实用医学杂志 ›› 2024, Vol. 40 ›› Issue (22): 3155-3159.doi: 10.3969/j.issn.1006-5725.2024.22.006
王慧群,叶超,许朝,陈思,张开光,肖梅( )
)
Huiqun WANG,Chao YE,Chao XU,Si CHEN,Kaiguang ZHANG,Mei. XIAO()
摘要:
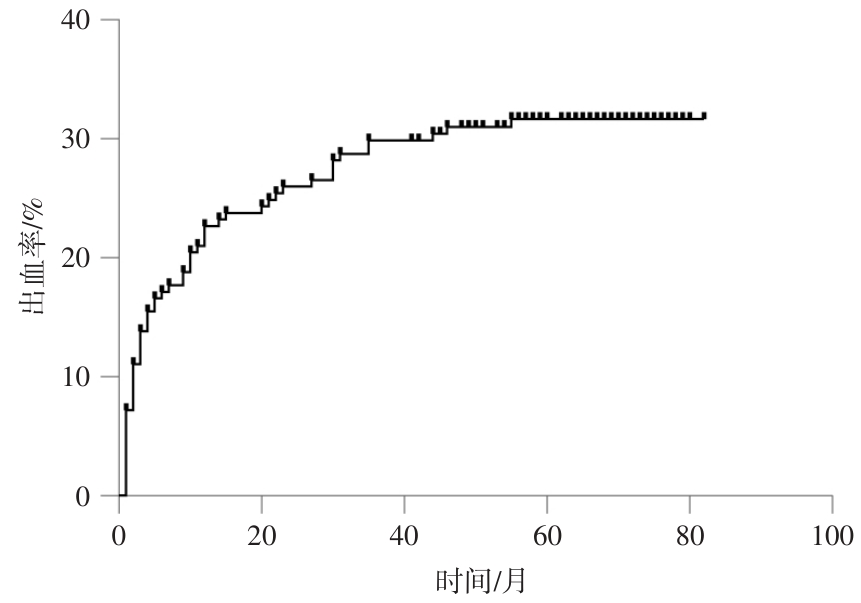
目的 探讨影响肝硬化食管胃底静脉曲张破裂出血(EGVB)内镜治疗后5年再发消化道出血的因素。 方法 回顾性选取2017年2月至2019年5月于中国科学技术大学附属第一医院就诊的肝硬化EGVB行内镜治疗的181例患者,至少随访5年。分析患者性别、年龄、肝硬化病因(病毒、酒精、自免、其他)、是否合并腹水、肝性脑病(无、1 ~ 2期、3期)、门静脉血栓、肝癌、门脉高压性胃病等并发症、外周血指标[谷草转氨酶(AST)、谷丙转氨酶(ALT)、白细胞(WBC)、总胆红素(TBIL)、白蛋白(ALB)、血小板(platelet, PLT)、凝血酶原时间(PT)、国际标准化比值(PTINR)]、门静脉内径、门静脉流速、脾静脉内径、Child分级、是否序贯治疗、再出血时间等临床资料。依据5年随访期间是否发生再出血,将所有患者分为未再出血组(n = 124)与再出血组(n = 57)。分别采用单因素和多因素分析影响内镜治疗后5年再出血的危险因素,采用Kaplan-Meier分析1、3、5年的累积出血率。 结果 单因素和二元logistics回归分析得TBIL、门静脉内径均为EGVB患者内镜治疗后5年再出血的危险因素(P < 0.05)。KM曲线显示,181例患者中,1、3、5年累积出血人数为41、54、57例,累积出血率为22.65%、29.83%、31.49%。 结论 肝硬化EGVB内镜治疗后远期再出血率较高,TBIL和门静脉内径是肝硬化EGVB内镜治疗后远期再出血的独立危险因素,对于TBIL和(或)门静脉内径较高的肝硬化EGVB内镜治疗患者的随访需给予高度重视。
中图分类号: