

The Journal of Practical Medicine ›› 2025, Vol. 41 ›› Issue (14): 2217-2223.doi: 10.3969/j.issn.1006-5725.2025.14.014
• Clinical Research • Previous Articles
Haowen ZHU1,Shijie XU1,Ran LIU1,Xinhua HONG1,Yiting XUE1,Wenze TIAN2,Zhen. SU1( )
)
Received:2025-02-27
Online:2025-07-25
Published:2025-07-29
Contact:
Zhen. SU
E-mail:494578873@qq.com
CLC Number:
Haowen ZHU,Shijie XU,Ran LIU,Xinhua HONG,Yiting XUE,Wenze TIAN,Zhen. SU. Effects of two driving pressure-based methods to set positive end-expiratory pressure on pulmonary mechanics and oxygenation in patients undergoing laparoscopic and thoracoscopic esophagectomy[J]. The Journal of Practical Medicine, 2025, 41(14): 2217-2223.
Tab.1
Comparison of general conditions of two groups of patients"
| 指标 | D组 | I组 | t/χ2 值 | P值 |
|---|---|---|---|---|
| 年龄/岁 | 67.30 ± 6.43 | 68.53 ± 6.64 | -0.731 | 0.468 |
| ASA 分级/例 | 2.308 | 0.129 | ||
| Ⅱ | 24 | 28 | ||
| Ⅲ | 6 | 2 | ||
| 性别/例 | 0.071 | 0.791 | ||
| 男 | 19 | 18 | ||
| 女 | 11 | 12 | ||
| BMI/(kg/m2) | 23.04 ± 1.74 | 22.40 ± 2.05 | 1.299 | 0.199 |
| 吸烟史/[例(%)] | 7(23.33) | 3(10.00) | 1.920 | 0.166 |
| 高血压病史/[例(%)] | 10(33.33) | 8(26.67) | 0.317 | 0.573 |
| 糖尿病病史/[例(%)] | 2(6.67) | 3(10.00) | 0.218 | 0.640 |
| 心血管疾病史/[例(%)] | 2(6.67) | 5(16.67) | 1.456 | 0.228 |
| 胸腔镜时间/min | 80.80 ± 15.97 | 87.83 ± 18.32 | -1.585 | 0.118 |
| 腹腔镜时间/min | 31.23 ± 5.17 | 33.47 ± 6.39 | -1.488 | 0.142 |
| 手术时间/min | 194.73 ± 34.01 | 207.17 ± 46.92 | -1.175 | 0.245 |
| 液体入量/mL | 1 640.00 ± 245.79 | 1 660.67 ± 302.33 | -0.291 | 0.772 |
| 尿量/mL | 330.00 ± 58.13 | 366.67 ± 142.84 | -1.302 | 0.198 |
| 失血量/mL | 106.33 ± 32.26 | 117.67 ± 63.93 | -0.861 | 0.393 |
| 血管活性药物(间羟胺)用量/mg | 2.70 ± 1.60 | 3.05 ± 1.13 | -0.972 | 0.335 |
Tab.2
Comparison of intraoperative respiratory mechanics of two groups of patients"
| 指标 | 组别 | T1 | T2 | T3 | T4 |
|---|---|---|---|---|---|
| PEEP | D组 | 5.00 ± 0.00 | 7.60 ± 1.07# | 7.27 ± 1.17# | 7.27 ± 1.17# |
| I组 | 5.00 ± 0.00 | 6.93 ± 0.98 | 6.53 ± 1.04 | 6.53 ± 1.04 | |
