

The Journal of Practical Medicine ›› 2025, Vol. 41 ›› Issue (22): 3544-3551.doi: 10.3969/j.issn.1006-5725.2025.22.011
• Clinical Research • Previous Articles
Ran LIU1,Dan CHEN2,Yingzhao QI1,Jiayu WANG1,Zhixin LIU1( )
)
Received:2025-07-22
Online:2025-11-25
Published:2025-11-26
Contact:
Zhixin LIU
E-mail:15803351940@163.com
CLC Number:
Ran LIU,Dan CHEN,Yingzhao QI,Jiayu WANG,Zhixin LIU. The efficacy of different surgical approaches in full⁃endoscopic treatment for degenerative lumbar lateral recess stenosis: A propensity score⁃matched cohort study[J]. The Journal of Practical Medicine, 2025, 41(22): 3544-3551.
Tab.1
Comparison of baseline data of patients between the two groups before matching"
| 基线特征 | 侧路组 (n = 34) | 后路组 (n = 44) | t/χ2 值 | P值 |
|---|---|---|---|---|
| 年龄/岁 | 65.76 ± 11.55 | 58.84 ± 16.15 | 2.113 | 0.038 |
| BMI/(kg/m2) | 22.15 ± 7.35 | 25.86 ± 8.51 | -2.024 | 0.046 |
| 性别/[例(%)] | 1.241 | 0.265 | ||
| 男 | 15(44.1) | 14(31.8) | ||
| 女 | 19(55.9 ) | 30(68.2) | ||
| 侧别/[例(%)] | 0.014 | 0.906 | ||
| 左 | 19(55.9) | 24(54.5) | ||
| 右 | 15(44.1) | 20(45.5) | ||
| 病程/周 | 12.51 ± 2.76 | 10.78 ± 3.56 | 2.341 | 0.022 |
| 糖尿病/[例(%)] | 9(26.5) | 14(31.8) | 0.264 | 0.607 |
| 吸烟史/[例(%)] | 8(23.5) | 9(20.5) | 0.106 | 0.745 |
Tab.2
Comparison of baseline data of patients between the two groups after matching"
| 基线特征 | 侧路组 (n = 25) | 后路组 (n = 25) | t/χ2 值 | P值 |
|---|---|---|---|---|
| 年龄/岁 | 62.59 ± 8.05 | 60.44 ± 9.15 | 0.882 | 0.382 |
| BMI/(kg/m2) | 22.80 ± 4.45 | 24.13 ± 4.51 | 1.049 | 0.299 |
| 性别/[例(%)] | 0.082 | 0.774 | ||
| 男 | 11(44.0) | 10(40.0) | ||
| 女 | 14(56.0 ) | 15(60.0) | ||
| 侧别/[例(%)] | 0.082 | 0.774 | ||
| 左 | 14(56.1) | 15(60.0) | ||
| 右 | 11(44.0) | 10(40.0) | ||
| 病程/周 | 10.41 ± 3.76 | 9.68 ± 3.96 | 0.668 | 0.507 |
| 糖尿病/[例(%)] | 7(28.0) | 8(32.0) | 0.095 | 0.758 |
| 吸烟史/[例(%)] | 6(24.0) | 7(28.0) | 0.104 | 0.747 |
Tab.3
The comparison of VAS scores between the two groups with low back pain"
| 时间点 | 侧路组(n = 25) | 后路组(n = 25) | 均值差(95%CI) | t值 | P值 |
|---|---|---|---|---|---|
| 术前 | 6.24 ± 0.97 | 6.57 ± 1.23 | -0.33(-0.96 ~ 0.30) | 1.05 | 0.297 |
| 术后3 d | 3.37 ± 0.85? | 3.27 ± 0.97? | 0.10(-0.42 ~ 0.62) | 0.39 | 0.700 |
| 术后3个月 | 2.56 ± 0.69? | 2.38 ± 0.75? | 0.18(-0.23 ~ 0.59) | 0.88 | 0.381 |
| 术后6个月 | 1.46 ± 0.83? | 1.19 ± 0.75? | 0.27(-0.18 ~ 0.72) | 1.21 | 0.233 |
