Direct Laryngoscopy for Nasotracheal Intubation[J]. Anesth Prog, 2020,67(4):193-199. doi:10.2344/anpr-67-02-08
doi: 10.2344/anpr-67-02-08 |
| 19 |
YIN F, ZHANG T J. Cardiac arrest by rhino-cardiac reflex during nasotracheal intubation[J]. Asian J Surg, 2023,46(6):2358-2359. doi:10.1016/j.asjsur.2022.11.145
doi: 10.1016/j.asjsur.2022.11.145 |
| 20 |
MESSINA S, MEROLA F, SANTONOCITO C, et al. Articulating Video Stylet Compared to Other Techniques for Endotracheal Intubation in Normal Airways: A Simulation Study in Consultants with No Prior Experience[J]. J Clin Med, 2024,13(3):728. doi:10.3390/jcm13030728
doi: 10.3390/jcm13030728 |
| 21 |
TSUKAMOTO M, KAMEYAMA I, MIYAJIMA R, et al. Alternative Technique for Nasotracheal Intubation Using a Flexible Fiberoptic Scope[J]. Anesth Prog, 2022,69(2):35-37. doi:10.2344/anpr-69-02-10
doi: 10.2344/anpr-69-02-10 |
| 22 |
HU H Z, CHENG X X, ZHANG T, et al. A visual laryngoscope combined with a fiberoptic bronchoscope improves intubation outcomes in patients with predicted difficult airways in thoracic surgery[J]. BMC Pulm Med, 2024,24(1):558. doi:10.1186/s12890-024-03369-z
doi: 10.1186/s12890-024-03369-z |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||