| Pplat | D组 | 16.67 ± 2.32 | 20.93 ± 1.57 | 20.57 ± 1.76 | 16.00 ± 1.76 |
| I组 | 17.23 ± 1.63 | 21.27 ± 2.29 | 20.80 ± 1.92 | 16.50 ± 1.48 | |
| Ppeak | D组 | 20.10 ± 2.44 | 24.10 ± 2.16 | 23.70 ± 2.17 | 19.03 ± 1.73 |
| I组 | 20.83 ± 1.82 | 24.76 ± 2.27 | 24.53 ± 2.00 | 19.80 ± 1.49 | |
| 驱动压 | D组 | 11.67 ± 2.32 | 13.33 ± 1.52# | 13.30 ± 1.29# | 8.73 ± 1.84# |
| I组 | 11.33 ± 1.65 | 14.33 ± 2.22 | 14.27 ± 1.51 | 9.96 ± 1.45 | |
| Cdyn/(mL/cmH2O) | D组 | 32.32 ± 7.52 | 21.43 ± 3.78# | 29.01 ± 3.54# | 41.28 ± 8.28# |
| I组 | 30.77 ± 4.88 | 19.56 ± 2.94 | 26.88 ± 3.38 | 36.49 ± 4.16 |
Tab.3
Comparison of hemodynamic parameters and blood gas analysis of two groups of patients"
| 指标 | 组别 | T0 | T1 | T2 | T3 | T4 | T5 |
|---|---|---|---|---|---|---|---|
| MAP/mmHg | D组 | 93.23 ± 8.73 | 78.03 ± 5.93 | 78.30 ± 7.41 | 81.37 ± 8.38 | 84.40 ± 7.37 | 86.93 ± 5.03 |
| I组 | 89.87 ± 6.90 | 77.63 ± 5.22 | 75.73 ± 5.14 | 79.00 ± 4.18 | 79.87 ± 3.75 | 84.80 ± 3.62 | |
| HR/(次/min) | D组 | 79.00 ± 7.11 | 72.87 ± 7.48 | 78.97 ± 9.27 | 73.07 ± 8.26 | 76.17 ± 7.07 | 82.07 ± 5.56 |
| I组 | 80.57 ± 10.09 | 70.97 ± 8.80 | 76.40 ± 9.34 | 74.60 ± 9.77 | 77.73 ± 4.56 | 80.17 ± 4.57 | |
| PaO2 /mmHg | D组 | 82.00 ± 10.26 | 332.30 ± 67.51 | 228.13 ± 67.80# | 295.47 ± 68.00# | 343.90 ± 74.84# | 110.43 ± 18.65 |
| I组 | 82.67 ± 9.76 | 335.50 ± 57.75 | 189.17 ± 58.41 | 252.83 ± 86.08 | 300.13 ± 91.73 | 112.37 ± 20.40 | |
| PaCO2/mmHg | D组 | 40.07 ± 3.68 | 39.57 ± 4.10 | 52.03 ± 8.15# | 46.80 ± 6.30 | 40.40 ± 3.71# | 41.23 ± 4.68 |
| I组 | 38.67 ± 2.67 | 37.73 ± 3.18 | 56.60 ± 7.53 | 45.80 ± 4.94 | 42.63 ± 3.11 | 41.93 ± 3.73 | |
| pH | D组 | 7.43 ± 0.04 | 7.42 ± 0.03 | 7.35 ± 0.04# | 7.36 ± 0.04 | 7.40 ± 0.03 | 7.41 ± 0.04 |
| I组 | 7.44 ± 0.03 | 7.40 ± 0.05 | 7.30 ± 0.05 | 7.35 ± 0.04 | 7.39 ± 0.04 | 7.39 ± 0.03 | |
| Hb | D组 | 12.69 ± 1.22 | 12.29 ± 1.16 | 12.09 ± 1.14 | 11.55 ± 1.18 | 11.70 ± 1.23 | 12.24 ± 1.42 |
| I组 | 12.42 ± 1.44 | 11.95 ± 1.55 | 11.47 ± 1.56 | 10.97 ± 1.41 | 11.42 ± 1.73 | 12.19 ± 1.66 | |