| 术后1年 | 0.62 ± 0.58? | 0.51 ± 0.47? | 0.11(-0.19 ~ 0.41) | 0.74 | 0.465 |
Tab.4
The comparison of VAS scores between the two groups with leg pain"
| 时间点 | 侧路组(n = 25) | 后路组(n = 25) | 均值差(95%CI) | t值 | P值 |
|---|---|---|---|---|---|
| 术前 | 7.23 ± 1.06 | 6.95 ± 1.34 | 0.28(-0.41 ~ 0.97) | 0.82 | 0.417 |
| 术后3 d | 3.28 ± 0.87? | 3.18 ± 0.97? | 0.10(-0.42 ~ 0.62) | 0.38 | 0.702 |
| 术后3个月 | 2.76 ± 0.56? | 2.37 ± 0.85? | 0.39(-0.02 ~ 0.80) | 1.92 | 0.061 |
| 术后6个月 | 1.97 ± 0.57? | 1.63 ± 0.87? | 0.34(-0.08 ~ 0.76) | 1.63 | 0.109 |
| 术后1年 | 1.65 ± 0.87? | 1.48 ± 0.76? | 0.17(-0.29 ~ 0.63) | 0.74 | 0.465 |
Tab.5
Comparison of ODI scores assessments between the two groups"
| 时间点 | 侧路组(n = 25) | 后路组(n = 25) | 均值差(95%CI) | t值 | P值 |
|---|---|---|---|---|---|
| 术前 | 68.52 ± 9.45 | 67.69 ± 10.32 | 0.83(-4.79 ~ 6.45) | 0.30 | 0.768 |
| 术后3 d | 42.18 ± 8.67? | 44.68 ± 9.97? | -2.50(-7.81 ~ 2.81) | -0.95 | 0.349 |
| 术后3个月 | 25.20 ± 8.55? | 27.52 ± 9.33? | -2.32(-7.41 ~ 2.77) | -0.92 | 0.364 |
| 术后6个月 | 20.38 ± 8.71? | 21.86 ± 9.66? | -1.48(-6.71 ~ 3.75) | -0.57 | 0.572 |
| 术后1年 | 16.07 ± 8.11? | 16.97 ± 9.30? | -0.90(-5.86 ~ 4.06) | -0.36 | 0.717 |
Tab.6
Comparison of lumbar stability and lateral recess angle assessments between the two groups"
| 指标 | 时间点 | 侧路组(n = 25) | 后路组(n = 25) | 均值差(95%CI) | t值 | P值 |
|---|---|---|---|---|---|---|
| 过伸过屈角度/° | 术前 | 7.51 ± 3.57 | 6.87 ± 4.84 | 0.64(-1.78 ~ 3.06) | 0.53 | 0.597 |
| 术后3月 | 7.23 ± 2.57 | 7.57 ± 1.34 | -0.34(-1.51 ~ 0.83) | -0.59 | 0.561 | |
| LRA | 术前 | 32.50 ± 9.30 | 34.23 ± 7.86 | -1.73(-6.63 ~ 3.17) | -0.710 | 0.481 |
| 术后3 d | 69.86 ± 5.22* | 72.84 ± 6.07* | -2.98(-6.20 ~ 0.24) | -1.861 | 0.069 |
Tab.7
Comparison of perioperative parameters between the two groups"
| 指标 | 侧路组(n = 25) | 后路组(n = 25) | 均值差(95%CI) | t值 | P值 |
|---|---|---|---|---|---|
| 手术时间/min | 85.3 ± 16.4 | 80.8 ± 20.6 | 4.50(-6.09 ~ 15.09) | 0.855 | 0.397 |
| 术后住院时间/d | 7.5 ± 1.8 | 7.0 ± 2.1 | 0.50(-0.61 ~ 1.61) | 0.904 | 0.370 |
| C臂透视次数 | 5.6 ± 2.3 | 3.5 ± 1.8 | 2.10(0.93 ~ 3.27) | 3.595 | < 0.001 |

Fig.1
Typical case 1"
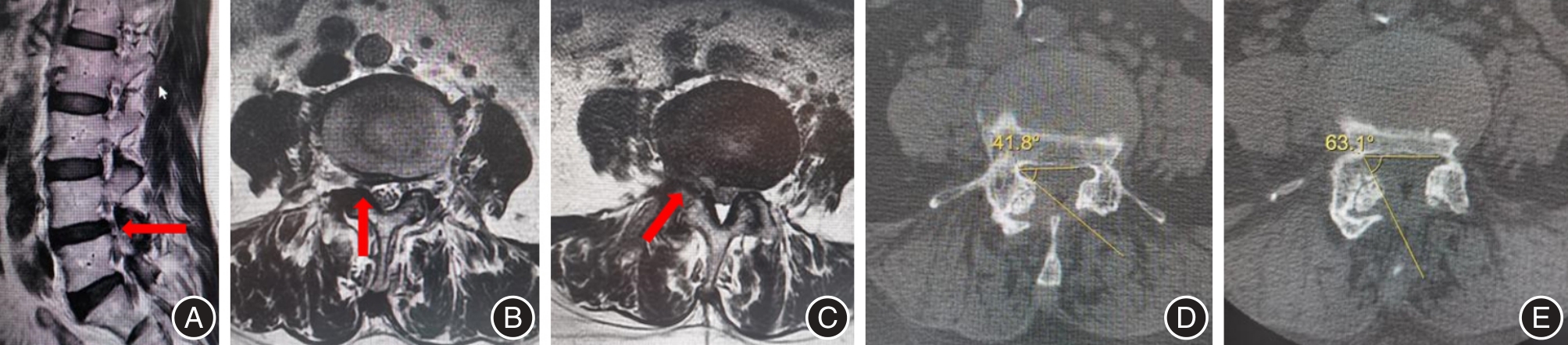

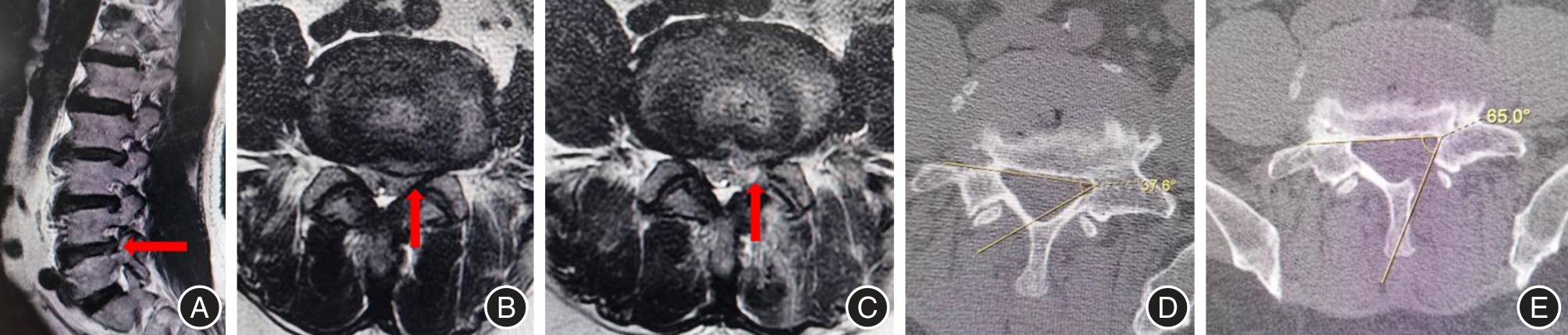
Fig.2
Typical case 2"
| [1] |
JENSEN R K, HARHANGI B S, HUYGEN F, et al. Lumbar spinal stenosis[J]. BMJ, 2021,373:n1581. doi:10.1136/bmj.n1581
doi: 10.1136/bmj.n1581 |
