

实用医学杂志 ›› 2026, Vol. 42 ›› Issue (6): 969-980.doi: 10.3969/j.issn.1006-5725.2026.06.009
梁苏东1( ),黄子强1,林建中2
),黄子强1,林建中2
收稿日期:2025-12-25
修回日期:2026-01-30
接受日期:2026-02-03
出版日期:2026-03-25
发布日期:2026-03-26
通讯作者:
梁苏东
E-mail:hupo5357979@163.com
基金资助:
Sudong LIANG1(),Ziqiang HUANG1,Jianzhong LIN2
Received:2025-12-25
Revised:2026-01-30
Accepted:2026-02-03
Online:2026-03-25
Published:2026-03-26
Contact:
Sudong LIANG
E-mail:hupo5357979@163.com
摘要:
目的 探究瑞维鲁胺联合雄激素剥夺治疗(ADT)对转移性激素敏感性前列腺癌(mHSPC)的近远期疗效及对血游离前列腺特异性抗原百分率(FPSAR)、胃泌素释放肽前体(proGRP)表达的影响。 方法 自医院电子病历库与随访数据库收集2022年8月至2024年2月医院收治的mHSPC患者102例的临床资料,按治疗方式分为瑞维鲁胺组(n = 44,瑞维鲁胺联合ADT治疗)与比卡鲁胺组(n = 58,比卡鲁胺联合ADT治疗),倾向性评分匹配(PSM)法平衡两组基线资料,按1∶1最近邻匹配法,卡钳值设定为0.2,最终获得41对无基线差异数据,比较两组近远期疗效,治疗前后血清前列腺特异性抗原(PSA)、乳酸脱氢酶(LDH)、FPSAR、proGRP、中性粒细胞/淋巴细胞比值(NLR)、血小板计数/淋巴细胞比率(PLR),不良事件、生存预后;所有患者按预后结局分组,Cox回归分析法分析mHSPC患者预后影响因素。 结果 治疗24周后,瑞维鲁胺组近期疾病控制率高于比卡鲁胺组,差异有统计学意义(P < 0.05)。治疗后,瑞维鲁胺组血清PSA、LDH、NLR、PLR、proGRP均显著低于同组治疗前及比卡鲁胺组治疗后,FPSAR高于同组治疗前与比卡鲁胺组治疗后,差异均有统计学意义(P < 0.05)。两组不良反应均可控,比较差异无统计学意义(P > 0.05);瑞维鲁胺组中位无进展生存期(PFS)、中位总生存期(OS)均长于比卡鲁胺组(P < 0.01)。Cox多因素回归分析显示,高瘤负荷、多部位转移、基线高proGRP为mHSPC患者生存预后的危险因素(P < 0.05),瑞维鲁胺 + ADT治疗、基线高FPSAR水平为保护因素(P < 0.05)。 结论 瑞维鲁胺联合ADT治疗mHSPC疾病控制率较高,生存预后更优,能显著上调FPSAR,降低血proGRP水平,且不良反应可控;多部位转移、高瘤负荷、基线高proGRP的mHSPC患者有更差的生存预后,瑞维鲁胺、高FPSAR为保护因素,需重点关注合并上述因素mHSPC患者预后的监测。
中图分类号:
梁苏东,黄子强,林建中. 瑞维鲁胺联合雄激素剥夺治疗转移性激素敏感性前列腺癌患者近远期疗效及对FPSAR、ProGRP表达的影响[J]. 实用医学杂志, 2026, 42(6): 969-980.
Sudong LIANG,Ziqiang HUANG,Jianzhong LIN. The short-term and long-term efficacy of rezvilutamide combined with androgen deprivation therapy in the treatment of patients with metastatic hormone-sensitive prostate cancer and its influence on the expression of FPSAR and ProGRP[J]. The Journal of Practical Medicine, 2026, 42(6): 969-980.