| SPO2 /% | D组 | 96.70 ± 1.51 | 99.90 ± 0.53 | 98.33 ± 1.18 | 99.53 ± 0.78 | 99.60 ± 0.56 | 98.03 ± 1.22 |
| I组 | 96.37 ± 0.96 | 99.80 ± 0.31 | 98.37 ± 1.54 | 99.73 ± 0.52 | 99.80 ± 0.41 | 98.63 ± 1.16 | |
| OI /mmHg | D组 | 390.47 ± 48.87 | 415.40 ± 84.38 | 285.20 ± 84.76# | 492.44 ± 113.32# | 573.17 ± 124.74# | 380.81 ± 64.31 |
| I组 | 393.66 ± 46.48 | 419.40 ± 72.20 | 236.48 ± 73.01 | 421.38 ± 143.47 | 500.22 ± 152.89 | 387.47 ± 70.34 |
Tab.4
Comparison of respiratory mechanics before and after titration of PEEP"
| 指标 | 胸腔镜期间 | 腹腔镜期间 | ||
|---|---|---|---|---|
| D组 | I组 | D组 | I组 | |
| Pplat | ||||
| 滴定前 | 15.73 ± 1.48 | 16.70 ± 2.32 | 15.77 ± 1.41 | 16.53 ± 1.61 |
| 滴定后 | 20.93 ± 1.57# | 21.27 ± 2.29# | 23.70 ± 2.17# | 20.80 ± 1.92# |
| Ppeak | ||||
| 滴定前 | 18.87 ± 1.72 | 19.93 ± 2.59 | 19.00 ± 1.68 | 20.20 ± 1.67 |
| 滴定后 | 24.10 ± 2.16# | 24.77 ± 2.27# | 23.70 ± 2.17# | 24.53 ± 2.00# |
| 驱动压 | ||||
| 滴定前 | 15.73 ± 1.48 | 16.70 ± 2.32 | 15.77 ± 1.41 | 16.53 ± 1.61 |
| 滴定后 | 13.33 ± 1.52# | 14.33 ± 2.22# | 13.30 ± 1.29# | 14.27 ± 1.51# |
| Cdyn/(mL/cmH2O) | ||||
| 滴定前 | 18.58 ± 2.43 | 17.50 ± 2.65 | 25.12 ± 3.50 | 23.89 ± 2.64 |
| 滴定后 | 21.43 ± 3.78# | 19.56 ± 2.94# | 29.01 ± 3.54# | 26.88 ± 3.38# |
Tab.5
Comparison of postoperative conditions between the two groups of patients"
| 指标 | D组 | I组 | t/χ2 /Z值 | P值 |
|---|---|---|---|---|
| 3 d内PPCs发生率 | 10(33.33) | 12(40.00) | 0.287 | 0.592 |
| 7 d内PPCs发生率 | 12(40.00) | 13(43.33) | 0.069 | 0.793 |
| 住院时间(x ± s)/d | 20.53 ± 2.94 | 21.03 ± 3.67 | -0.582 | 0.563 |
| 住院费用[M(P25,P75 )]/元 | 93 838.44(88 973.71,100 142.18) | 100 489.50(90 932.61,108 962.68) | -1.981 | 0.048 |
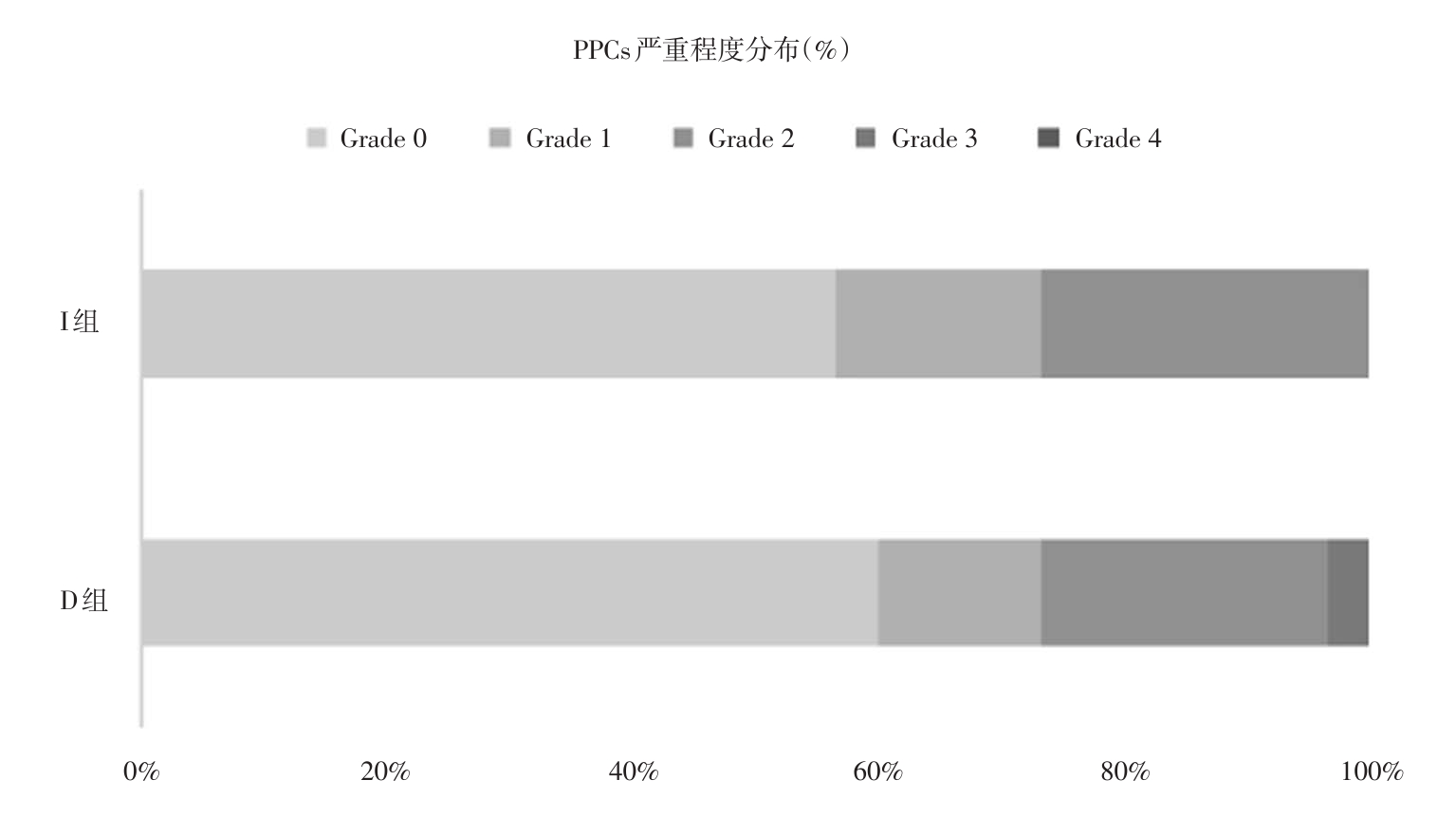
Fig.1
Grades of the severity of PPCs within 7 days after operation"
| [1] |
郑荣寿,陈茹,韩冰峰,等. 2022年中国恶性肿瘤流行情况分析[J]. 中华肿瘤杂志,2024,46(3):221-231. doi:10.3760/cma.j.cn112152-20240119-00035
doi: 10.3760/cma.j.cn112152-20240119-00035 |
| [2] |
SHELLEY B, GLASS A, KEAST T, et al. Perioperative cardiovascular pathophysiology in patients undergoing lung resection surgery: A narrative review[J]. Br J Anaesth. 2023;130(1):e66-e79. doi:10.1016/j.bja.2022.06.035
doi: 10.1016/j.bja.2022.06.035 |
| [3] | FERRANDO C, CARRAMINANA A, PINEIRO P, et al. Individualised, perioperative open-lung ventilation strategy during one-lung ventilation (iPROVE-OLV): A multicentre, randomised, controlled clinical trial[J]. Lancet Respir Med,2024,12(3):195-206. |
| [4] | 任亚雯,刘孟洁,王月兰. 驱动压导向个体化呼气末正压对术后肺部并发症的影响[J]. 国际麻醉学与复苏杂志,2023,44(10):1090-1093. |
| [5] |
HE P, WU C, YANG Y, et al. Effectiveness of postural lung recruitment on postoperative atelectasis assessed by lung ultrasound in children undergoing lateral thoracotomy cardiac surgery with cardiopulmonary bypass[J]. Pediatr Pulmonol,2021,56(6):1724-1732. doi:10.1002/ppul.25315
doi: 10.1002/ppul.25315 |
| [6] |
SODERSTROM H, MOONS J, NAFTEUX P, et al. Major Intraoperative Complications During Minimally Invasive Esophagectomy[J]. Ann Surg Oncol,2023,30(13):8244-8250. doi:10.1245/s10434-023-14340-3
doi: 10.1245/s10434-023-14340-3 |
| [7] |
GU W J, CEN Y, ZHAO F Z, et al. Association between driving pressure-guided ventilation and postoperative pulmonary complications in surgical patients: A meta-analysis with trial sequential analysis[J].Br J Anaesth,2024,133(3):647-657. doi:10.1016/j.bja.2024.04.060
doi: 10.1016/j.bja.2024.04.060 |
| [8] | 郭玉,王昌理,丁任,等. 中国中老年人肺功能、慢性肺疾病与头痛的相关性:基于CHARLS分析[J]. 海军军医大学学报,2024,45(11):1395-1401. |
| [9] |
辛超,高巨,葛亚丽,等. 驱动压导向个体化呼气末正压对机器人辅助前列腺癌根治术老年患者术中脑血流及局部脑氧饱和度的影响[J]. 实用医学杂志,2023,39(12):1524-1528,1535. doi:10.3969/j.issn.1006-5725.2023.12.011
doi: 10.3969/j.issn.1006-5725.2023.12.011 |
| [10] |
SPADARO S, GRASSO S, KARBING D S, et al. Physiological effects of two driving pressure-based methods to set positive end-expiratory pressure during one lung ventilation[J].J Clin Monit Comput,2021,35(5):1149-1157. doi:10.1007/s10877-020-00582-z
doi: 10.1007/s10877-020-00582-z |
| [11] |
SIMONTE R, CAMMAROTA G, DE ROBERTIS E. Intraoperative lung protection: Strategies and their impact on outcomes[J].Curr Opin Anaesthesiol,2024,37(2):184-191. doi:10.1097/aco.0000000000001341
doi: 10.1097/aco.0000000000001341 |
| [12] |
LI X F, JIANG R J, MAO W J, et al. The effect of driving pressure-guided versus conventional mechanical ventilation strategy on pulmonary complications following on-pump cardiac surgery: A randomized clinical trial[J].J Clin Anesth,2023,89:111150. doi:10.1016/j.jclinane.2023.111150
doi: 10.1016/j.jclinane.2023.111150 |
| [13] | 秦晨光,方开云,彭晶,等. 驱动压导向呼气末正压通气对原位肝移植患者术中氧合和术后并发症的影响[J]. 临床麻醉学杂志,2024,40(7):677-682. |
| [14] |
ZHANG C, XU F, LI W, et al. Driving Pressure-Guided Individualized Positive End-Expiratory Pressure in Abdominal Surgery: A Randomized Controlled Trial[J].Anesth Analg,2021,133(5):1197-1205. doi:10.1213/ane.0000000000005575
doi: 10.1213/ane.0000000000005575 |
| [15] |
XAVIER T B, COELHO L V, FERREIRA D A L, et al. Individualized positive end-expiratory pressure reduces driving pressure in obese patients during laparoscopic surgery under pneumoperitoneum: A randomized clinical trial[J]. Front Physiol,2024,15:1383167. doi:10.3389/fphys.2024.1383167
doi: 10.3389/fphys.2024.1383167 |
| [16] | 张倩倩,孙高悦,钟晓倩,等. 驱动压导向呼气末正压通气对老年患者腹腔镜前列腺癌根治术后肺功能的影响[J]. 临床麻醉学杂志,2023,39(4):351-356. |
| [17] |
黄伟坚,李洋,王海彦,等. 基于驱动压的肺保护性通气策略在婴儿单肺通气中的应用效果[J]. 实用医学杂志,2024,40(3):360-364. doi:10.3969/j.issn.1006-5725.2024.03.014
doi: 10.3969/j.issn.1006-5725.2024.03.014 |
| [18] |
PARK M, YOON S, NAM J S, et al. Driving pressure-guided ventilation and postoperative pulmonary complications in thoracic surgery: A multicentre randomised clinical trial[J].Br J Anaesth,2023,130(1):e106-e118. doi:10.1016/j.bja.2022.06.037
doi: 10.1016/j.bja.2022.06.037 |
| [19] |
KIM Y J, KIM B R, KIM H W, et al. Effect of driving pressure-guided positive end-expiratory pressure on postoperative pulmonary complications in patients undergoing laparoscopic or robotic surgery: A randomised controlled trial[J]. Br J Anaesth,2023,131(5):955-965. doi:10.1016/j.bja.2023.08.007
doi: 10.1016/j.bja.2023.08.007 |
| [20] |