| [2] |
XIE P, FENG F, CHEN Z, et al. Percutaneous transforaminal full endoscopic decompression for the treatment of lumbar spinal stenosis[J]. BMC Musculoskelet Disord, 2020,21(1):546. doi:10.1186/s12891-020-03566-x
doi: 10.1186/s12891-020-03566-x |
| [3] |
KATZ J N, ZIMMERMAN Z E, MASS H, et al. Diagnosis and Management of Lumbar Spinal Stenosis: A Review[J]. JAMA, 2022,327(17):1688-1699. doi:10.1001/jama.2022.5921
doi: 10.1001/jama.2022.5921 |
| [4] | 王子桓, 张翼升, 余熙荣, 等. 单一切口椎间孔镜治疗双节段腰椎管狭窄合并腰椎间盘突出症的效果[J]. 实用医学杂志, 2025,41(1):41-47. |
| [5] |
LI K, ZHANG Z, RAN J, et al. Unilateral Endoscopic and Unilateral Biportal Endoscopic surgery for lumbar spinal stenosis: A systematic review and meta-analysis[J]. Front Surg, 2025,12:1585783. doi:10.3389/fsurg.2025.1585783
doi: 10.3389/fsurg.2025.1585783 |
| [6] | 廖军, 宗少晖, 陈晓明, 等. 经皮内镜后路腰椎间融合术与微创经椎间孔入路腰椎椎间融合术治疗腰椎管狭窄症的效果[J]. 实用医学杂志, 2022,38(17):2209-2215. |
| [7] | 中国医疗保健国际交流促进会骨科分会脊柱内镜学部, 中国医师协会骨科医师分会脊柱微创学组, 戎利民, 等. 脊柱内镜手术规范化命名的中国专家共识[J]. 中国脊柱脊髓杂志, 2024, 34(4): 444-448. |
| [8] |
GUNJOTIKAR S, PESTONJI M, TANAKA M, et al. Evolution, Current Trends, and Latest Advances of Endoscopic Spine Surgery[J]. J Clin Med, 2024,13(11):3208. doi:10.3390/jcm13113208
doi: 10.3390/jcm13113208 |
| [9] | 刁文博, 李文祥, 娄才立, 等. 对椎间孔分区方法在内镜下腰椎后外侧入路手术中应用的效果分析[J]. 骨科临床与研究杂志, 2024, 9(3): 163-169. |
| [10] | 蒋强,丁宇,卢正操,等. PE-MFD与Endo-LOVE治疗腰椎间盘突出症疗效比较[J].中国骨与关节损伤杂志, 2021,36(1):13-16. |
| [11] |
AUSTIN P C. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies[J]. Multivariate Behav Res, 2011, 46(3): 399-424. doi:10.1080/00273171.2011.568786
doi: 10.1080/00273171.2011.568786 |
| [12] |
WEINSTEIN J N, TOSTESON T D, LURIE J D, et al. Surgical versus Nonsurgical Therapy for Lumbar Spinal Stenosis[J]. N Engl J Med, 2008, 358(8): 794-810. doi:10.1056/nejmoa0707136
doi: 10.1056/nejmoa0707136 |
| [13] | 舒涛,吴帝求,沈茂. 不同微创椎管减压术在腰椎管狭窄症中的研究进展[J]. 中国修复重建外科杂志, 2023, 37(7): 895-900. |
| [14] |
JU C I, KIM P, HA S W, et al. Contraindications and Complications of Full Endoscopic Lumbar Decompression for Lumbar Spinal Stenosis: A Systematic Review[J]. World Neurosurg, 2022, 168: 398-410. doi:10.1016/j.wneu.2022.07.066
doi: 10.1016/j.wneu.2022.07.066 |
| [15] |
CHEN K T, CHOI K C, SHIM H K, et al. Full-endoscopic versus microscopic unilateral laminotomy for bilateral decompression of lumbar spinal stenosis at L4-L5: Comparative study[J].Int Orthop, 2022, 46(12): 2887-2895. doi:10.1007/s00264-022-05549-0