表1
PSM前两组基线资料 (例(%))"
| 资料 | 瑞维鲁胺组(n = 44) | 比卡鲁胺组(n = 58) | χ2 /t值 | P值 |
|---|---|---|---|---|
| 年龄(x ± s)/岁 | 67.52 ± 7.13 | 70.36 ± 6.76 | 2.052 | 0.043 |
| 体质量(x ± s)/kg | 67.86 ± 8.57 | 66.51 ± 10.93 | 0.676 | 0.500 |
| 基础疾病 | ||||
| 合并糖尿病 | 11(25.00) | 18(31.03) | 0.448 | 0.503 |
| 合并高血压 | 16(36.36) | 25(43.10) | 0.473 | 0.492 |
| 临床分期 | 0.015 | 0.902 | ||
| Ⅳa期 | 8(18.18) | 10(17.24) | ||
| Ⅳb期 | 36(81.82) | 48(82.76) | ||
| 转移部位 | 0.126 | 0.989 | ||
| 骨转移 | 22(50.00) | 27(46.55) | ||
| 骨转移 + 淋巴结转移 | 14(31.82) | 20(34.48) | ||
| 内脏转移(肺、肝) | 5(11.36) | 7(12.07) | ||
| 多部位转移(骨 + 内脏 + 淋巴结) | 3(6.82) | 4(6.90) | ||
| ECOG评分 | 0.001 | 0.971 | ||
| 0 ~ 1分 | 41(93.18) | 53(91.38) | ||
| 2分 | 3(6.82) | 5(8.62) | ||
| Gleason评分 | 0.266 | 0.606 | ||
| ≥ 8分 | 29(65.91) | 41(70.69) | ||
| < 8分 | 15(34.09) | 17(29.31) | ||
| 肿瘤负荷 | 1.061 | 0.303 | ||
| 高瘤负荷 | 31(70.45) | 46(79.31) | ||
| 低瘤负荷 | 13(29.55) | 12(20.69) | ||
| 基线血清PSA(x ± s)/(ng/mL) | 79.52 ± 15.17 | 80.24 ± 17.23 | 0.220 | 0.826 |
| 基线LDH(x ± s)/(U/L) | 238.79 ± 47.83 | 240.52 ± 51.09 | 0.174 | 0.862 |
| 基线NLR(x ± s) | 2.41 ± 0.63 | 2.71 ± 0.45 | 2.805 | 0.006 |
| 基线PLR(x ± s) | 125.36 ± 25.47 | 135.14 ± 30.17 | 1.732 | 0.086 |
表2
PSM后两组基线资料 (例(%))"
| 资料 | 瑞维鲁胺组(n = 41) | 比卡鲁胺组(n = 41) | χ2 /t值 | P值 |
|---|---|---|---|---|
| 年龄(x ± s)/岁 | 68.32 ± 7.15 | 68.79 ± 6.95 | 0.302 | 0.764 |
| 体质量(x ± s)/kg | 67.52 ± 8.34 | 67.23 ± 8.57 | 0.155 | 0.877 |
| 基础疾病 | ||||
| 合并糖尿病 | 10(24.39) | 11(26.83) | 0.064 | 0.800 |
| 合并高血压 | 15(36.59) | 17(41.46) | 0.205 | 0.651 |
| 临床分期 | 0.082 | 0.775 | ||
| Ⅳa期 | 7(17.07) | 8(19.51) | ||
| Ⅳb期 | 34(82.93) | 33(80.49) | ||
| 转移部位 | 0.373 | 0.946 | ||
| 骨转移 | 21(51.22) | 20(48.78) | ||
| 骨转移 + 淋巴结转移 | 13(31.71) | 14(34.15) | ||
| 内脏转移(肺、肝) | 4(9.76) | 5(12.20) | ||
| 多部位转移(骨 + 内脏 + 淋巴结) | 3(7.32) | 2(4.88) | ||
| ECOG评分 | - | 1.000 | ||
| 0 ~ 1分 | 38(92.68) | 39(95.12) | ||
| 2分 | 3(7.32) | 2(4.88) | ||
| Gleason评分 | 0.053 | 0.817 | ||
| ≥ 8分 | 27(65.85) | 26(63.41) | ||
| < 8分 | 14(34.15) | 15(36.59) | ||
| 肿瘤负荷 | 0.064 | 0.800 | ||
| 高瘤负荷 | 30(73.17) | 31(75.61) | ||
| 低瘤负荷 | 11(26.83) | 10(24.39) | ||
| 基线血清PSA(x ± s)/(ng/mL) | 78.52 ± 14.17 | 79.65 ± 15.21 | 0.348 | 0.729 |
| 基线LDH(x ± s)/(U/L) | 235.71 ± 42.78 | 237.14 ± 48.25 | 0.142 | 0.887 |
| 基线NLR(x ± s) | 2.38 ± 0.61 | 2.51 ± 0.52 | 1.038 | 0.302 |