YU J, WU Z, AN R, et al. Association between driving pressure and postoperative pulmonary complications in patients undergoing lung resection surgery: A randomised clinical trial[J]. Anaesth Crit Care Pain Med,2023,42(1):101160. doi:10.1016/j.accpm.2022.101160
doi: 10.1016/j.accpm.2022.101160 |
| [21] |
GAO L, ZHANG B, QI J, et al. Effects of individualized positive end-expiratory pressure on intraoperative oxygenation and postoperative pulmonary complications in patients requiring pneumoperitoneum with Trendelenburg position: A systematic review and meta-analysis[J]. Int J Surg,2025,111(1):1386-1396. doi:10.1097/js9.0000000000002041
doi: 10.1097/js9.0000000000002041 |
| [22] |
DE SANTIS SANTIAGO R, TEGGIA DROGHI M, FUMAGALLI J, et al. High Pleural Pressure Prevents Alveolar Overdistension and Hemodynamic Collapse in Acute Respiratory Distress Syndrome with Class Ⅲ ObesityA Clinical Trial[J].Am J Respir Crit Care Med,2021,203(5):575-584. doi:10.1164/rccm.201909-1687oc
doi: 10.1164/rccm.201909-1687oc |
| [23] |
LI X, LIU H, WANG J, et al. Individualized Positive End-expiratory Pressure on Postoperative Atelectasis in Patients with Obesity: A Randomized Controlled Clinical Trial[J]. Anesthesiology,2023,139(3):262-273. doi:10.1097/aln.0000000000004603
doi: 10.1097/aln.0000000000004603 |
| [24] |
SCHARFFENBERG M, MANDELLI M, BLUTH T, et al. Respiratory mechanics and mechanical power during low vs. high positive end-expiratory pressure in obese surgical patients-A sub-study of the PROBESE randomized controlled trial[J]. J Clin Anesth,2024,92:111242. doi:10.1016/j.jclinane.2023.111242
doi: 10.1016/j.jclinane.2023.111242 |
| [25] |
SZAMOS K, BALLA B, PALOCZI B, et al. One-lung ventilation with fixed and variable tidal volumes on oxygenation and pulmonary outcomes: A randomized trial[J]. J Clin Anesth,2024,95:111465. doi:10.1016/j.jclinane.2024.111465
doi: 10.1016/j.jclinane.2024.111465 |
| [26] | 朱佳羽,姚婧,王子轩,等. 驱动压指导PEEP滴定对机器人辅助前列腺癌根治术老年患者肺损伤的影响[J]. 中华麻醉学杂志,2022,42(1):39-43. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||