doi: 10.1007/s00264-022-05549-0 |
| [16] |
LIANG X, RAN L, ZHAI N, et al. Application of Repeated Foraminoplasty in Percutaneous Endoscopic Transforaminal Discectomy for Lumbar Disc Herniation Patients with Lumbar Foraminal Stenosis.[J]. World Neurosurg, 2025, 195: 123647. doi:10.1016/j.wneu.2024.123647
doi: 10.1016/j.wneu.2024.123647 |
| [17] |
LIANG M, WANG Y, JIANG Y, et al. Clinical Efficacy of Interlaminar and Transforaminal Spinal Endoscopy in the Treatment of Lumbar Spinal Stenosis[J].Clin Interv Aging, 2023, 18: 881-890. doi:10.2147/cia.s406566
doi: 10.2147/cia.s406566 |
| [18] |
YU L, DONG H, TAN H, et al. Uniportal Full-endoscopic Foraminotomy for Lumbar Foraminal Stenosis: Clinical Characteristics and Functional Outcomes[J]. Orthop Surg, 2024,16(8): 1861-1870. doi:10.1111/os.14102
doi: 10.1111/os.14102 |
| [19] |
LEWANDROWSKI K U, DOWLING Á, DE CARVALHO P S T, et al. Indication and Contraindication of Endoscopic Transforaminal Lumbar Decompression.[J]. World Neurosurg, 2021, 145: 631-642. doi:10.1016/j.wneu.2020.03.076
doi: 10.1016/j.wneu.2020.03.076 |
| [20] |
LIU J, KONG Q, MA J, et al. Comparison of clinical efficacy between Percutaneous Endoscopic Large channels nerve decompression through Translaminar approach and Percutaneous Endoscopy Conventional channels nerve decompression through Transforaminal approach for the treatment of degenerative L4/5 spinal stenosis: A retrospective study[J]. BMC Musculoskelet Disord, 2025, 26(1): 493. doi:10.1186/s12891-025-08623-x
doi: 10.1186/s12891-025-08623-x |
| [21] |
ZOU H J, HU Y, LIU J B, et al. Percutaneous Endoscopic Transforaminal Lumbar Discectomy via Eccentric Trepan foraminoplasty Technology for Unilateral Stenosed Serve Root Canals[J]. Orthop Surg, 2020, 12(4): 1205-1211. doi:10.1111/os.12739
doi: 10.1111/os.12739 |
| [22] |
KISHIMA K, YAGI K, YAMASHITA K, et al. Transforaminal Full-Endoscopic Ventral Facetectomy: Midterm Results and Factors Associated with Poor Surgical Outcomes.[J]. J Neurol Surg A Cent Eur Neurosurg, 2024,85(2): 155-163. doi:10.1055/a-1995-1772
doi: 10.1055/a-1995-1772 |
| [23] | 刘学光, 孙振中. 全内镜下手术治疗高度移位型腰椎间盘突出症的研究进展[J]. 中国脊柱脊髓杂志, 2023, 33(6): 564-569. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||