| 基线PLR(x ± s) | 124.29 ± 23.41 | 126.34 ± 27.63 | 0.362 | 0.718 |
表3
两组近期疗效对比 (例(%))"
| 项目 | 瑞维鲁胺组 | 比卡鲁胺组 | Z/χ2 值 | P值 |
|---|---|---|---|---|
| 疗效等级 | 1.972 | 0.049 | ||
| 完全缓解 | 3(7.32) | 1(2.44) | ||
| 部分缓解 | 25(60.98) | 20(48.78) | ||
| 稳定 | 9(21.95) | 9(21.95) | ||
| 进展 | 4(9.76) | 11(26.83) | ||
| DCR | 37(90.24) | 30(73.17) | 3.998 | 0.046 |
| PSA50 | 37(90.24) | 29(70.73) | 4.970 | 0.026 |
| PSA90 | 30(73.17) | 21(51.22) | 4.201 | 0.040 |
表4
两组实验室指标比较 (x ± s)"
| 组别 | 例数 | FPSAR/% | LDH/(U/L) | proGRP/(pg/mL) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 基线 | 治疗24周 | 差值 | 基线 | 治疗24周 | 差值 | 基线 | 治疗24周 | 差值 | ||
| 瑞维鲁胺组 | 41 | 13.79 ± 4.01 | 20.51 ± 3.36* | 6.72 ± 3.69 | 235.71 ± 42.78 | 206.36 ± 30.51* | 29.35 ± 36.65 | 45.14 ± 8.36 | 30.05 ± 7.14* | 15.09 ± 7.75 |
| 比卡鲁胺组 | 41 | 13.57 ± 3.86 | 16.32 ± 4.23* | 2.75 ± 4.05 | 237.14 ± 48.25 | 231.25 ± 50.36 | 5.89 ± 49.31 | 46.01 ± 9.74 | 37.14 ± 8.51* | 8.87 ± 9.13 |
| t值 | 0.253 | 4.966 | 4.640 | 0.142 | 2.707 | 2.445 | 0.434 | 4.087 | 3.326 | |
| P值 | 0.801 | < 0.001 | < 0.001 | 0.887 | 0.008 | 0.017 | 0.656 | < 0.001 | 0.001 | |
| 组别 | 例数 | NLR | PLR | PSA/(ng/mL) | ||||||
| 基线 | 治疗24周 | 差值 | 基线 | 治疗24周 | 差值 | 基线 | 治疗24周 | 差值 | ||
| 瑞维鲁胺组 | 41 | 2.38 ± 0.61 | 1.71 ± 0.36* | 0.67 ± 0.49 | 124.29 ± 23.41 | 93.05 ± 10.76* | 31.24 ± 17.09 | 78.52 ± 14.17 | 1.75 ± 0.52* | 76.77 ± 7.35 |
| 比卡鲁胺组 | 41 | 2.51 ± 0.52 | 2.03 ± 0.41* | 0.48 ± 0.47 | 126.34 ± 27.63 | 110.14 ± 7.94* | 16.20 ± 17.79 | 79.65 ± 15.21 | 2.96 ± 0.71* | 76.69 ± 7.96 |
| t值 | 1.038 | 3.755 | 1.792 | 0.362 | 8.183 | 3.904 | 0.348 | 8.804 | 0.047 | |
| P值 | 0.302 | < 0.001 | 0.077 | 0.718 | < 0.001 | < 0.001 | 0.729 | < 0.001 | 0.962 | |
表5
两组治疗不良事件发生率对比 (例(%))"
| 分类 | 不良事件 | 分级 | 瑞维鲁胺组(n = 41) | 比卡鲁胺组(n = 41) | χ2值 | P值 |
|---|---|---|---|---|---|---|
| 内分泌系统 | 潮热 | 1级 | 18(43.90) | 16(39.02) | 0.201 | 0.654 |
| 2级 | 5(12.20) | 4(9.76) | - | 1.000 | ||
| 3级 | 0(0.00) | 1(2.44) | - | 1.000 | ||
| 乳房胀痛 | 1级 | 6(14.63) | 8(19.51) | 0.345 | 0.557 | |
| 2级 | 2(4.88) | 3(7.32) | - | 1.000 | ||
| 3级 | 0(0.00) | 0(0.00) | - | - | ||
| 心血管系统 | 高血压 | 1级 | 7(17.07) | 5(12.20) | 0.391 | 0.532 |
| 2级 | 4(9.76) | 3(7.32) | - | 1.000 | ||
| 3级 | 1(2.44) | 1(2.44) | 0.513 | 0.474 | ||
| 心悸 | 1级 | 3(7.32) | 2(4.88) | - | 1.000 | |
| 2级及以上 | 0(0.00) | 0(0.00) | - | - | ||
| 消化系统 | 恶心 | 1级 | 5(12.20) | 6(14.63) | 0.105 | 0.745 |
| 2级 | 1(2.44) | 1(2.44) | 0.513 | 0.474 | ||
| 腹泻 | 1级 | 4(9.76) | 3(7.32) | - | 1.000 | |
| 2级及以上 | 0(0.00) | 0(0.00) | - | - | ||
| 血液系统 | 中性粒细胞减少 | 1级 | 2(4.88) | 1(2.44) | - | 1.000 |
| 2级及以上 | 0(0.00) | 0(0.00) | - | - | ||
| 贫血 | 1级 | 3(7.32) | 2(4.88) | - | 1.000 | |
| 2级及以上 | 0(0.00) | 0(0.00) | - | - | ||
| 神经系统 | 乏力 | 1级 | 10(24.39) | 9(21.95) | 0.069 | 0.794 |
| 2级 | 3(7.32) | 2(4.88) | - | 1.000 | ||
| 头晕 | 1级 | 4(9.76) | 3(7.32) | - | 1.000 | |
| 2级及以上 | 0(0.00) | 0(0.00) | - | - | ||
| 皮肤及附件 | 皮疹 | 1级 | 2(4.88) | 1(2.44) | - | 1.000 |
| 2级及以上 | 0(0.00) | 0(0.00) | ||||
| 其他 | 骨痛加重 | 1级 | 1(2.44) | 2(4.88) | - | 1.000 |
| 2级 | 0(0.00) | 1(2.44) | - | 1.000 | ||
| 合计 | 任何不良事件 | - | 35(85.37) | 33(80.49) | 0.345 | 0.557 |
| 3级 | - | 1(2.44) | 2(4.88) | - | 1.000 |
表6
两组随访PFS和OS比较 (月)"
| 组别 | 例数 | PFS | |||||
|---|---|---|---|---|---|---|---|
| 均值 | 中位数 | ||||||
| 估计值 | SE | 95%CI | 估计值 | SE | 95%CI | ||
| 瑞维鲁胺组 | 41 | 32.55 | 1.587 | 29.443 ~ 35.665 | 37.20 | 1.701 | 33.866 ~ 40.534 |
| 比卡鲁胺组 | 41 | 17.18 | 2.090 | 13.088 ~ 21.279 | 15.30 | 2.162 | 11.063 ~ 19.537 |
| Log-rank χ2 值 | 28.309 | ||||||
| P值 | < 0.001 | ||||||
| 组别 | 例数 | OS | |||||
| 均值 | 中位数 | ||||||
| 估计值 | SE | 95%CI | 估计值 | SE | 95%CI | ||
| 瑞维鲁胺组 | 41 | 34.93 | 1.193 | 32.586 ~ 37.264 | 38.50 | 2.794 | 33.024 ~ 43.976 |
| 比卡鲁胺组 | 41 | 20.61 | 2.050 | 16.593 ~ 24.627 | 18.40 | 2.162 | 14.162 ~ 22.638 |
| Log-rank χ2 值 | 29.209 | ||||||
| P值 | < 0.001 | ||||||
图1
两组PFS比较"
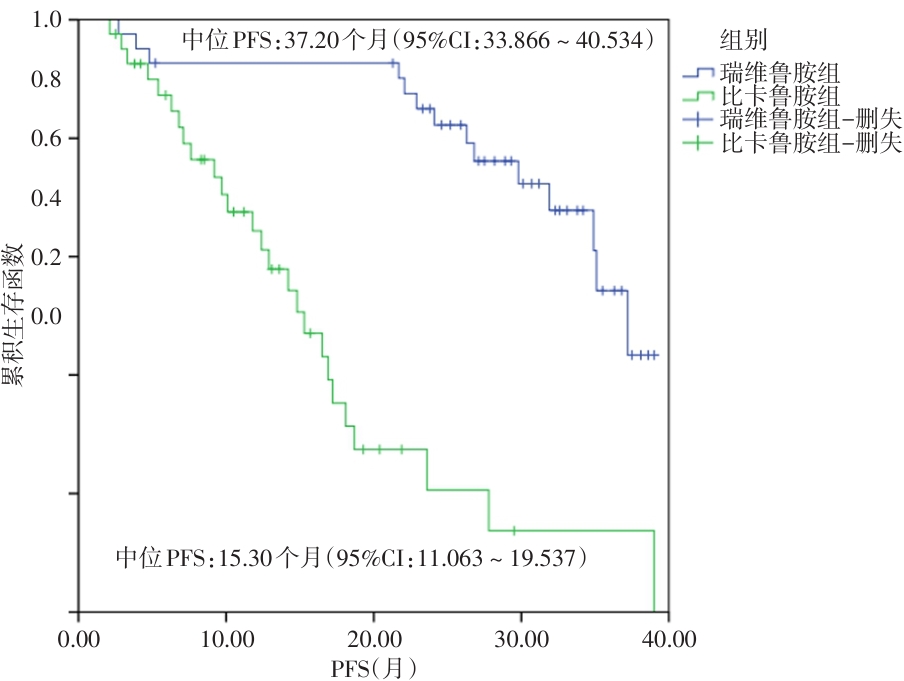
图2
两组OS比较"
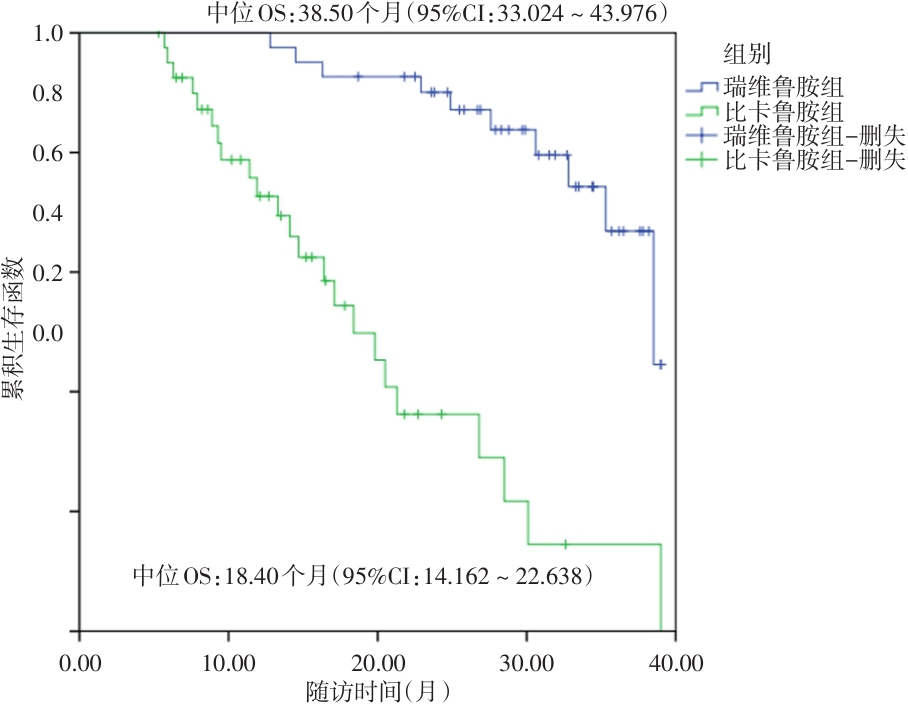
表7
不同预后患者临床特征对比 (例(%))"
| 资料 | 生存组(n = 49) | 死亡组(n = 33) | χ2 /t值 | P值 |
|---|---|---|---|---|
| 年龄(x ± s)/岁 | 66.98 ± 7.63 | 67.08 ± 7.71 | 0.058 | 0.954 |
| 体质量(x ± s)/kg | 67.34 ± 8.41 | 67.17 ± 8.23 | 0.091 | 0.928 |
| 基础疾病 | ||||
| 合并糖尿病 | 12(24.49) | 9(27.27) | 0.080 | 0.777 |
| 合并高血压 | 18(36.73) | 14(42.42) | 0.205 | 0.651 |
| 临床分期 | 3.129 | 0.077 | ||
| Ⅳa期 | 12(24.49) | 3(9.09) | ||
| Ⅳb期 | 37(75.51) | 30(90.91) | ||
| 转移部位 | 30.169 | < 0.001 | ||
| 骨转移 | 36(73.47) | 5(15.15) | ||
| 骨转移 + 淋巴结转移 | 11(22.45) | 16(48.48) | ||
| 内脏转移(肺、肝) | 2(4.08) | 7(21.21) | ||
| 多部位转移(骨 + 内脏 + 淋巴结) | 0(0.00) | 5(15.15) | ||
| ECOG评分 | 1.961 | 0.161 | ||
| 0 ~ 1分 | 48(97.96) | 29(87.88) | ||
| 2分 | 1(2.04) | 4(12.12) | ||
| Gleason评分 | 13.054 | 0.001 | ||
| ≥ 8分 | 24(48.98) | 29(87.88) | ||
| < 8分 | 25(51.02) | 4(12.12) | ||
| 肿瘤负荷 | 19.012 | < 0.001 | ||
| 高瘤负荷 | 28(57.14) | 33(100.00) | ||
| 低瘤负荷 | 21(42.86) | 0(0.00) | ||
| 基线血清PSA(x ± s)/(ng/mL) | 68.72 ± 14.93 | 85.71 ± 17.53 | 4.709 | < 0.001 |
| 基线LDH(x ± s)/(U/L) | 229.85 ± 40.69 | 240.63 ± 50.49 | 1.067 | 0.289 |
| 基线NLR(x ± s) | 2.10 ± 0.57 | 2.97 ± 0.34 | 7.867 | < 0.001 |
| 基线PLR(x ± s) | 111.14 ± 20.71 | 139.51 ± 30.34 | 5.037 | < 0.001 |
| 基线FPSAR(x ± s)/% | 14.95 ± 3.63 | 11.05 ± 3.05 | 5.095 | < 0.001 |
| 基线proGRP(x ± s)/(pg/mL) | 39.71 ± 8.14 | 50.57 ± 9.52 | 5.532 | < 0.001 |
| 治疗方式 | 8.570 | 0.003 | ||
| 瑞维鲁胺 + ADT | 31(63.27) | 10(30.30) | ||
| 比卡鲁胺 + ADT | 18(36.73) | 23(69.70) |
表8
mHSPC患者预后影响因素赋值表"
| 自变量 | 赋值 |
|---|---|
| 治疗方式 | 比卡鲁胺 + ADT = 0,瑞维鲁胺 + ADT = 1 |
| 肿瘤负荷 | 低瘤负荷 = 0,高瘤负荷 = 1 |
| 转移部位 | 非多部位转移 = 0,多部位转移 = 1 |
| Gleason评分 | < 8分 = 0,≥ 8分 = 1 |
| 基线PSA | < 45 ng/mL = 0,≥ 45 ng/mL = 1 |
| 基线FPSAR | < 15% = 0,≥ 15% = 1 |
| 基线NLR | < 3.0 = 0,≥ 3.0 = 1 |
| 基线PLR | < 150 = 0,≥ 150 = 1 |
| 基线proGRP | < 45 pg/mL = 0,≥ 45 pg/mL = 1 |
表9
mHSPC患者预后影响因素Cox回归分析"
| 自变量 | β | SE | Wald χ2 | HR | 95%CI | P值 | VIF |
|---|---|---|---|---|---|---|---|
| 治疗方式 | -0.967 | 0.392 | 6.283 | 0.380 | 0.182 ~ 0.795 | 0.012 | 1.086 |
| 肿瘤负荷 | 1.086 | 0.385 | 8.761 | 2.963 | 1.451 ~ 6.050 | 0.003 | 1.324 |
| 转移部位 | 0.855 | 0.372 | 5.318 | 2.351 | 1.164 ~ 4.746 | 0.018 | 1.395 |
| Gleason评分 | 0.281 | 0.369 | 0.587 | 1.324 | 0.645 ~ 2.719 | 0.385 | 1.243 |
| 基线PSA | 0.579 | 0.395 | 3.728 | 1.784 | 0.893 ~ 3.564 | 0.105 | 1.482 |
| 基线FPSAR | -0.754 | 0.362 | 4.378 | 0.470 | 0.232 ~ 0.952 | 0.036 | 1.189 |
| 基线NLR | 0.484 | 0.397 | 2.876 | 1.623 | 0.793 ~ 3.321 | 0.187 | 1.369 |
| 基线PLR | 0.465 | 0.399 | 2.528 | 1.591 | 0.773 ~ 3.278 | 0.213 | 1.304 |
| 基线proGRP | 0.983 | 0.391 | 7.342 | 2.672 | 1.314 ~ 5.438 | 0.007 | 1.215 |
| [1] |
FILHO A M, LAVERSANNE M, FERLAY J, et al. The GLOBOCAN 2022 cancer estimates: Data sources, methods, and a snapshot of the cancer burden worldwide[J]. Int J Cancer, 2025,156(7):1336-1346. doi: 10.1002/ijc.35278 .
doi: 10.1002/ijc.35278 |
| [2] |
BRAY F, LAVERSANNE M, SUNG H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2024,74(3):229-263. doi: 10.3322/caac.21834 .
doi: 10.3322/caac.21834 |
| [3] |
李唯尊, 邢晨, 安恒庆. STAT活化抑制蛋白2基因在前列腺癌中的表达水平及与临床病理特征的关系[J]. 实用医学杂志, 2025, 41(18): 2844-2852. doi:10.3969/j.issn.1006-5725. 2025.18.009 .
doi: 10.3969/j.issn.1006-5725. 2025.18.009 |
| [4] |
RAVAL A D, CHEN S, LITTLETON N, et al. Real-world use of androgen-deprivation therapy intensification for metastatic hormone-sensitive prostate cancer: A systematic review[J]. BJU Int, 2025,135(3):408-421. doi: 10.1111/bju.16577 .
doi: 10.1111/bju.16577 |
| [5] |
FIZAZI K, CLARKE N W, DE SANTIS M, et al. Capivasertib plus abiraterone in PTEN-deficient metastatic hormone-sensitive prostate cancer: CAPItello-281 phase III study[J]. Ann Oncol, 2026,37(1):53-68. doi: 10.1016/j.annonc.2025.10.004 .
doi: 10.1016/j.annonc.2025.10.004 |
| [6] |
GU W, HAN W, LUO H, et al. Rezvilutamide versus bicalutamide in combination with androgen-deprivation therapy in patients with high-volume, metastatic, hormone-sensitive prostate cancer (CHART): A randomised, open-label, phase 3 trial[J]. Lancet Oncol, 2022, 23(10): 1249-1260. doi: 10.1016/S1470-2045(22)00507-1 .
doi: 10.1016/S1470-2045(22)00507-1 |
| [7] |
KEAM S J. Rezvilutamide: First Approval[J]. Drugs, 2023,83(2):189-193. doi: 10.1007/s40265-022-01831-y .
doi: 10.1007/s40265-022-01831-y |
| [8] |
SINGH K, MANDAL S, NAYAK P, et al. Rezvilutamide for metastatic hormone-sensitive prostate cancer[J]. Lancet Oncol, 2022,23(11):e490. doi: 10.1016/S1470-2045(22)00624-6 .
doi: 10.1016/S1470-2045(22)00624-6 |
| [9] |
GARRIDO M M, MARTA J C, BERNARDINO R M, et al. The percentage of [-2]pro-prostate-specific antigen and the prostate health index outperform prostate-specific antigen and the percentage of free prostate-specific antigen in the detection of clinically significant prostate cancer and can be used as reflex tests[J]. Arch Pathol Lab Med, 2022, 146(6): 691-700. doi: 10.5858/arpa.2021-0079-OA .
doi: 10.5858/arpa.2021-0079-OA |
| [10] |
YASHI M, NISHIHARA D, YOKOYAMA M, et al. Plasma progastrin-releasing peptide level shows different predictive profiles for treatment response by androgen receptor axis-targeted agents in patients with metastatic castration-resistant prostate cancer[J]. Cancer Rep (Hoboken), 2023, 6(3): e1762. doi: 10.1002/cnr2.1762 .
doi: 10.1002/cnr2.1762 |
| [11] |
GILLESSEN S, BOSSI A, DAVIS I D, et al. Management of patients with advanced prostate cancer-metastatic and/or castration-resistant prostate cancer: Report of the Advanced Prostate Cancer Consensus Conference (APCCC) 2022[J]. Eur J Cancer, 2023, 185: 178-215. doi: 10.1016/j.ejca.2023.02.018 .
doi: 10.1016/j.ejca.2023.02.018 |
| [12] |
YOUNES A, HILDEN P, COIFFIER B, et al. International Working Group consensus response evaluation criteria in lymphoma (RECIL 2017)[J]. Ann Oncol, 2017, 28(7): 1436-1447. doi: 10.1093/annonc/mdx097 .
doi: 10.1093/annonc/mdx097 |
| [13] |
BARBOSA F G, QUEIROZ M A, FERRARO D A, et al. Prostate-specific Membrane Antigen PET: Therapy response assessment in metastatic prostate cancer[J]. Radiographics,2020, 40(5): 1412-1430. doi: 10.1148/rg.2020200058 .
doi: 10.1148/rg.2020200058 |
| [14] |
FREITES-MARTINEZ A, SANTANA N, ARIAS-SANTIAGO S, et al. Using the Common Terminology Criteria for Adverse Events (CTCAE-Version 5.0) to evaluate the severity of adverse events of anticancer therapies[J]. Actas Dermosifiliogr (Engl Ed), 2021, 112(1): 90-92. doi: 10.1016/j.ad.2019.05.009 .
doi: 10.1016/j.ad.2019.05.009 |
| [15] |
CHEN W, YOSHIDA S, MIURA N, et al. Efficacy of docetaxel addition to next-generation androgen receptor-axis-targeted therapies and androgen deprivation therapy in metastatic hormone-sensitive prostate cancer: A tumor volume-specific analysis[J]. Int J Urol, 2025,32(4): 361-370. doi: 10.1111/iju.15657 .
doi: 10.1111/iju.15657 |
| [16] |
PARIKH M, TANGEN C, HUSSAIN M H A, et al. Three- and seven-month prostate-specific antigen levels as prognostic markers for overall survival in metastatic hormone-sensitive prostate cancer: Results from SWOG S1216, a phase 3 randomized trial of androgen deprivation plus orteronel or bicalutamide[J]. Eur Urol Oncol, 2024, 7(5): 1097-1104. doi: 10.1016/j.euo. 2024. 03.001 .
doi: 10.1016/j.euo. 2024. 03.001 |
| [17] |
BIAN X, GU W, ZHANG X, et al. Correlation of PSA and survival in metastatic hormone-sensitive prostate cancer treated with rezvilutamide plus ADT in the CHART trial[J]. Med, 2025, 6(2): 100520. doi: 10.1016/j.medj.2024.09.009 .
doi: 10.1016/j.medj.2024.09.009 |
| [18] |
SINGH K. Rezvilutamide for metastatic castration-sensitive prostate cancer: CHART trial[J]. Indian J Urol, 2023,39(2): 171-172. doi: 10.4103/iju.iju_336_22 .
doi: 10.4103/iju.iju_336_22 |
| [19] |
ARMSTRONG A J, AZAD A A, IGUCHI T, et al. Improved survival with enzalutamide in patients with metastatic hormone-sensitive prostate cancer[J]. J Clin Oncol, 2022, 40(15): 1616-1622. doi: 10.1200/JCO.22.00193 .
doi: 10.1200/JCO.22.00193 |
| [20] |
HONG J, ZENG X, CHEN W, et al. Cost-effectiveness analysis of rezvilutamide versus bicalutamide and androgen-deprivation therapy in patients with high-volume, metastatic, hormone-sensitive prostate cancer: A markov's model-based evaluation[J]. Front Public Health, 2025, 13: 1574780. doi: 10.3389/fpubh.2025.1574780 .
doi: 10.3389/fpubh.2025.1574780 |
| [21] |
JIA A Y, SPRATT D E. Bicalutamide monotherapy with radiation therapy for localized prostate cancer: A non-evidence-based alternative[J]. Int J Radiat Oncol Biol Phys, 2022, 113(2): 316-319. doi: 10.1016/j.ijrobp.2022.01.037 .
doi: 10.1016/j.ijrobp.2022.01.037 |
| [22] |
GOLDBERG H, GLICKSMAN R, WOON D, et al. Can post-treatment free PSA ratio be used to predict adverse outcomes in recurrent prostate cancer?[J]. BJU Int, 2021, 127(6): 654-664. doi: 10.1111/bju.15236 . Epub 2020 Sep 26.
doi: 10.1111/bju.15236 |
| [23] |
DING H, LI S, XU X, et al. Cost-effectiveness analysis of rezvilutamide versus bicalutamide in the treatment of metastatic hormone-sensitive prostate cancer[J]. BMJ Open, 2024, 14(7): e073170. doi: 10.1136/bmjopen-2023-073170 .
doi: 10.1136/bmjopen-2023-073170 |
| [24] |
FAROKHI S, ROUSHANI M. Flower-like core-shell nanostructures based on natural asphalt coated with Ni-LDH nanosheets as an electrochemical platform for prostate cancer biomarker sensing[J]. Mikrochim Acta, 2023, 190(5): 198. doi: 10.1007/s00604-023-05779-y .
doi: 10.1007/s00604-023-05779-y |
| [25] |
ZHANG C, REN J, KANG Y, et al. Case report and literature review of rezvilutamide in the treatment of hormone-sensitive prostate cancer[J]. Front Oncol, 2024, 14: 1374039. doi: 10.3389/fonc.2024.1374039 .
doi: 10.3389/fonc.2024.1374039 |
| [26] |
NAH E H, CHO S, PARK H, et al. Establishment and validation of reference intervals for tumor markers (AFP, CEA, CA19-9, CA15-3, CA125, PSA, HE4, Cyfra 21-1, and ProGRP) in primary care centers in Korea: A cross-sectional retrospective study[J]. Health Sci Rep, 2023,6(2): e1107. doi: 10.1002/hsr2.1107 .
doi: 10.1002/hsr2.1107 |
| [27] |
崔英杰,张桂芳. 治疗转移性激素敏感性前列腺癌的第2代雄激素受体拮抗剂瑞维鲁胺[J]. 中国新药杂志, 2024, 33(20): 2109-2113. doi: 10.3969/j.issn.1003-3734.2024.20.005 .
doi: 10.3969/j.issn.1003-3734.2024.20.005 |
| [28] |
WU H, GONG M, YUAN R. Relationship between neutrophil-lymphocyte ratio (NLR) and platelet-lymphocyte ratio (PLR) in peripheral blood and prognosis after castration therapy for prostate cancer[J]. Indian J Cancer,2024, 61(1): 193-199. doi: 10.4103/ijc.ijc_211_24 .
doi: 10.4103/ijc.ijc_211_24 |
| [29] |
TAHSIN S, SANE N S, CERNYAR B, et al. AR loss in prostate cancer stroma mediated by NF-κB and p38-MAPK signaling disrupts stromal morphogen production[J]. Oncogene, 2024,43(27): 2092-2103. doi: 10.1038/s41388-024-03064-7 .
doi: 10.1038/s41388-024-03064-7 |
| [30] |
PENG S, ZHANG R, ZOU Z, et al.Real-world multicenter study of rezvilutamide plus androgen deprivation therapy in Chinese patients with high-volume metastatic hormone-sensitive prostate cancer[J]Front Oncol, 2025, 15: 1657772. doi: 10.3389/fonc. 2025.1657772 .
doi: 10.3389/fonc. 2025.1657772 |
| [31] |
LIN K L, TALMOR B, CRUMBAKER M, et al. A review of hot flash management in patients with prostate cancer[J]. J Clin Endocrinol Metab, 2025, 110(9): 2509-2519. doi: 10.1210/clinem/dgaf302 .
doi: 10.1210/clinem/dgaf302 |
| [32] |
TSUBOI I, SCHULZ R J, LAUKHTINA E, et al. Incidence, management, and prevention of gynecomastia and breast pain in patients with prostate cancer undergoing antiandrogen therapy: A systematic review and meta-analysis of randomized controlled trials[J]. Eur Urol Open Sci, 2025, 73: 31-42. doi: 10.1016/j.euros.2025.01.001 .
doi: 10.1016/j.euros.2025.01.001 |
| [33] |
IBÁÑEZ C, TOURÍS-LORES M, MONTESA Á, et al. Drug-drug interactions in metastatic hormone-sensitive prostate cancer (mHSPC): practical considerations for treating men with androgen receptor pathway inhibitors and common medications in this stage[J]. Expert Opin Drug Metab Toxicol, 2025, 21(6): 625-636. doi: 10.1080/17425255.2025.2478167 .
doi: 10.1080/17425255.2025.2478167 |
| [34] |
WU H, SUN L, FENG R, et al. Cost-effectiveness of rezvilutamide versus bicalutamide and androgen-deprivation therapy in patients with highvolume, metastatic, hormone-sensitive prostate cancer[J]. Front Pharmacol,2024, 14: 1269129. doi: 10.3389/fphar.2023.1269129 .
doi: 10.3389/fphar.2023.1269129 |
| [35] |
AZAD A A, PETRYLAK D P, IGUCHI T, et al. Enzalutamide and prostate-specific antigen levels in metastatic prostate cancer: A secondary analysis of the ARCHES randomized clinical trial[J]. JAMA Netw Open, 2025, 8(5): e258751. doi: 10.1001/jamanetworkopen.2025.8751 .
doi: 10.1001/jamanetworkopen.2025.8751 |
| [36] |
MORRIS M J, CASTELLANO D, HERRMANN K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naive patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomised, controlled trial[J]. Lancet,2024, 404(10459): 1227-1239. doi: 10.1016/S0140-6736(24)01653-2 .
doi: 10.1016/S0140-6736(24)01653-2 |
| [37] |
CHOWDHURY S, BJARTELL A, AGARWAL N, et al. Deep, rapid, and durable prostate-specific antigen decline with apalutamide plus androgen deprivation therapy is associated with longer survival and improved clinical outcomes in TITAN patients with metastatic castration-sensitive prostate cancer[J]. Ann Oncol, 2023, 34(5): 477-485. doi: 10.1016/j.annonc.2023.02.009 .
doi: 10.1016/j.annonc.2023.02.009 |
| [38] |
MOHAMMED NAWI A, MASDOR N A, OTHMAN R, et al. Survival rate and prognostic factors of localised prostate cancer in southeast asian countries: A systematic review with meta-analysis[J]. Asian Pac J Cancer Prev, 2023, 24(9): 2941-2095. doi: 10.31557/APJCP.2023.24.9.2941 .
doi: 10.31557/APJCP.2023.24.9.2941 |
| [39] |
LI L, ZHANG Q, WANG Y, et al. Evaluating the diagnostic and prognostic value of serum TuM2-PK, NSE, and ProGRP in small cell lung cancer[J]. J Clin Lab Anal, 2023, 37(7): e24865. doi: 10.1002/jcla.24865 . Epub 2023 Apr 23.
doi: 10.1002/jcla.24865 |
| [1] | 李唯尊,邢晨,安恒庆. STAT活化抑制蛋白2基因在前列腺癌中的表达水平及与临床病理特征的关系[J]. 实用医学杂志, 2025, 41(18): 2844-2852. |
| [2] | 刘俊志,邱磊,徐坤,刘建炜,胡德华,朱华,沈城,陆明,陈建刚. 系统性免疫炎症指数预测前列腺癌盆腔淋巴结转移列线图模型的建立[J]. 实用医学杂志, 2025, 41(15): 2349-2354. |
| [3] | 邵泓超,罗淇元,高文彬,罗文,叶木石. 白藜芦醇抑制前列腺癌生长及激素抵抗的体内实验[J]. 实用医学杂志, 2025, 41(12): 1835-1839. |
| [4] | 刘伟峰,戴政,周毅彬,封凯文,魏恺,孙古乐,阳东荣,朱进. 尿液蛋白激酶Y基因启动子位点甲基化在前列腺癌早期诊断中的价值[J]. 实用医学杂志, 2024, 40(5): 688-694. |
| [5] | 陈灿伟,廖壮文,范子文,黄帅,黄彦,陈斌伟. 溶酶体相关膜蛋白3通过VEGF/AKT通路抑制PC-3细胞增殖、转移及血管生成[J]. 实用医学杂志, 2024, 40(2): 182-187. |
| [6] | 黄敏玉,吴军,覃天资,周威,苏立泽,邱荣,黄璐. 血清DCLK1、sTim-3对前列腺癌根治术患者预后的评估价值[J]. 实用医学杂志, 2023, 39(18): 2368-2372. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||